



PEER REVIEWED
Optic Neuritis Associated with Multiple Sclerosis:
a Teaching Case Report
Betty Wang, OD, FAAO, and Callista Belles, OD
Abstract
Optic neuritis is an inflammatory demyelination of the optic nerve that is highly associated with multiple sclerosis (MS). Optic neuritis is the presenting feature in up to 20% of MS patients and occurs in up to 50% of patients with MS. The condition occurs more commonly in women than in men and occurs between the ages of 20 and 50. The two most common symptoms of optic neuritis are vision loss and eye pain. Signs of optic neuritis include decreased visual acuity, an afferent pupillary defect, abnormal color vision, visual field defects and reduced contrast sensitivity. One-third of patients have visible optic nerve inflammation and two-thirds have a normal-appearing optic nerve known as retrobulbar optic neuritis. The Optic Neuritis Treatment Trial (ONTT) showed that high-dose intravenous corticosteroid treatment is beneficial for acute attacks and that oral corticosteroid alone is contraindicated due to increased risk of recurrence. Gadolinium contrast-enhanced magnetic resonance imaging (MRI) of the brain and orbits confirms optic neuritis, and baseline MRI findings are an important predictor of the risk of future recurrence.
Key Words: optic neuritis, multiple sclerosis, inflammatory demyelination, the Optic Neuritis Treatment Trial (ONTT), Uhthoff’s phenomenon, gadolinium contrast-enhanced brain MRI
Background
Optic neuritis is an acute inflammatory demyelinating injury to the optic nerve. Optic neuritis is the presenting feature in up to 20% of multiple sclerosis (MS) patients and occurs in up to 50% of MS patients at some point during their lifetime. The two most common symptoms of acute optic neuritis are vision loss and eye pain. Optic nerve edema is seen in one-third of MS patients, and two-thirds of patients have a normal optic nerve appearance, known as retrobulbar optic neuritis. Gadolinium contrast-enhanced magnetic resonance imaging (MRI) of the brain and orbits, showing hyperintense white matter abnormalities, is used for diagnosis. In the Optic Neuritis Treatment Trial (ONTT), intravenous corticosteroids accelerated visual recovery and oral corticosteroids alone did not improve visual outcome and were associated with an increased rate of optic neuritis recurrence. Baseline gadolinium contrast-enhanced MRI of the brain and orbits is an essential tool for the diagnosis and management of optic neuritis and also serves as a predictor of recurrent episodes. Chronic features of optic neuritis include reduced visual acuity, color desaturation, optic atrophy and visual field loss.
The patient in this case report presented to clinic reporting acute onset of blurred vision, blind spots and halos in the left eye. Although his visual acuity and color vision remained normal, he had a new visual field defect in the left eye and optic nerve swelling. The patient was promptly treated with a four-day course of intravenous corticosteroids. At the two-week follow-up exam, his symptoms and visual field defect were resolved. For prompt evaluation and treatment, it is crucial for eye physicians to educate patients with a history of MS on the symptoms and signs of optic neuritis.
Student Discussion Guide
Case presentation
A 38-year-old Caucasian male presented to the Orlando VA Eye Clinic on Oct. 24, 2017, for a scheduled six-month ocular health exam and follow-up on MS with no history of optic neuritis. The patient reported no changes in vision since his previous eye exam on June 22, 2017. He stated that he still saw blue rings in both eyes two to three times a week and experienced occasional blurred vision following exercise or hot showers, which was reported at his last eye exam. The patient’s ocular history included dry eye syndrome OU, forme fruste keratoconus OD, early cataracts OU, lattice degeneration with atrophic retinal holes OU, and MS with no history of optic neuritis. However, the patient did experience Uhthoff’s symptoms of blue rings in vision when overheated or after exercise. The patient was diagnosed with MS in 2014, which was managed by the VA neurology clinic. His most recent brain MRI without contrast was on June 14, 2017, consistent with the clinical impression of MS with presence of infratentorial and supratentorial lesions. The scan was stable with no interval development of new lesions from his prior brain MRI on Jan. 7, 2016. His systemic medications for MS included dimethyl fumarate (Tecfidera) 240 mg twice a day, aspirin 325 mg once a day and Vitamin D3 1000 IU supplement twice a day. The patient’s systemic health was otherwise unremarkable. The only ocular medication used was artificial tears two to four times a day as needed for dry eye symptoms.
Visual acuity in the right eye was 20/25 due to mild keratoconus, which was stable, and 20/20 in the left eye. Pupils were equal, round and reactive to light without a relative afferent pupillary defect (APD). Confrontation visual fields and extra ocular motility testing were normal in both eyes. Color vision tested with the Farnsworth Panel D-15 was normal in each eye. Anterior segment exam showed mild corneal thinning of the right eye but was otherwise unremarkable in both eyes. Intraocular pressure was 12 mmHg in each eye. Anterior cortical lenticular changes were present in both eyes. The optic nerves of both eyes were healthy with no edema or pallor; a positive spontaneous venous pulsation was present. Optic nerve glial tissue was present in both eyes (Figure 1). The cup to disc ratio was 0.35 in the right eye and 0.25 in the left eye. Peripheral retinal lattice with atrophic holes was present in both eyes and was stable from the patient’s prior dilated fundus exam. Optical coherence tomography (OCT) of the retinal nerve fiber layer (RNFL) was performed (Spectralis, Heidelberg Engineering). The RNFL was normal in all quadrants and sectors compared to age-matched normative data and stable to the scan obtained at the prior visit (Figure 2). Humphrey visual field 24-2 SITA Standard testing was completed prior to pupil dilation and revealed a full field in each eye (Figure 3).
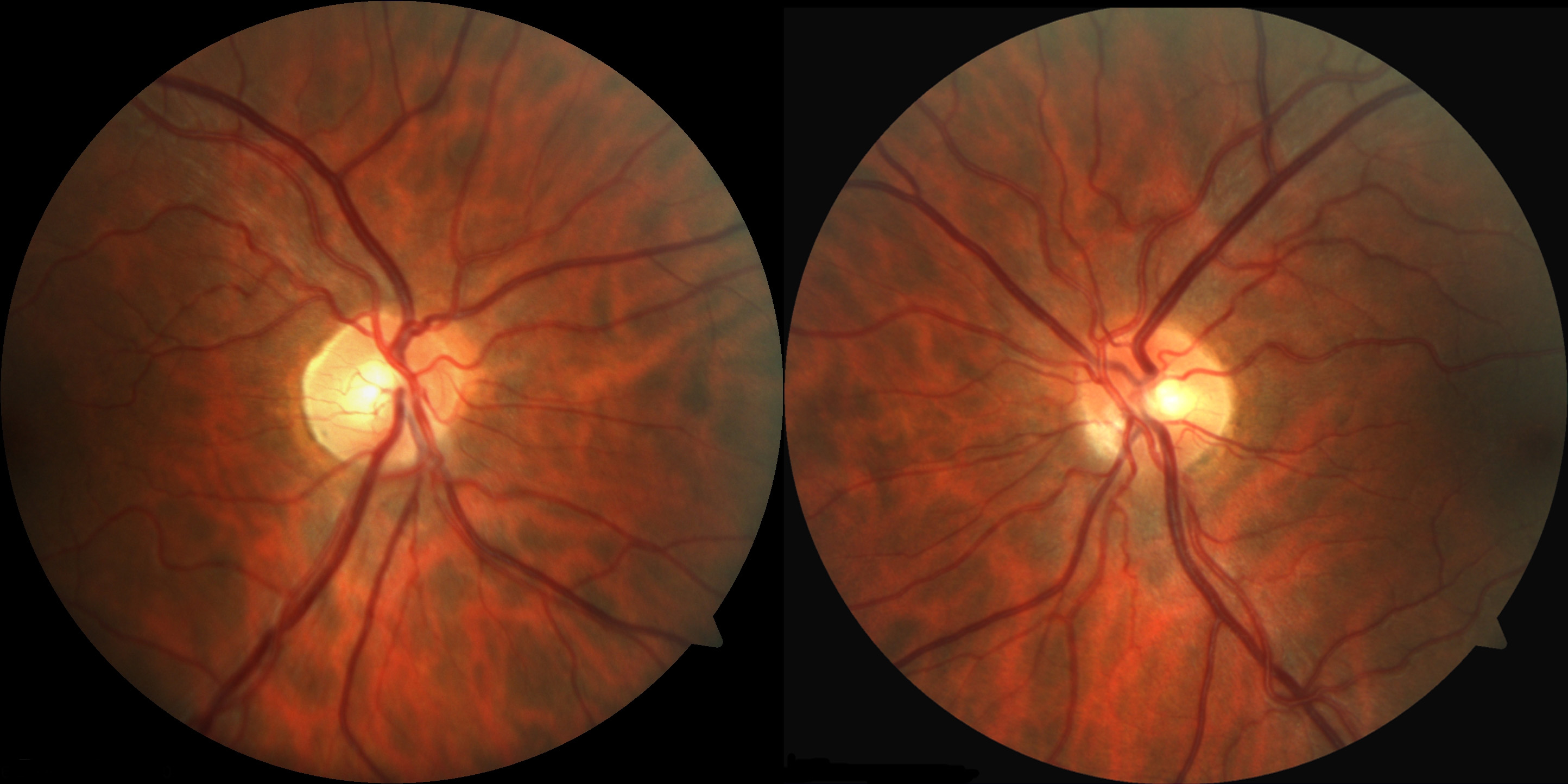 Figure 1. Optic nerve photographs of the right eye and left eye. |
 Figure 2. OCT of the retinal nerve fiber layer. |
 Figure 3. Humphrey 24-2 SITA Standard visual field test of the left eye and right eye. |
The patient was informed of stable clinical optic nerve findings with no signs of optic neuritis. He was advised to follow-up with his neurologist as scheduled on Feb. 26, 2018, and to return to the eye clinic in six months for a follow-up. He was educated on the symptoms of acute optic neuritis and instructed to return to clinic immediately if any acute eye pain, vision loss or other acute changes in vision occured prior to his next appointment.
Follow-up #1
The patient returned to clinic 10 days later, on Nov. 3, 2017, as an urgent care walk-in reporting acute onset of blurred vision, blind spots and halos in the left eye, which started one day prior. He verified no vision loss and no eye pain associated with his symptoms.
Visual acuity remained stable at 20/25 in the right eye and 20/20 in the left eye. Pupils were equal, round and reactive to light without a relative APD. Confrontation visual fields and extra ocular motility testing were normal in both eyes. There was no pain with eye movement. D15 color vision testing was repeated and remained normal in each eye. Humphrey visual field 24-2 SITA Standard was completed on the left eye only and showed a new superior cluster of points appearing as a vertical line just temporal from center (Figure 4). The mean deviation and pattern standard deviation worsened since the visual field test on October 24, 2017. The mean deviation was reduced from -0.28 to -3.96 decibels, and the pattern standard deviation increased from 1.07 to 2.22 decibels (Figure 4). Due to time constraints on the day of this urgent care visit, a second visual field test of the left eye was not completed to determine repeatability of the new field defect.
 Figure 4. Humphrey 24-2 SITA Standard visual field test of the left eye on Nov. 3, 2017 (left) compared to Oct. 24, 2017 (right). |
 Figure 5. Optic nerve photos of the right eye and left eye at the first follow-up visit. |
 Figure 6. OCT of the retinal nerve fiber layer of the left eye. The thicker black line corresponds to the scan on Nov. 3, 2017. The thinner grey line corresponds to the baseline scan. |
 Figure 7. OCT of the retinal nerve fiber layer of the right and left eye. Note the asymmetry of the inferior quadrant and inferior temporal sector showing thicker retinal nerve fiber layer in the left eye, particularly the 38-micron difference in the inferior temporal sector. |
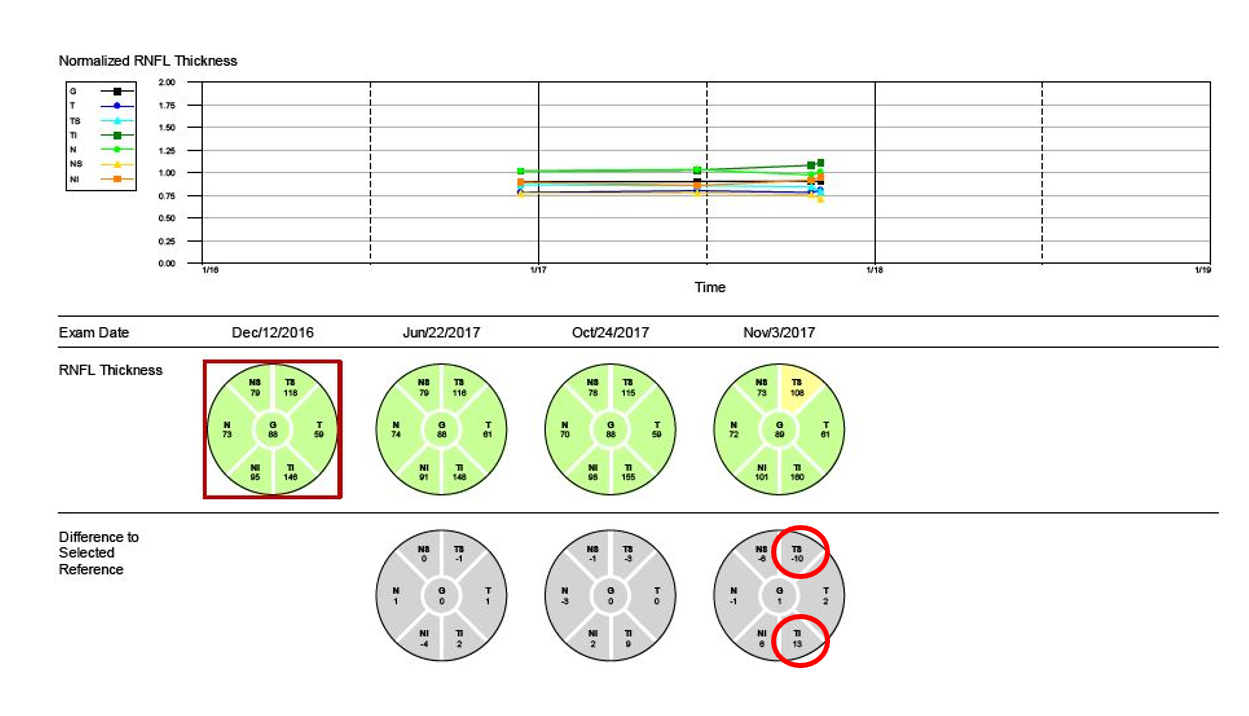 Figure 8. OCT retinal nerve fiber layer progression report for the left eye. |
 Figure 9. MRI of the brain with and without contrast showing new intracranial white matter T2 hyperintensities. |
Anterior segment exam was significant for mild corneal thinning in the right eye, which was noted at the patient’s previous visit and stable. All other anterior segment findings were normal. Intraocular pressure was 11 mmHg in the right eye and 14 mmHg in the left eye. Optic nerve evaluation was unremarkable in the right eye (Figure 5). The left optic nerve showed blurring of the disc margin from 6-11 o’clock and mild sectoral disc edema with associated elevation of the RNFL in the inferior quadrant (Figure 5). The cup to disc ratio was 0.35 in the right eye and 0.25 in the left eye. Both optic nerves were pink and showed a spontaneous venous pulse. There were no hemorrhages in either eye. The glial tissue inferior nasal in the left eye was previously noted.
OCT of the RNFL of the left eye showed a decrease in thickness compared to baseline in the superior temporal sector and a slight increase compared to baseline and the Oct. 24, 2017, scan in the inferior temporal sector (Figure 6). Comparison of OCT of the RNFL in the right and left eye showed asymmetry inferior showing thicker RNFL in the left eye than right, particularly in the inferior temporal sector where there was a 38-micron difference between the eyes (Figure 7). The RNFL progression report for the left eye showed an increase of 13 microns in the inferior temporal sector and a decrease of 10 microns in the superior temporal sector from baseline 11 months prior (Figure 8). The increased thickness of the inferior temporal sector correlated to both the clinical exam showing mild disc edema inferior and a new superior visual field defect.
The differential diagnoses for the findings of acute unilateral sectoral disc edema with an associated visual field defect were non-arteritic anterior ischemic optic neuropathy, Leber’s hereditary optic neuropathy, compressive optic neuropathy, inflammatory, infectious, infiltrative optic neuropathies, and acute optic neuritis associated with MS.
Based on the patient’s presenting symptoms of blurred vision, blind spots and halos in the left eye, history of MS and clinical exam findings of a new superior visual field defect that corresponded to inferior optic nerve edema seen clinically and confirmed with OCT, the patient was diagnosed with acute optic neuritis of the left eye associated with MS. The on-call neurologist was contacted to discuss the case, and the patient was directed to the Orlando Lake Nona VA emergency department for additional lab testing, brain MRI and possible admission for intravenous steroids.
The patient was evaluated at the Lake Nona emergency department that afternoon. Additional laboratory testing included erythrocyte sedimentation rate, complete blood count and c-reactive protein, all of which were within normal ranges. MRI of the brain with and without contrast was performed and showed new intracranial white matter T2 hyperintensities as well as scattered foci of enhancement consistent with active and new demyelination superimposed on a background of MS (Figure 9). MRI of the orbits showed normal optic nerves in both eyes, which were symmetrical in size and signal. The patient was admitted for a course of intravenous methylprednisolone (Solumedrol) 1 gram daily for four days. He was discharged on Nov. 7, 2017, in stable condition, and he reported that his blurred vision, blind spots and halos were improving. The neurologist and hospitalist recommended the patient follow-up with the eye clinic in one to two weeks and continue his current medications (Tecfidera 240 mg twice a day, aspirin 325 mg once a day and Vitamin D3 1000 IU supplement twice a day).
Follow-up #2
The patient returned to the eye clinic on Nov. 17, 2017, for a follow-up visit reporting that his symptoms of blurred vision, blind spots and halos resolved three days after being discharged with no recurrence. Visual acuity remained stable at 20/25 in the right eye and 20/20 in the left eye. Pupils were equal, round and reactive to light without a relative APD. Humphrey visual field 24-2 SITA Standard testing was completed prior to dilation and revealed a full field in each eye (Figure 10). The visual field defect in the left eye noted on Nov. 3, 2017, was resolved.
 Figure 10. Humphrey 24-2 SITA Standard visual field test of the left eye and right eye at the second follow-up visit. Click to enlarge |
 Figure 11. Optic nerve photos of the right eye and left eye at the second follow-up visit. |
 Figure 12. OCT retinal nerve fiber layer progression report for the left eye at the second follow-up visit. |
Anterior segment examination of both eyes revealed no changes since the prior visit. Intraocular pressure was 10 mmHg in right eye and 11 mmHg in the left eye. Optic nerve evaluation remained unremarkable in the right eye, and the left optic nerve showed residual sectoral edema inferior (Figure 11). The cup to disc ratio was stable, 0.35 in the right eye and 0.25 in the left eye. The OCT RNFL progression report showed the thickness of the inferior temporal quadrant on Nov. 17, 2017, was reduced compared with Nov. 3, 2017, and had returned to within 1 micron of the thickness compared with Oct. 24, 2017 (Figure 12). The RNFL thickness changes measured by OCT correlated with the clinical optic nerve evaluation and visual field test results for the left eye as well as with the patient’s symptoms.
The patient was informed of the improved optic nerve and visual field findings for his left eye. He was advised to follow-up with his neurologist as scheduled on Feb. 26, 2018, and to return to the eye clinic in six weeks for a follow-up exam. He was reminded about the symptoms of acute optic neuritis, informed that the condition could return, and instructed to return to clinic immediately if any acute eye pain, vision loss or other acute changes in vision occured prior his next appointment.
Key concepts
- Optic neuritis is an acute inflammation of the optic nerve that is typically monocular and presents with sudden vision loss and eye pain
- Optic neuritis is the presenting feature in up to 20% of MS patients and occurs in up to 50% of MS patients
- In the ONTT, one-third of patients were found to have signs of optic nerve inflammation; two-thirds of patients had a normal optic nerve appearance, known as retrobulbar optic neuritis
- The ONTT showed that high-dose intravenous corticosteroid treatment is beneficial for acute attacks and that oral corticosteroid alone is contraindicated due to increased risk of recurrence
- Gadolinium contrast-enhanced MRI of the brain and orbits provides confirmation of optic neuritis, and baseline MRI findings are an important predictor of the future risk of MS
- With prompt and appropriate detection, treatment and referral, eye physicians can play a significant role in reducing the risk of permanent vision impairment associated with optic neuritis
Learning objectives
- To define optic neuritis, list etiologies of the disease and understand its association with MS
- To gain knowledge about the signs and symptoms of optic neuritis associated with MS
- To gain insight into the optometrist’s role in the management and follow-up of patients with MS, the importance of regular dilated eye exams, and the incorporation of additional testing and imaging including visual fields, color vision, optic nerve photographs and RNFL OCT
- To describe the main findings of the ONTT and their relevance to the management and treatment of optic neuritis associated with MS
- To gain knowledge about contrast-enhanced brain MRI findings in the diagnosis of MS and optic neuritis, and to predict the risk for future recurrence as found in the ONTT
- To understand the importance of educating MS patients on the signs and symptoms of acute optic neuritis and the need for prompt evaluation and treatment to prevent optic nerve and RNFL damage, which can lead to permanent vision loss
Discussion questions
1. Background knowledge of optic neuritis and MS
- Define optic neuritis and MS
- List the etiologies for optic neuritis
- Explain the pathogenesis of optic neuritis in MS
- In the ONTT what were the two most common symptoms reported?
- Discuss the clinical signs of optic neuritis and the additional tests and imaging needed for diagnosis
- Discuss the chronic features of optic neuritis
- What were the significant findings of the ONTT for treatment of optic neuritis?
- Explain why oral corticosteroids alone are contraindicated for the treatment of acute optic neuritis
- Explain the need for prompt referral and treatment of optic neuritis
- Discuss the correlation between brain lesions on MRI and the risk of developing MS at 5, 10 and 15 years as found in the ONTT study
2. Primary care optometrist’s role in the management of this patient with MS
- Discuss the role of the optometrist in co-managing patients with MS with and without a history of optic neuritis
- Discuss the importance of a baseline dilated eye exam and regular follow-up exams in patients with MS
- List the additional tests, retinal and/or optic nerve imaging, and scans that can be obtained as part of the eye evaluation for patients with MS
- What signs and symptoms of acute optic neuritis should the optometrist include in patient education/discussions; how soon should patients be seen if they are experiencing acute symptoms?
- Explain the appropriate time frame for referral and treatment of patients with acute optic neuritis
3. Critical-thinking questions
- How frequently should MS patients with or without a history of optic neuritis have dilated eye exams?
- Should baseline visual fields, color vision testing, optic nerve photos and/or RNFL OCT scans be obtained on MS patients with no prior history of optic neuritis; how frequently should these additional tests be repeated?
- In this case, the patient presented with a complaint of sudden blind spots and halos with no vision loss or eye pain: If you were the optometrist managing this case, would you have evaluated the patient the same day; what additional tests would you have ordered at this visit?
- If a patient is diagnosed with acute optic neuritis, to whom and to where should the optometrist refer the patient for prompt treatment?
Educator’s Guide
The educator’s guide includes the information necessary for discussing the case. This teaching case report is appropriate for optometry students, residents and practicing optometrists. Optometrists serve a crucial role in co-managing patients with MS with and without a history of optic neuritis and can prevent permanent vision loss with prompt diagnosis and immediate referral for treatment. OCT of the RNFL is used routinely to detect and manage retinal and optic nerve disorders, but is also useful in the management of neurological conditions such as MS. This case report discusses the role of OCT in monitoring MS, which is relevant to the clinical training of optometry students and residents.
Optic neuritis associated with multiple sclerosis
Optic neuritis is defined as acute inflammation of the optic nerve that is typically monocular and presents with sudden vision loss and eye pain.1,2 The etiologies of acute optic neuritis include demyelinating diseases (MS), viral infections, inflammation of the orbit or sinuses and granulomatous inflammatory conditions (sarcoidosis, tuberculosis, and syphilis). It is highly associated with MS, which is a demyelinating disease of the central nervous system. In up to 20% of MS patients, optic neuritis is the initial presenting manifestation and has been shown to occur in up to 50% of patients during their disease course.3 The patient in this case report was diagnosed with MS in 2014 with no history of optic neuritis.
Optic neuritis associated with demyelinating disease occurs more commonly in women, at 75% compared to 25% in men, which closely matches the epidemiology of MS. The condition occurs between ages 20 and 50 with a peak age of onset between 30 and 40 years.4 Geographically, the incidence is higher in northern areas such as the northern United States and Eastern Europe and lowest in areas closer to the equator. The annual incidence of optic neuritis in the United States has been reported as high as 6.4 per 100,000.5
Pathophysiology of optic neuritis
The pathophysiological changes that cause inflammatory demyelination in optic neuritis are comparable to the processes in MS. Inflammation causes edema in myelinated nerve fibers and retinal vessel endothelial tissue, which leads to myelin damage and breakdown. Clinically, these changes manifest as retinal nerve fiber swelling, optic nerve swelling and retinal vein sheathing.6 The exact mechanism and target antigen that causes inflammatory demyelination in optic neuritis is unknown; however, it is hypothesized that the process is immune-mediated with T- and B-cell activation. Studies have shown systemic T-cell activation at symptom onset and B-cell activation in cerebrospinal fluid of optic neuritis patients.7,8
Clinical presentation of optic neuritis
Acute optic neuritis typically presents as monocular vision loss and eye pain. In the ONTT, which involved 457 patients age 18-46 with acute unilateral optic neuritis, vision loss and eye pain were the two most common symptoms reported.9 More than 90% of patients in the ONTT reported a decrease in central visual acuity. Vision loss occurred over a period of hours to several days and peaked between one and two weeks after symptom onset. The severity of vision loss was dependent on the area of central visual field affected. Visual acuities ranged significantly from 20/20 in 11% of patients to no light perception in 3% of patients; however, the majority of visual acuities ranged from 20/25 to 20/190. The median visual acuity was 20/60. Eye pain that increased with eye movement occurred in 92% of patients in the ONTT.9
The patient presented in this case experienced blind spots in vision of the left eye but maintained a best-corrected central visual acuity of 20/20 with no associated eye pain. Additional visual symptoms associated with optic neuritis include photopsia (reported in 30% of patients in the ONTT),9 changes in color perception and peripheral visual field loss. Blurred vision, flashing/flickering lights, blind spots and other visual disturbances can be precipitated by the patient becoming overheated, which is known as Uhthoff’s phenomenon. The photopsia reported in 30% of patients in the ONTT frequently occurred with eye movement.9 The patient in this case had a history of Uhthoff’s phenomenon-like symptoms and reported sudden blurred vision, blind spots and halos in the left eye the day he was diagnosed with acute optic neuritis.
In cases of monocular optic neuritis, several studies have shown deficits in visual acuity, visual field, color vision and contrast sensitivity in the contralateral eye with no reported symptoms.10,11 In a prospective study, Beck et al. investigated visual abnormalities of the contralateral eye in 448 eligible patients from the ONTT. They found that 67% of patients demonstrated a visual deficit in at least one of four parameters tested: visual acuity, visual field, color vision and contrast sensitivity. Abnormalities in the fellow eye were found on measurement of visual acuity in 13.8%, contrast sensitivity in 15.4%, color vision in 21.7%, and visual field in 48% of patients.10
Clinical signs of acute optic neuritis include reduced visual acuity, APD if the contralateral eye is unaffected, abnormal color vision, reduced contrast sensitivity, visual field defect, optic nerve inflammation, which can present as optic nerve edema, hyperemia and blurred disc margins, and optic nerve hemorrhages. In the ONTT, one-third of patients were found to have signs of optic nerve inflammation. Two-thirds of patients had retrobulbar optic neuritis with a normal optic nerve appearance. Retrobulbar optic neuritis is inflammation posterior to the globe without clinical optic nerve edema.9 In addition to demyelinating diseases such as MS, retrobulbar optic neuritis can be secondary to systemic lupus erythematosus, infections such as syphilis, or granulomatous inflammatory conditions such as sarcoidosis or Wegener’s granulomatosis.12 RNFL thickness measured by OCT shows thinning in 85% of optic neuritis cases.13 Abnormal color vision was found in 88% of cases tested with Ishihara plates and in 94% of cases tested with the Farnsworth-Munsell 100 hue test. Prior to the ONTT, an isolated central scotoma was thought to be the visual field defect typically associated with acute optic neuritis.14 However, only 8% of patients in the ONTT had a central scotoma defect based on the Humphrey 30-2 threshold automated perimetry test. Diffuse depression was most common, occurring in 48% of patients, followed by altitudinal defects, which occurred in 15% of patients. Fang et al. investigated visual field defects associated with optic neuritis using the database of the 457 patients in the ONTT and concluded that visual field abnormalities including localized altitudinal, central or cecocentral, or quadrant defects extended throughout the 30 degrees of the visual field tested and that optic neuritis does not preferentially affect one visual field location. Instead, the condition is a diffuse process that affects more than one group of axons and therefore causes a diffuse depression of the visual field.15 The patient presented in this case had a depressed total deviation and a superior cluster defect appearing as a vertical line just temporal from center on pattern deviation, which correlated with inferior optic nerve edema that was not noted on his normal visual field ten days prior.
Chronic features and complications of optic neuritis
Chronic features of optic neuritis include color desaturation, optic atrophy, visual field loss, Uhthoff’s phenomenon and a delayed pattern-shift visual evoked response. A relative APD remains in approximately one-fourth of patients two years after presentation.11 The prognosis for visual acuity is relatively favorable. Beck et al. found that nearly all patients recovered one line of acuity or better after three weeks, and median acuity at six months was 20/16.16 At the five-year follow-up in the ONTT, 87% of patients had a visual acuity of 20/25 or better. Patients can experience deficits in color vision, contrast sensitivity and perception of light brightness years after resolution of optic neuritis.9 The National Eye Institute Visual Function Questionnaire was administered to 244 ONTT patients five to eight years after treatment for optic neuritis to assess perceived health-related quality of life and visual impairment. They scored lower compared with the disease-free reference group in nearly all categories including general health, general vision, ocular pain, driving ability, color vision, peripheral vision, social functioning, mental health and dependency.17
The role of OCT for the clinical monitoring of multiple sclerosis and optic neuritis
OCT is a non-invasive imaging technique that has become an essential tool in managing neuro-ophthalmologic conditions, including MS and optic neuritis. The pathogenesis of demyelination in MS contributes to axonal loss and thinning of the RNFL and ganglion cell layer, which can be quantified by OCT. OCT is a highly sensitive and reliable method for evaluating changes in the RNFL and ganglion cell layer in optic neuritis. In 1999, Parisi et al. were the first to publish a study that found significant decreases in average RNFL thickness and temporal RNFL thickness as measured by OCT in optic neuritis patients at one-year follow-up. RNFL thinning was also seen in MS patients who did not have optic neuritis compared with controls.18,19 OCT can also detect subclinical axonal loss in patients with normal visual acuity and normal visual fields.18 Klinstorner et al.’s study of patients with unilateral optic neuritis and MS showed RNFL thinning as measured by OCT in 85% of cases.13 In the acute phase of optic neuritis, OCT can help to confirm optic nerve swelling with an increase in thickness, which would be followed by axonal loss and thinning.19

Figure 13. OCT provides quantitative information useful for monitoring retinal nerve fiber layer changes in optic neuritis. In this patient, significant changes were seen between October 24 and November 3.
Click to enlarge
This case is an example of how OCT is used for quantitative evaluation of RNFL changes in optic neuritis. OCT of the RNFL was obtained at each follow-up visit. When the patient presented with acute optic neuritis on Nov. 3, 2017, OCT showed RNFL changes consistent with the clinical exam findings of optic nerve and RNFL swelling. The inferior temporal sector showed a 13-micron increase from baseline. The superior temporal sector showed a 10-micron decrease, which represents axonal damage/thinning, which has been shown in literature to occur in patients with optic neuritis in the non-acute phase. These changes were shown throughout the patient’s follow-up visits, but the significant decrease was seen from Oct. 24 to Nov. 3, 2017 (Figure 13).
A recent study published in Neurology by Ratchford et al. of 164 patients with MS showed thinning of the ganglion cell/inner plexiform (GCIP) layer and RNFL compared to healthy control patients. The study also found that the rate of GCIP layer thinning was significantly higher in MS patients compared to control patients and therefore is more associated with clinical measures of MS progression.20
One limitation of this teaching case report is that OCT of the ganglion cell layer was not obtained during the course of follow-up. Given recent literature supporting the value of ganglion cell layer OCT in monitoring the axonal integrity of MS patients with and without a history of optic neuritis, this scan will be completed at his future visits and for other patients with MS. OCT is now considered an essential tool in assessing the disease activity in MS and optic neuritis and has been used in most recent MS clinical trials. The authors recommend that MS patients have baseline OCT scans of the RNFL and the ganglion cell layer, which should be repeated yearly along with dilated clinical evaluations of the optic nerve and RNFL. Dilation and repeat OCT scans of the RNFL and ganglion cell layer should be completed sooner if the patient reports any visual changes or if MRI reveals new demyelinating lesions.
MRI of the brain with gadolinium contrast enhancement for diagnosis and management
MRI of the brain with gadolinium contrast enhancement is a key tool to aid in the diagnosis of optic neuritis. Inflammation of the optic nerve manifests as a hyperintense signal with contrast-enhanced MRI.21 The hyperintense signal, consistent with demyelination, is seen in approximately 95% of optic neuritis patients and can persist for a mean of 30 days after onset.22,23 Optic nerve signal abnormalities can remain after recovery in vision and are present in up to 60% of patients with MS with no history of optic neuritis.23 White matter lesions of the brain seen on MRI are typically larger than 3 mm, ovoid and periventricular. In the ONTT, approximately 40% of patients had MRI lesions.9 A study conducted by Dalton et al. involving 115 optic neuritis patients showed a low yield for MRI of the spine; only four patients had spine abnormalities with a normal brain MRI.24 Abnormal cerebral spinal fluid findings in optic neuritis patients include oligoclonal bands in up to 69%, IgG in up to 36%, and myelin basic protein in 20%.25
Diagnosis of MS follows the McDonald Criteria for Diagnosis of Multiple Sclerosis created by an international panel of 30 MS experts and updated in December 2017.26 The following conditions need to be met for diagnosis of MS: evidence of damage in two or more separate areas of the central nervous system (optic nerve, brain, or spinal cord), evidence that the damage occurred at least one month apart, and the damage did not occur due to another disease. Three key changes in the 2017 updated criteria were: 1) positive findings of oligoclonal bands in the cerebral spinal fluid can substitute for demonstration of dissemination of lesions in time in some settings, 2) asymptomatic and now symptomatic MRI lesions can be considered in determining dissemination in space or time, and 3) cortical lesions were added to juxtacortical lesions for use in determining MRI criteria for dissemination of lesions in space.26
The Optic Neuritis Treatment Trial
The ONTT provided valuable information about the clinical profile of optic neuritis patients, the benefits and adverse effects of corticosteroid treatment, and the risk of developing MS in patients with optic neuritis. The ONTT enrolled 457 patients with acute optic neuritis between 1988 and 1991 who were followed prospectively for 15 years with final examination in 2006. Patients were seen within eight days of symptom onset with unilateral vision loss in an eye without prior history of optic neuritis. Patients were randomized to one of three treatment groups: oral prednisone (1 mg/kg/day) for 14 days; intravenous methylprednisolone (250 mg every 6 hours) for 3 days, followed by oral prednisone (1 mg/kg/day) for 11 days; and oral placebo for 14 days. The oral prednisone and placebo groups were double-masked. The intravenous methylprednisolone group was single-masked. Visual acuity, contrast sensitivity, color vision and visual field were evaluated at baseline, at seven follow-up exams in the first six months and then yearly to determine the rate of visual recovery and long-term outcome. The primary purpose of the ONTT was to determine whether oral or intravenous steroids altered the visual outcome in patients with optic neuritis. The results showed that a three-day course of methylprednisolone given intravenously in a dose of 250 mg every six hours followed by two weeks of daily oral prednisone in a dose of 1 mg/kg/day accelerated visual recovery but did not improve the eventual visual outcome. Treatment with oral prednisone alone in a dose of 1 mg/kg/day for two weeks also did not improve visual outcome and was associated with an increased rate of optic neuritis recurrence.9
An unanticipated finding of the ONTT was that intravenous steroids had a protective effect and reduced the risk of a second demeylinating attack consistent with MS: 16% of patients who received intravenous corticosteroids followed by oral corticosteroids developed MS over two years compared to 30% of the patients treated with oral steroids or placebo.27 This protective effect, however, was not seen in the third year, where the risk for recurrence was equal among the patients treated with intravenous steroids, oral steroids and placebo.27
The ONTT also revealed a correlation between baseline brain MRI lesions and the risk of developing MS at five, 10 and 15 years. In the trial, 25% of patients with normal brain MRI scans developed MS within five years, which significantly increased to 50% if one or more MRI lesions were present. At 10 years, the risk of developing MS was 56% in patients with one or more MRI lesions compared to 22% of patients with normal MRI scans. At 15 years, 72% of patients with one or more MRI lesions developed MS compared to 25% of patients with no lesions.28 The researchers concluded that findings on baseline brain MRI at the time of the first episode of optic neuritis was the single most important predictor of future risk of MS.27,28
Teaching instructions and assessment methodology
This teaching case report is most appropriate for fourth-year optometry students and optometry residents who have learned about optic neuritis associated with MS in a didactic setting and will be gaining more clinical experience during rotations or residency. After a thorough review of this patient’s case, follow-up visits and discussion of optic neuritis, fourth-year optometry students and optometry residents should have a better understanding of the pathogenesis of the condition, clinical findings, treatment and follow-up guidelines and the conclusions of the ONTT. Students and residents should also have gained insight into the optometrist’s role in the management of patients with MS, the importance of regular dilated eye exams and how to incorporate additional testing and imaging including visual fields, color vision, optic nerve photos and RNFL OCT to aid in patient management and follow-up care.
This teaching case report can be delivered to fourth-year optometry students and/or optometry residents as a journal club reading assignment for discussion in an ocular disease or primary care clinic rotation or residency. Students and residents would also independently answer the discussion and critical-thinking questions. During journal club, the students and/or residents should share their answers and discuss the case, the major findings of the ONTT, and the insight they gained from the case regarding how to manage MS patients with and without a history of optic neuritis.
One way to assess the understanding of this case is a role play during which one student/resident plays the role of a patient with MS and the other student/resident plays the role of the optometrist. The team can simulate a baseline eye exam and the student/resident playing the role of the doctor can ask the appropriate questions, discuss the additional tests or imaging that should be completed, and complete the patient education. The student playing the role of the patient could also imitate having sudden changes in vision or eye pain, and the team could discuss what tests need to be performed and where the patient should be referred if optic neuritis is diagnosed. Other options are a group discussion with students and residents sharing cases of patients they may have seen with MS or other demyelinating neuro-ophthalmologic conditions and how they can use OCT scans of the RNFL and ganglion cell layer in monitoring these diseases.
Conclusion
Optic neuritis is an inflammatory demyelination of the optic nerve that is highly associated with MS. Optic neuritis occurs in up to 50% of patients with MS. The two most common symptoms of optic neuritis are vision loss and eye pain. Signs of optic neuritis include decreased visual acuity, APD, abnormal color vision, visual field defects and reduced contrast sensitivity. One-third of patients have visible optic nerve inflammation and two-thirds have a normal-appearing optic nerve, which is known as retrobulbar optic neuritis. The ONTT showed that high-dose intravenous corticosteroid treatment is beneficial for acute attacks and that oral corticosteroid alone is contraindicated due to increased risk of recurrence. Gadolinium contrast-enhanced MRI of the brain and orbits provides confirmation of optic neuritis, and baseline MRI findings are an important predictor of the future risk of MS. Eye physicians play a critical role in the co-management of MS patients with and without a prior history of optic neuritis.
This case report shows the value of obtaining baseline fundus photos, RNFL OCT scans and visual field testing on MS patients to help assess changes that occur throughout the course of the disease. It is also crucial for eye physicians to counsel patients with MS on the signs and symptoms of optic neuritis and the need for immediate evaluation if any acute symptoms occur. Prompt diagnosis and treatment of optic neuritis are needed to prevent optic nerve and RNFL atrophy, which can lead to chronic vision loss, reduced contrast sensitivity, color vision deficits and visual defect defects.
References
1. Behbehani R. Clinical approach to optic neuropathies. Clin Ophthalmol. 2007 Sep;1(3): 233-46.
2. Ebers GC. Optic neuritis and multiple sclerosis. Arch Neurol. 1985;42(7):702-4.
3. Frohman EM, Frohman TC, Zee DS, et al. The neuro-ophthalmology of multiple sclerosis. Lancet Neurol. 2005;4(2):111-21.
4. Beck RW, Trobe JD, Moke PS, et al. High- and low-risk profiles for the development of multiple sclerosis within 10 years after optic neuritis: experience of the optic neuritis treatment trial. Arch Ophthalmol. 2003;121(7):944-9.
5. Percy AK, Nobrega FT, Kurland LT. Optic neuritis and multiple sclerosis. An epidemiologic study. Arch Ophthalmol. 1972;87(2):135-9.
6. Lightman S, McDonald WI, Bird AC, et al. Retinal venous sheathing in optic neuritis. Its significance for the pathogenesis of multiple sclerosis. Brain. 1987 Apr;110(Pt 2):405-14.
7. Roed H, Frederiksen J, Langkilde A, Sørensen TL, Lauritzen M, Sellebjerg F. Systemic T-cell activation in acute clinically isolated optic neuritis. J Neuroimmunol. 2005 May;162(1-2):165-72.
8. Söderström M, Link H, Xu Z, Fredriksson S. Optic neuritis and multiple sclerosis: anti-MBP and anti-MBP peptide antibody-secreting cells are accumulated in CSF. Neurology. 1993; 43(6):1215-22.
9. Optic Neuritis Study Group. A randomized, controlled trial of corticosteroids in the treatment of acute optic neuritis. N Engl J Med. 1992 Feb 27;326(9):581-8.
10. Beck RW, Kupersmith MJ, Cleary PA, Katz B. Fellow eye abnormalities in acute unilateral optic neuritis: experience of the optic neuritis treatment trial. Ophthalmology. 1993;100(5):691-8.
11. Brusa A, Jones SJ, Plant GT. Long-term remyelination after optic neuritis: A 2-year visual evoked potential and psychophysical serial study. Brain. 2001 Mar;124(Pt 3):468-79.
12. Kemp PS, Winges KM, Wall M. Optic neuritis. EyeRounds.org. Posted Sept. 30, 2012. Available from https://www.EyeRounds.org/cases/159-optic-neuritis.htm
13. Klistorner A, Arvind H, Nguyen T, et al. Axonal loss and myelin in early ON loss in postacute optic neuritis. Ann Neurol. 2008 Sep;64(3):325-31.
14. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006 March 23;354(12):1273-80.
15. Fang JP, Donahue SP, Lin RH. Global visual field involvement in acute unilateral optic neuritis. Am J Ophthalmol. 1999 Nov;128(5):554-65.
16. Beck RW, Cleary PA, Backlund JC. The course of visual recovery after optic neuritis. Experience of the Optic Neuritis Treatment Trial. Ophthalmology. 1994;101(11):1771-8.
17. Cole SR, Beck RW, Moke PS, Gal RL, Long DT. The National Eye Institute Visual Function Questionnaire: experience of the ONTT. Optic Neuritis Treatment Trial. Invest Ophthalmol Vis Sci. 2000 April;41(5):1017-21.
18. Rebolleda G, Diez-Alvarez L, Casado A, et al. OCT: new perspectives in neuro-ophthalmology. Saudi J Ophthalmol. 2015 Jan-Mar;29(1):9-25.
19. Lamirel C, Newman NJ, Biousse V. Optical coherence tomography (OCT) in optic neuritis and multiple sclerosis. Rev Neurol (Paris). 2010 December;166(12):978-86.
20. Ratchford JN, Saidha S, Sotirchos ES, et al. Active MS is associated with accelerated retinal ganglion cell/inner plexiform layer thinning. Neurology. 2013;80(1):47-54.
21. Kale N. Optic neuritis as an early sign of multiple sclerosis. Eye Brain. 2016 Oct 26;8:195-202.
22. Rocca MA, Hickman SJ, Bö L, et al. Imaging the optic nerve in multiple sclerosis. Mult Scler. 2005 Oct;11(5):537-41
23. Hickman SJ, Toosy AT, Miszkiel KA, et al. Visual recovery following acute optic neuritis – a clinical, electrophysiological and magnetic resonance imaging study. J Neurol. 2004;251(8):996-1005.
24. Dalton CM, Brex PA, Miszkiel KA, et al. Spinal cord MRI in clinically isolated optic neuritis. J Neurol Neurosurg Psychiatry. 2003;74(11):1577-80.
25. Nilsson P, Larsson EM, Maly-Sundgren P, Perfekt R, Sandberg-Wollheim M. Predicting the outcome of optic neuritis: evaluation of risk factors after 30 years of follow-up. J Neurol. 2005;252(4):396-402.
26. Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162-173.
27. Beck RW, Cleary PA, Trobe JD, et al. The effect of corticosteroids for acute optic neuritis on the subsequent development of multiple sclerosis: The Optic Neuritis Study Group. N Engl J Med. 1993 Dec 9;329(24):1764-9.
28. Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: final optic neuritis treatment trial follow-up. Arch of Neurol. 2008;65(6):727-32.
 Save article as PDF
Save article as PDF