
PEER REVIEWED
Navigating Visual Field Loss, Visual Neglect, and Ocular Dominance
Esther Moller, OD, Jessica Licausi, OD FAAO, FCOVD, Shephali Patel, OD, MS,FAAO
Abstract
Functional visual field loss can be caused by neurologic or ocular disease issues. Proper management will depend on its etiology, and therefore, ancillary testing is required to rule out visual neglect and ocular dominance interference. The results of the tests are essential to optimize patient management.
This teaching case report discusses a patient with multi-factorial visual field loss from bilateral end- stage glaucoma, stroke, ocular dominance, and possible neglect who presented for a low vision examination. Visual field, visual neglect and ocular dominance tests were performed. The patient was sent for vision rehabilitation therapy to teach proper scanning techniques to compensate for visual field deficits.
Clinical presentation, differential diagnosis, pertinent ancillary testing and proper co-management are discussed. The results of the ancillary testing and how it affected proper management are the key points to the management of patient’s ability to navigate in his world.
Key Words: visual field defect, visual neglect, ocular dominance, ocular rivalry, hemianopia
Background
Visual field loss can lead to difficulties in the performance of many activities of daily living as well as orientation and mobility. Furthermore, field loss can be complicated by visual neglect, a condition where a lesion in the cranial hemisphere causes a spatial bias and increased attention toward the ipsilateral visual hemifield and decreased attention to the contralateral visual hemifield.1 Although the etiology of neglect is poorly understood and pathophysiology highly controversial, many believe the damage is a result of specific lesions in the gray matter, while others believe the damage is along the large white matter fiber tracks.2 Testing can help isolate neglect from other sources of functional visual field loss. This is a case report of a patient who had several comorbidities of field loss making it difficult to elucidate whether neglect was present. Clinical presentation, differential diagnosis, pertinent ancillary testing and proper referrals are discussed. The intended audience is third and fourth-year optometry students, optometry residents and primary care optometrists.
Case Description
An 81-year-old white male with a recent diagnosis of severe bilateral primary open angle glaucoma presented to the low vision clinic for evaluation of functional vision deficits due to reduced visual field. The patient complained of difficulty finding objects or people, accidentally bumping into them, knocking down surrounding objects and missing steps while walking up or down stairs. Ocular history included cataract extraction in both eyes 5 years prior to examination. Ocular treatment for glaucoma management included 1 drop of latanoprost 0.005% at night in both eyes, 1 drop of brimonidine 0.20%-brinzolamide 1.00% 2 times a day in both eyes and 1 drop of timolol 0.50% once a day in both eyes. Medical history included hypertension, coronary artery disease, chronic kidney disease, atrial fibrillation, anemia, and gastroesophageal reflux disease, all of which were controlled medically, and a right intra-cranial hemorrhage with craniotomy.
At the present visit, the patient’s best-corrected vision was 2M/2.5 in each eye, as measured with an ETDRS test. Pupils were equal, round, reactive to light, and ocular motilities were full range of motion, but jerky movements were present in both eyes. His contrast sensitivity testing revealed 1.32 (severe contrast loss) with both eyes tested together as measured with a Mars contrast test. His Amsler grid testing at 33 centimeters revealed a three to four left column scotoma in the right eye, an upper-left (superior-temporal) scotoma in the left eye, and a left sided hemianopia when tested with both eyes together. Confrontation visual fields revealed a complete left hemianopia for the right eye, a superior and inferior-nasal constriction and possible left sided neglect in the left eye.
Humphrey visual field (HVF) 24-2 of the right eye revealed an overall deeply constricted defect which is densest superior and inferior-nasal (Figure 1a). The HVF 24-2 of the left eye revealed a deeper overall constricted field, which is densest superior and inferior-temporal (Figure 1b). The HVF 10-2 of the right eye revealed a left hemianopia with some extension superior-temporal and inferior-temporal (Figure 2a). The HVF 10-2 of the left eye revealed a complete and deep full field defect (Figure 2b).
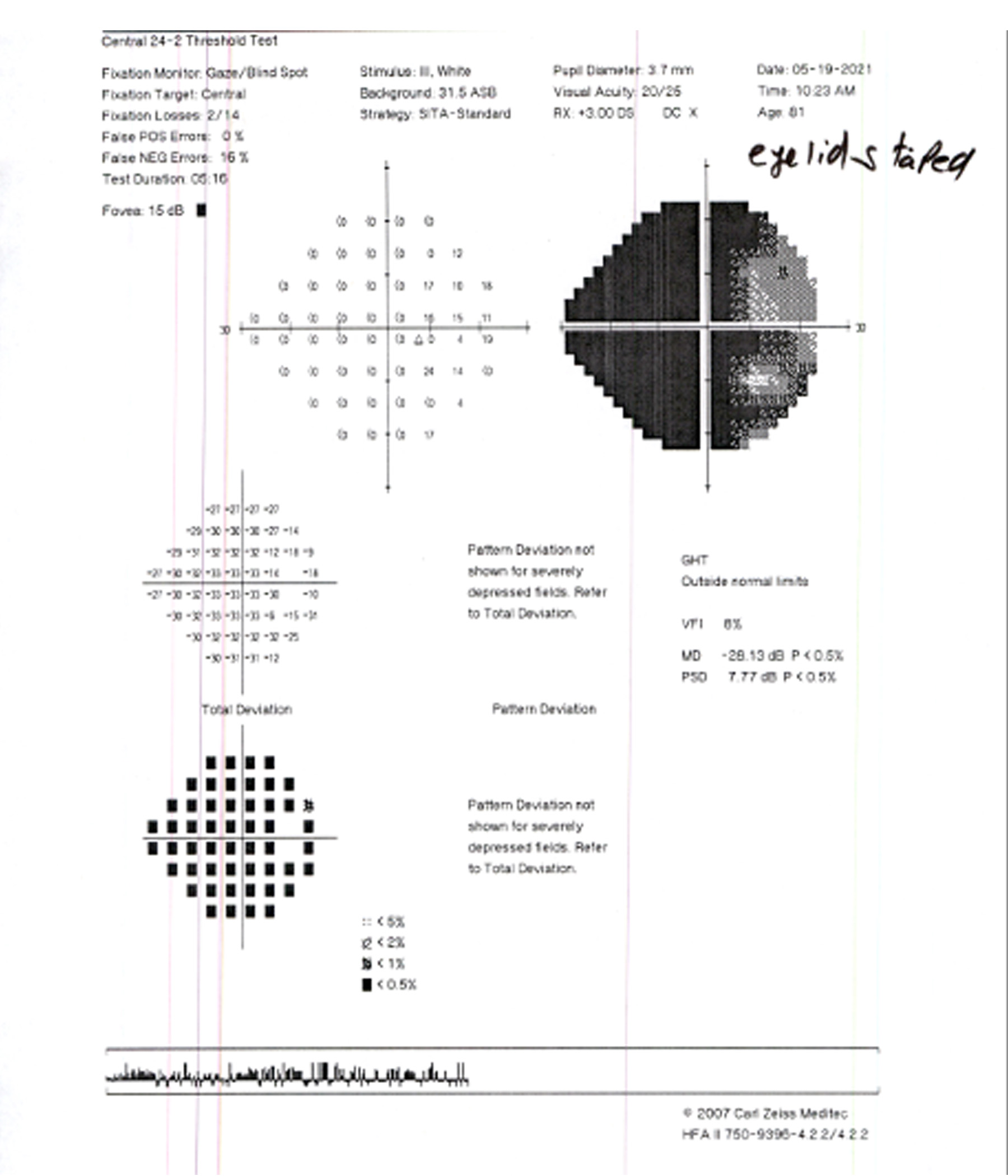
Figure 1a. Humphrey Visual Field 24-2 of the right eye. Click to enlarge
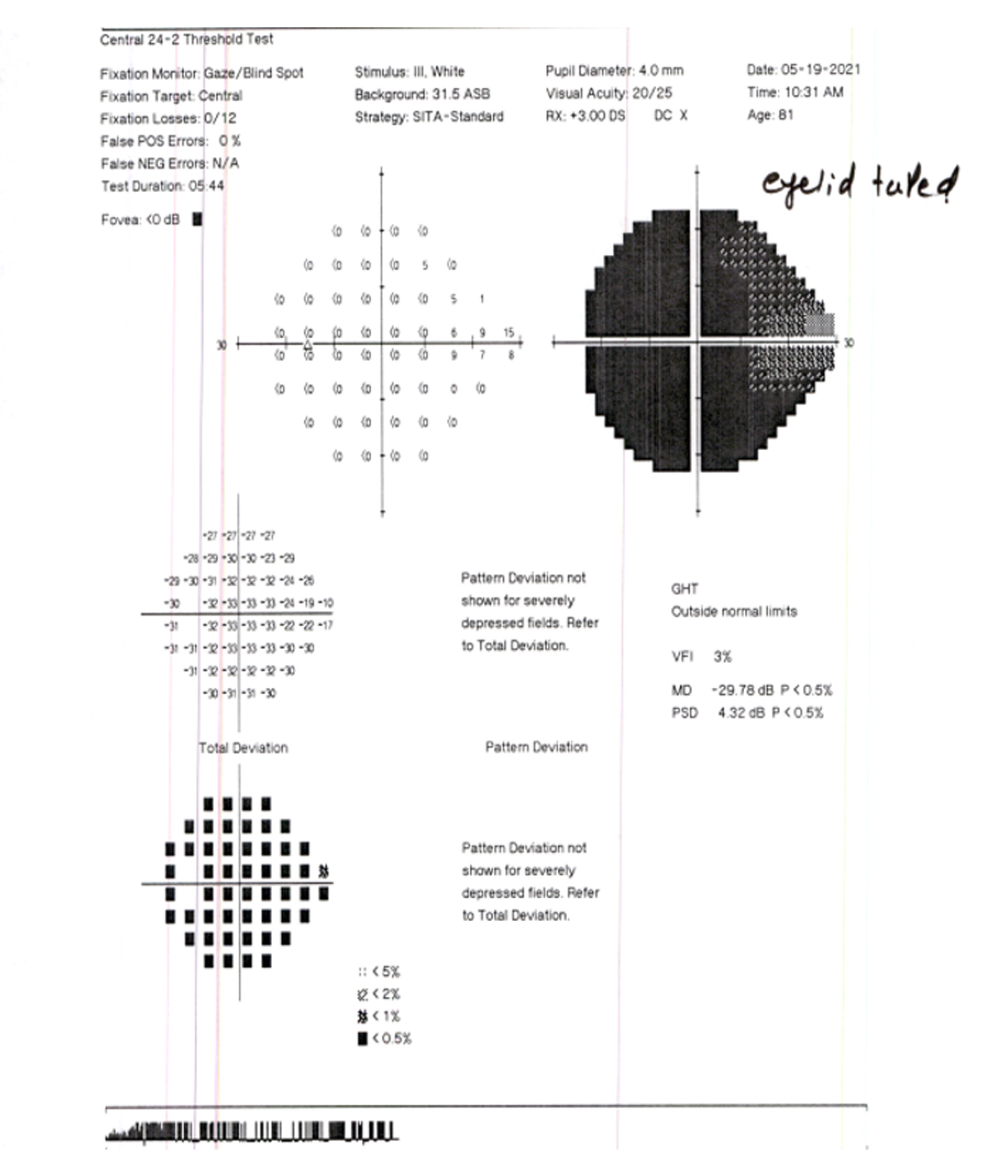
Figure 1b. Humphrey Visual Field 24-2 of the left eye. Click to enlarge
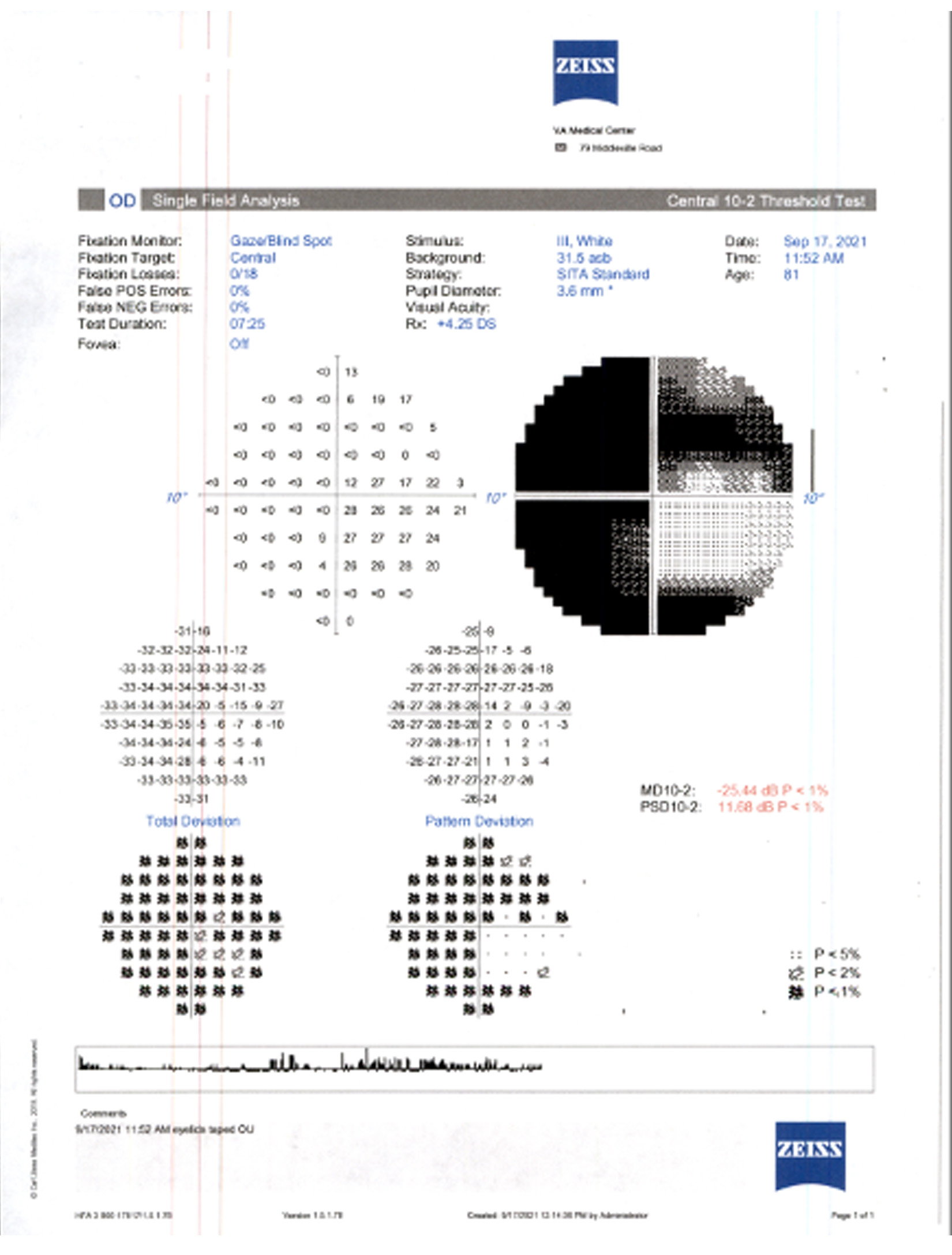
Figure 2a. Humphrey Visual Field 10-2 of the right eye. Click to enlarge

Figure 2b. Humphrey Visual Field 10-2 of the left eye.Click to enlarge
Initially, the patient was thought to have visual field loss from glaucoma. However, testing revealed a left hemianopia, likely from a hemorrhagic stroke causing a concurrent left-sided hemianopic visual field defect.
Neglect testing included the line bisection test (Figure 3) and the clock drawing test (Figure 4). Both tests showed the patient’s ability to complete the task with only a possible small neglect component.

Figure 3. Patient’s line bisection test of various lengths. Click to enlarge
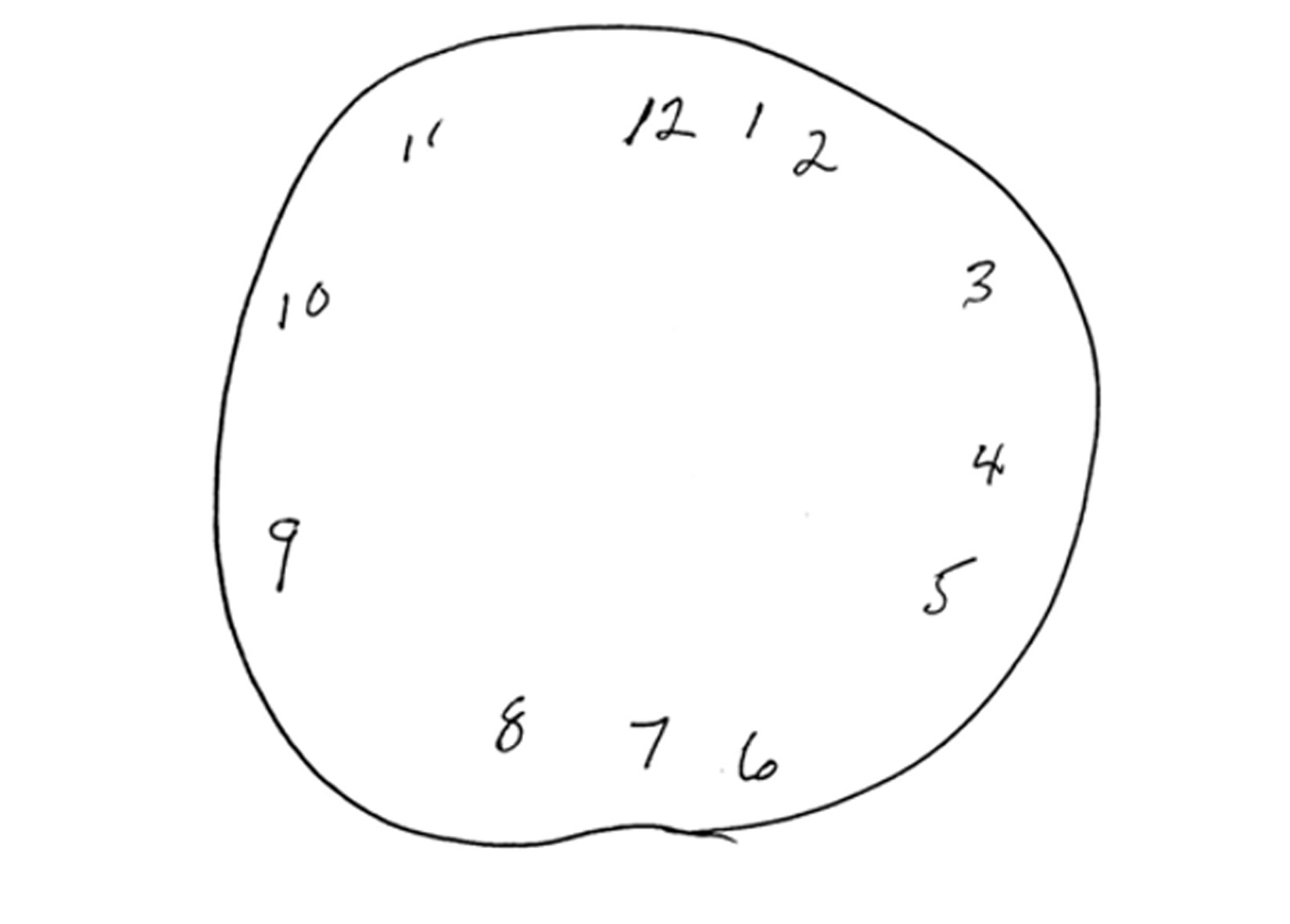
Figure 4. Patient’s clock drawing test.
Click to enlarge
Overall, the patient’s visual acuity was adequate for his needs with standard distance glasses: right eye: +1.75-1.75×045, left eye: +0.25-0.75×090; and with reading glasses right eye: +4.25-1.75×045, left eye +2.75-0.75×090 with six prism diopters base left prism in both eyes. The patient was referred to vision therapy for scanning training. The patient was also referred to the Blind Rehab Outpatient Specialist (BROS) for orientation and mobility training. The patient was educated to keep his scheduled appointments with glaucoma clinic.
Education Guidelines
Learning objectives
- Understand the anatomy of visual field loss, ocular dominance and neglect
- Techniques for testing and analyzing concurrent visual neglect testing
- Technique for testing and analyzing concurrent ocular dominance testing
- Identify proper referrals and co-management
Key concepts
- Identify multiple causes for field loss in single patient
- Testing to differentiate the causes of field loss
- Management of patients with field loss
Discussion questions
- What is the definition of a homonymous visual field defect and what is the definition of visual neglect?
- What is the anatomical correlate for visual field defects?
- What is the anatomical cause of visual neglect?
- Why is left sided neglect more common than right sided neglect?
- What are some tests used to diagnose neglect, and why is this important for patients with visual loss?
- What are some tests used to identify the dominant eye?
- What are some techniques used in optometric management of neglect and ocular dominance?
- To whom should referrals be considered?
Teaching instructions
This case report is appropriate for discussion among third- and fourth- year optometry students and would be most applicable to those in primary care, ocular disease, and low vision rotations. The authors recommend presenting the case as a power point with concurrent verbal discussion. The verbal discussion should include the discussion questions (below) to evaluate the learning objectives and student understanding of the condition, its management and treatment. The discussion questions should be completed once the case and discussion section of the paper have been thoroughly read and reviewed.
Discussion
What is the definition of a homonymous visual field defect and what is the definition of visual neglect?
A homonymous visual field defect is a definite physical loss of visual field on the same side of both eyes, which is typically caused by neurologic insult. Depending on where along the pathway the insult occurs, a typical defect will occur as will be discussed in question two. Visual neglect is a spatial bias, which leads to a person’s inattention to half of their body and/or their surroundings.
What is the anatomical correlate for visual field defects?
Visual field defects correlate to where along the visual pathway the lesion is located. Pre-chiasmal lesions will affect one eye only. Chiasmal lesions will typically affect the bi-temporal fields. Post-chiasmal lesion will cause homonymous visual field defects. The further back along the visual pathway the lesion, the more congruous and homonymous the defect. Vascular lesions of the occipital lobe are macular sparing.4
What is the anatomical cause of visual neglect?
The pathophysiology of neglect is poorly understood, controversial and has many theories. The theories can be broken down into two main categories: the gray matter lesions and the white matter lesions.
The gray matter lesion category has many conflicting theories. There are several areas thought to be involved in causing the neglect. The inferior parietal lobe (IPL) at the junction with the temporal lobe has been shown, in some studies, to be the area of concern.2 However, other studies have shown that it may be the middle and rostral parts of the superior temporal gyrus (STG).2 More recent studies have theorized that different lesions may cause different types of neglect (personal/extra-personal or viewer-centered, stimulus centered).2 The superior parietal lobe, specifically the temporo-parietal junction, has also been shown to cause neglect when there is an imbalance between the right and left hemisphere.4
Newer research has focused on white matter lesions.2 New imaging, diffusion tensor magnetic resonance imaging tractography (DT-MRI), is used to track long range white matter fibers which can cause large-scale dysfunction if affected.2 Studies have highlighted the second branch of the superior longitudinal fasciculus, which connects the inferior parietal lobe, superior parietal lobe and frontal lobe as a possible root for visual imbalance and neglect.5 The white matter model focuses on poorly functioning cortical networks rather than specific lesion in the cortex (gray matter model).2 Research has postulated that looking at the network dysfunction may give a more accurate prognosis than looking at specific lesions in the gray matter.2
While the actual lesion or area of dysfunction is unclear in both models, there is agreement that it is often larger or several interacting and overlapping lesions that cause large-scale dysfunction.2 Researching the affected pathways on a general level lends a different perspective on the pathophysiology of unilateral spatial neglect. There are two main visual pathways. The first pathway connects the retina to the lateral geniculate body and continues further to the occipital cortex.5 This is a retinotopic pathway and therefore lesions post-chiasm will cause a contralateral hemianopic visual field loss that can be documented with perimetric testing.6 The second pathway connects the visual cortex to the parietal cortex.6 This is a non-retinotopic pathway and therefore a lesion along this pathway will not be able to be detected on perimetry, rather it will cause unilateral spatial neglect.6
Unilateral spatial neglect is most commonly caused by cerebral vascular accidents (CVA), typically when the middle cerebral artery is affected.6,7,8,9 A stroke can cause lesions along the first pathway, the second pathway or a combination of the two.6 Clinically it would present as visual field loss, neglect, or a combination of the two. In the latter scenario, the patient may not be aware of the hemianopia due to the neglect present as well.6
Why is left sided neglect more common than right sided neglect?
(Figure 5) The right visual hemifield is controlled by both the right and left hemisphere. The left visual hemifield is controlled by the right hemisphere alone. If there is damage to the left hemisphere there is still some control by the right hemisphere of the right hemifield, thereby allowing processing of information and preventing neglect of the right hemifield. If there is damage to the right hemisphere there is no control of the left hemifield anymore thereby potentially causing neglect.10 The examples used in this teaching case report will reflect left-sided neglect since it is the more common form of neglect seen clinically.

Figure 5. Rendition of brain hemisphere attention control of visual hemifield.
Click to enlarge
What are some tests used to diagnose neglect, and why is this important for patients with visual loss?
It is important to elucidate neglect from visual field loss as prognosis and management While there are no standardized test forms, there are several tests that can be used to identify neglect. The clinician must draw the templates for the patient to complete.
- Copy drawing tests
- Instructions: Have the patient copy a drawing that is in front of them.
- Interpretation: The patient with left neglect will omit the details of the left side of the drawing or in rare cases will expand the details on the left side.2 (Figure 6)
Figure 6. Rendition of the rare case of detail expansion in the left hemifield.
Click to enlarge
- Memory drawing
- Instructions: Have the patient draw a picture from memory, once with open eyes and once with closed eyes.
- Interpretations: With open eyes, the patient with left neglect usually omits the left side’s details or in rare cases extends the details on the left side. With closed eyes, the patient with left neglect can usually draw the full drawing in a more symmetrical manner. Withholding visual stimulation can be used in training techniques.2
- Line cancellation test
- Instructions: Have the patient cancel many small lines on a sheet in front of them.
- Interpretation: Patients with left neglect usually only cross out the line on the right side of the paper and may cross out the same line repeatedly, known as “perseverative”. They misjudge found targets as new discoveries.11 After the left neglect has resolved, the patient may be able to cancel out all the lines. However, they will usually start from the right side of the paper as opposed to the typical left side as we read from left to right.11
- Line bisection
- Instructions: Have the patient bisect different size horizontal lines.
- Interpretation: This test can differentiate neglect from hemianopia and identify when comorbid.
- Left neglect alone: Average size line (greater than 5 cm): the bisection will be skewed to the right, the longer the line the more rightward the bisection will be. Small line (5 cm or less): the bisection will be skewed to the left due to the poorly understood mechanism of the paradoxical effect.2
- Left hemianopia alone: The bisection will be to the left of center
- Left hemianopia in conjunction with left neglect: The bisection will have the most marked deviation rightward.12
- Visual memory: Have the patient describe a familiar street that has shops on both sides as they imagine walking down the street. An alternative to this test can be to walk down a well decorated hallway and then have the patient describe the hallway’s decorations. ** This test can identify neglect when suspected along with hemianopia **
- The patient with left neglect will mention the stores and details found on the right side only. When the patient turns around and walks back (imaginatively), the patient will mention the stores on the other side of the street, that are now on the right side in visual memory.12
What are some tests used to identify the dominant eye?
These are three tests used to identify the dominant eye:
- Keyhole test
- Instructions: Make a small triangle out of both hands by overlapping the thumbs in the same plane and overlapping the fingers perpendicular to each other, holding the hands out at arm’s length. With both eyes open, find a small distant target, such as a keyhole, and fit the view in the triangle. Close one eye at a time.
- Interpretation: The eye that contains the view of the target is the dominant eye. Limitations of this test are that about 50% of patients had variable answers 80% of the time.13
- +0.50 sphere fog test
- Instructions: With both eyes open, place a +0.50 spherical lens over each eye, one at a time.
- Interpretation: The dominant eye is the one that is more bothered by the blur induced with the +0.50 spherical lens over it. This may be a poor test for someone who has low vision, as they tend not to notice small changes in refraction. In these cases, the test may need to be performed with a higher amount of plus.
- Telescope test
- Instructions: Have the patient make a small circle out of both hands. Tell the patient to bring the circle up to the eye as if the patient is looking through a telescope.
- Interpretation: Whichever eye the patient naturally gravitates towards tends to be the dominant eye.
What are some techniques used in optometric management of neglect and ocular dominance?
Management of the patient with visual neglect is complicated by their inability to recognize their impairment. It can be difficult for patients to learn to compensate because they do not attend to that side. Therapy should focus on adaptive methods. Familiar environments, such as the home, should place frequently used objects on the side without neglect. Family members and acquaintances should be educated to approach the patient from their unaffected side. One tool that can be given to the patient is a Hemi reading card. On this card there is a red boundary marking the edge of the reading material. The patient should be educated to scan until the mark is in view ensuring that fixation is fully drawn over to the edge of the text. The red boundary should be placed on the side correlating to the side of the field loss. Any colored strip of paper placed on the side of the field loss can produce the same effect.14,15 Patients with right hemianopias should be educated to always scan over until they see the end of every word to ensure they are not missing parts of words when reading.14 The patient can also be encouraged to turn their head to the opposite side to use their intact field to scan.16
When evaluating for prismatic lenses it is important to keep in mind it may be more difficult for the patient to utilize these systems because the patient may not make an effort to look into the prism. Full field lenses may be better indicated in this patient population because the whole image from their non-seeing field is shifted to the seeing hemi-field when objects are viewed through the spectacles.17 No extra eye movements are needed to use this lens system.17 It has also been shown that this visual shift can better match the patient’s new perceived midline.17
The Eli Peli (EP) prism horizontal lens was developed by Dr. Eli Peli. Patients with neglect may also benefit from the EP Prism Horizontal Lens which does not require as many eye movements as other lens systems.14 The prism is mounted in the lens on the side of the visual field loss with the base of the prism facing in the direction of visual field loss as well. The carrier lens can have one or two segments which are placed above and below the patient’s line of sight. More commonly two segments are used.14 When wearing the lens and looking straight ahead the patient will have a simultaneous view of their seeing field from the center portion of the lens and an image of their non-seeing field from the prism segments above and below.14,15,18 (Figure 7)

Figure 7. Rendition of Eli Peli prism system for left sided neglect, as sitting on the patients face.
Click to enlarge
The brain can perceptually fill in the space between the two images produced by the superior and inferior prism segment to determine what object is located in their non-seeing field.14 There is no resultant image jump from using this prism system.14 Another benefit is that no head movements are required to obtain a view of their non-seeing field. This lens system has the benefit of increasing field awareness, however requires specific training to mitigate confusion from producing a simultaneous view. Additional benefits include utilizing higher power prisms and scanning techniques to provide a shift away from the area of field loss. The EP prism has a high acceptance rate as shown in the community-based trial funded by the National Institute of Health (NIH).19 The lens itself is a form of a Fresnel lens and thus contrast is slightly reduced when viewing objects through the prism.14 The contrast however is not as reduced as the standard Fresnel prism. It is thought the difference in contrast can be helpful for the patient to differentiate the shifted image from the real object that is straight ahead.14
Fresnel prism can be beneficial for both demonstrating any of the above lens systems but also for trialing a system with the patient during a course of therapy.14,15,18 The lenses are made up of rows of miniature prisms. This enables the prism to be available in higher powers of up to 40 prism diopters, without increasing the thickness of the lens.14 They can be applied to the back of any spectacle lens and cut to the shape of the frame.14 They also can be removed and applied as the patient needs the prism.14 The disadvantage to this lens is the reduction in contrast that is produced when viewing objects through the lens.14 They are not recommended for patients who want to drive or who are high functioning.14 If a patient is successful with a trial of Fresnel prism it can be ordered as ground-in prism.14,18 It is important to confirm with the lab before finalizing the prism prescription as each lab has an upper limit of how many prism diopters it can grind into a lens. Another factor to be mindful of is cosmesis and weight of the lenses on the patient’s face, the higher the prism diopter the more distorted and heavier the lens.
Alternative treatments may also need to be considered in these more difficult rehabilitation cases. The use of phasic alerting, or using sounds presented in the affected field, may help draw the patient’s eyes to their side of field loss during vision therapy.16
To whom should referrals be considered?
Managing neglect takes a multidisciplinary approach to care. Identifying the source of neglect and any concurrent morbidity is imperative. Working with a patient’s primary care physician, neurologist, neuroradiologist, and eye care team including primary eye care provider, vision and low vision therapists will optimize rehabilitation potential. Vision rehabilitation may include scanning techniques, peripheral awareness and laterality training.
Conclusion
Functional vision loss can be challenging to manage when confronted with concurrent causes of visual field loss. The clinician should be aware that visual neglect and ocular dominance/rivalry issues can ensue with multifactorial visual field loss. Although the pathophysiology of neglect is poorly understood, it is agreed that the damage is usually large scale and diffuse in nature.2 Utilizing the proper battery of ancillary testing can allow the clinician to target a rehabilitation plan to optimize awareness of neglect and improve patient function. The suspected contributors in the above case were multi-factorial visual field loss from bilateral end stage glaucoma and stroke, which could have led to concurrent visual neglect and ocular dominance/rivalry issues. Testing can help to finalize the source of the functional vision deficits and thereby help to manage the patient correctly with proper referrals.
References
-
- Snow JC, Mattingley JB. Goal-driven selective attention in patients with right hemisphere lesions: how intact is the ipsilesional field? Brain. January 2006;129(1): 168–181. doi: 1101.1093/brain/awh690
- Bartolomeo, P. Visual neglect, Curr Opin Neurol. August 2007; 20(4) 381-386. doi: 10.1097/WCO.0b013e32816aa3a3
- Ruddy J, Asuncion RMD, Cardenas AC. Hemianopsia. 2021 Aug 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan.
- Shindo K, Sugiyama K, Huabao L, Nishijima K, Kondo T, Izumi S. Long-term effect of low-frequency repetitive transcranial magnetic stimulation over the unaffected posterior parietal cortex in patients with unilateral spatial neglect. J Rehabil Med. 2006 Jan;38(1):65-7. doi: 10.1080/1650197050044180
- Schmahmann JD, Pandya DN, Wang R, Dai G, D’Arceuil HE, de Crespigny AJ, Wedeen VJ. Association fibre pathways of the brain: parallel observations from diffusion spectrum imaging and autoradiography. March 2007. Brain. 130(3), 630–653. doi: 10.1093/brain/awl359
- Suchoff IB, Ciuffreda KJ. A primer for the optometric management of unilateral spatial inattention. Optometry 2004 May (75): 305-318. doi: 10.1016/s1529-1839(04)70067-6
- Gainotti G, D’Erme P, De Bonis C. Components of visual attention disrupted in unilateral neglect. In: Brown JW, ed. Neuropsychology of visual perception. Hillside, N.J.: Enbaum, 1989:123-44. doi: 10.4324/9781315441849-6
- Freeman E. Unilateral spatial neglect: new treatment approaches with potential application to occupational therapy. Am J Occup Ther 2001 Jul-Aug;55:401-8. doi: 10.5014/ajot.55.4.401
- Dombovy ML, Aggarwal U. Stroke rehabilitation. In: Grabois M, Garrison SJ, Hart KA, et al., eds. Physical medicine and rehabilitation: the complete approach. Maiden, Mass.: Blackwell Scientific Publications, 2000:1331.
- Greene JDW. Apraxia, agnosias, and higher visual function abnormalities. J Neuro Neurosurg Psychiatry 2005 Dec;76 Suppl 5(Suppl5): v25-34. doi: 10.1136/jnnp.2005.081885
- Mannan SK, Mort DJ, Hodgson TL, Driver J, Kennard C, Husain M. Revisiting previously searched locations in visual neglect: role of right parietal and frontal lesions in misjudging old locations as new. J Cogn Neurosci. 2005 Feb;17(2):340-54. doi: 10.1162/0898929053124983
- Thomas RH, Hughes TA. Dot-to-dot. Pract Neurol. 2008 Oct;8(5):325-329.
- Laby DM, Kirschen DG. Thoughts on ocular dominance-is it actually a preference? Eye Contact Lens. 2011 May;37(3):140-4. doi: 10.1097/ICL.0b013e31820e0bdf
- Windsor R, Ford C, Windsor L. Visual Neglect – Hemianopsia.net Everything you need to know about Hemianopsia. Hemianopsia.net – Hemianopsia.net Everything you need to know about Hemianopsia. [Cited 2022 March 15], Available from http://www.hemianopsia.net/visual-neglect/
- Suter PS, Margolis N. Managing Visual Field Defects Following Acquired Brain Injury. Brain Injury Professional: 26-29.
- Liu GT, Volpe NJ, Galetta SL. Visual Loss: overview, visual field, testing, and topical diagnosis. Neuro-ophthalmology: Diagnosis and Management. Philadelphia: Saunders, 2001.
- Padula WV. Neuro-optometric Rehabilitation. Santa Ana, CA: Optometric Extension Program, 2000.
- Cohen AH. Management of Patients with Hemianopic Visual Field Loss. J College of Optom Vision Dev 2003;34: 111-18.
- Bowers AR, Keeney K, Peli E. Community-based trial of a peripheral prism visual field expansion device for hemianopia. Arch Ophthalmol. 2008 May;126(5):657–664. doi:10.1001/archopht.126.5.657

