
PEER REVIEWED
Floppy Eyelid Syndrome
Stephen Dellostritto, OD, MS, and Harriette Canellos, OD, FAAO, Dipl. ABO
Abstract
Floppy eyelid syndrome is a highly underdiagnosed anterior segment condition that can affect various patient populations and can be associated with obstructive sleep apnea as well as other significant ocular and systemic conditions. It is important to be able to recognize the signs and symptoms of floppy eyelid syndrome to allow for improved management strategies and proper referral for sleep studies when indicated. This case series illustrates the importance of assessing lid laxity to guide case history and management strategies for floppy eyelid syndrome patients.
Key Words: floppy eyelid syndrome, obstructive sleep apnea, snoring
Background
The following case series is designed to be used as a teaching guide for all eyecare providers. It is relevant in all levels of training, especially optometry school and residency. Floppy eyelid syndrome (FES) is a highly underdiagnosed anterior segment condition characterized by hyperlaxity of the eyelids that typically results in chronic irritation and inflammation of the conjunctival tissue.1 Since its introduction in 1981 by Culbertson and Ostler, the condition has become an established clinical entity with diagnostic features and associated ocular, as well as systemic, conditions including anterior segment disease and obstructive sleep apnea (OSA).1-2 This case series illustrates the importance of assessing lid laxity to guide case history and management strategies for FES patients.
Case Description #1
History
- Patient demographic: 38-year-old Black male
- Chief complaint: the patient presented with frequent irritation, grittiness, tearing and crusting in both eyes (OU), worse in his left eye (OS); symptoms were worse in the morning and improved slightly throughout the day; the patient denied a history of contact lens wear and reported sleeping more often on his left side with his face against the pillow
- Ocular, medical history: the patient has a history of refractive amblyopia OS (anisometropic sphere and cylinder component) with patching therapy as a child, borderline hypertension and OSA; he had been advised to utilize a continuous positive airway pressure (CPAP) machine, which he reported using minimally or not at all
- Medications: none
Pertinent findings
1. Clinical
- best-corrected visual acuity (BCVA): 20/20 OD, 20/20-3 OS
- intraocular pressure (IOP): 18 mmHg OD/OS
2. Physical
- ocular surface: external observation showed nasal ptosis OU, which was more prominent OS; slit lamp examination revealed capped meibomian glands, lid hyperlaxity superiorly (Figure 1) and inferiorly, multiple retention cysts and concretions on the palpebral conjunctiva and chronic papillary conjunctivitis, all worse OS; mild superficial punctate keratitis (SPK) was noted with sodium fluorescein dye OU
- lens: unremarkable
- fundoscopy: OD – vitreal syneresis, temporal pigmented optic nerve head (ONH) crescent, distinct borders with pink and healthy rim tissue, 0.65V x 0.60H cup-to-disc ratio, normal vasculature, flat and intact macula, and temporal retinal white without pressure; OS – vitreal syneresis, myopic ONH tilt with 360-degree myopic crescent, distinct borders with pink and healthy rim tissue, 0.75V x 0.70H cup-to-disc ratio, normal vasculature, flat and intact macula, and temporal and inferior peripheral white without pressure
3. Imaging studies: an anterior segment photograph was taken to document floppy eyelids (Figure 1)

Figure 1. Photograph of patient #1’s left eye. The superior palpebral conjunctiva is easily seen with minimal elevation of the upper eyelid, exemplifying hyperlaxity of the upper tarsus. Click to enlarge
Differential diagnosis
- Primary: meibomian gland dysfunction (MGD)/dry eye associated with FES
- Additional: chronic allergic conjunctivitis, refractive amblyopia OS, glaucoma suspect (low risk) secondary to large, asymmetric cup-to-disc ratio
Treatment and management
- Olopatadine 0.2% ophthalmic drops every day for 2 weeks, then as needed
- Refresh Lacri-Lube (Allergan) eye ointment every night at bedtime OU
- Warm compresses 2 times a day for 2 weeks then every night at bedtime OU
- Adjust sleeping position to reduce eversion of upper eyelids and mechanical irritation
- Recommended to follow-up with his primary care physician regarding his OSA and poor compliance with CPAP machine use
- Return for baseline glaucoma testing
Case Description #2
History
- Patient demographic: 53-year-old Latino male
- Chief complaint: the patient presented for a dry eye evaluation with symptoms of constant grittiness OS that worsens throughout the day; he noticed a reduced blink rate and confirmed previous report of intermittent blur or “veil” over vision that occurs shortly after blinking; the patient was referred from the neuro-optometry clinic at the University Eye Center after ruling out of neurological involvement for his subjective visual complaints of intermittent blur, decreased vision and haze, described as “gauze over vision,” much worse in his right eye (OD); the patient had been using preservative-free artificial tears once daily with temporary improvement in symptoms
- Ocular, medical history: the patient has a history of hypertension and laser epithelial keratomileuses (LASEK) more than 15 years prior to examination with no reported complications; he denied a history of OSA but reports heavy snoring and prefers sleeping on his left side
- Medications: losartan 100 mg, hydrochlorothiazide 12.5 mg every day
Pertinent findings
1. Clinical
- BCVA: 20/20 OD/OS
- dry eye testing: tear osmolarity was below range OD and 298 OS, suggesting asymmetry in osmolarity OS > OD
- IOP: 13 mmHg OD/OS
2. Physical
- ocular surface: slit lamp examination revealed trace Demodex blepharitis OU, floppy eyelids OU, lagophthalmos OU, trace injection worse superiorly and temporally OU, capped meibomian glands OU, 1+ lid wiper epitheliopathy of upper and lower lids OU, trace papillae of upper and lower lids OD, 1+ papillae of upper and lower lids OS and diffuse calcified concretions that stained with sodium fluorescein on upper and lower palpebral conjunctiva OU; the tear film appeared oily with a reduced tear break-up time (TBUT) of 6 seconds OD and 4 seconds OS with 1+ diffuse SPK inferiorly
- lens and fundoscopy: findings unremarkable
3. Imaging studies: meibography displayed no significant atrophy or truncation of meibomian glands of upper or lower eyelids in either eye
Differential diagnosis
- Primary: evaporative dry eye disease OS > OD with papillary reaction associated with FES
- Secondary: Demodex blepharitis OU
Treatment and management
- Recommended to be more cognizant of and discontinue eye rubbing
- Meibomian gland compression performed in office with noted thick, yellow secretions OU (prescribed erythromycin ophthalmic ointment 5 mg/g 2 times a day for 7 days OU)
- loteprednol etabonate ophthalmic suspension 0.5% (Lotemax) 4 times a day for 2 weeks then 2 times a day for 2 weeks OU
- lifitegrast ophthalmic solution 5% (Xiidra) 2 times a day OU
- Refresh Lacri-Lube (Allergan) eye ointment every night at bedtime OU
- Warm compresses 2 times a day for 2 weeks then every night at bedtime OU
- Initiate hypochlorous eyelid spray every night at bedtime OU
- Recommended a sleep study to rule out OSA
Case Description #3
History
- Patient demographic: 61-year-old Hispanic male
- Chief complaint: the patient presented for anterior segment consultation regarding interest in pterygium removal OD; the patient reported symptoms of fluctuating distance vision blur, tearing, dryness and itching OU, but worse OD
- Ocular, medical history: denies history of OSA but reports heavy snoring
- Medications: none
Pertinent findings
1. Clinical
- BCVA: 20/25 + OD, 20/20 – 2 OS
- dry eye testing: phenol red testing 12 mm OD, 8 mm OS
- IOP: 12 mmHg OD, 11 mmHg OS (iCare tonometry)
2. Physical
- ocular surface: external observation revealed lagophthalmos OU, hyperlaxity of upper eyelids OU, ptosis OD that appeared worse medially (Figure 2); slit lamp examination revealed capped meibomian glands, collarettes, palpebral conjunctival concretions, 1+ diffuse injection with petechial hemorrhages on the bulbar conjunctiva, and an instant tear TBUT; a 4-mm by 7-mm nasal pterygium was encroaching the visual axis OD with stromal scarring inferior OD; significant inferior stromal scarring with scalloped borders and a Hudson-Stahli line was noted OS (Figure 3)
- lens and fundoscopy: unremarkable
3. Imaging studies: anterior segment photos (Figures 2 and 3)
 Figure 2. Photograph of patient #3’s eyelid position to demonstrate ptosis, worse medially in both eyes and more pronounced in the right eye. Click to enlarge |
 Figure 3. Anterior segment photograph of patient #3’s left eye showing significant inferior-temporal stromal scarring secondary to exposure keratopathy. Click to enlarge |
Differential diagnosis
- Primary: MGD/dry eye secondary to FES
- Secondary: Demodex blepharitis, stromal scarring secondary to exposure keratoconjunctivitis and incomplete lid closure
Treatment and management
- Tea tree oil treatment for Demodex dermatitis was performed in-office
- Initiate hypochlorous eyelid spray every night at bedtime OU
- Begin cyclosporine ophthalmic emulsion 0.05% (Restasis) 2 times a day OU in conjunction with preservative-free artificial tears 4 times a day and nighttime ointment every night at bedtime OU
- Recommended to tape lids at night to reduce exposure
- Warm compresses every night at bedtime for 10 minutes OU
- Recommended a sleep study to rule out OSA
- Insert punctal plugs at follow-up visit
Education Guide
Key concepts
- Recognize the clinical findings of FES
- Better understand the diverse patient base that FES may affect
- Adjust case history to include symptoms of OSA
- Treatment and management of FES patients
- Consider sleep study referral for patients with FES and OSA symptoms
Learning objectives
At the conclusion of the case, participants should be able to:
- Identify signs and symptoms of FES
- Know the ocular and systemic manifestations in individuals with FES
- Understand the relationship between FES and OSA, as well as the postulated pathophysiology
- Provide proper patient education on management and co-management of FES
Discussion questions/points
- Describe the signs and symptoms of FES
- What case history questions could be important in patients with FES?
- What ocular and systemic diseases may be associated with FES and how could this impact management for these patients?
- What healthcare providers should be communicated with and engaged in interprofessional care?
Learning assessment
- Assess the patient’s anterior segment both in and out of the slit lamp
- Case history continues throughout the exam and should include questions related to potential systemic associations, such as OSA
- Engage students in report-writing to different healthcare providers, including primary care physicians and pulmonologists
Discussion
The term “floppy eyelid syndrome” was first proposed to describe the most prominent feature of individuals whose eyelids everted during sleep resulting in mechanical irritation and papillary conjunctivitis.2 Although diagnosis was primarily associated with, and is more common in, obese middle-age men, FES is well-documented in both males and females as well as in various age groups, including children.1-5 Furthermore, not all individuals with FES display obesity or are overweight.1-5 The prevalence of FES in the general population varies from 3.8-15.8% with increased prevalence in certain individuals, such as those with OSA, keratoconus or atopic disease. However, the prevalence is likely underestimated because of delays in diagnosis or underdiagnosis due to inaccuracy of the definition and lack of diagnostic criteria.1,6,7
There are numerous well-established ocular and systemic associations with FES as well as OSA including keratoconus, blepharitis, MGD, glaucoma, severe ocular surface disease and sequelae, obesity, hypertension, diabetes mellitus, Ehlers-Danlos syndrome, and more. Although there is an exhaustive list of systemic associations, OSA is the most prevalent, and the amount of eyelid laxity in FES appears to be correlated with OSA severity. The prevalence of OSA in patients with FES is highly debated in the literature; however, the link is evident. Both FES and OSA appear to be more commonly associated with males, obesity and increased age but both may affect men and women with various weight classes and ages.8 It is the optometrist’s role to manage the ocular manifestations of FES as well as refer and co-manage severe ocular conditions and systemic comorbidities with appropriate providers.
Typical presenting symptoms of patients with FES include ocular irritation, redness and mucous discharge that tend to be worse on the patient’s preferred sleeping side and upon waking.1,9 These non-specific symptoms can easily mimic various ocular surface disease etiologies; therefore, careful examination and history are needed for proper diagnosis and management.1,6 The hallmark of FES is hyperlaxity of the upper tarsus with easily everted superior eyelids with mild upward traction, chronic papillary conjunctivitis that tends to be worse temporally, and ptosis that tends to be worse nasally, both more significant on the preferred sleeping side. This hyperlaxity of the eyelids allows for easy eversion while sleeping, and mechanical irritation to various ocular structures results in numerous anterior segment findings, including chronic papillary conjunctivitis, nasal ptosis, lash ptosis, blepharoptosis, dermatochalasis, blepharitis and more.1,9,10 Although these presenting findings may be seen in patients with FES, these conditions should also be considered differential diagnoses for FES.
Like many conditions, FES has proposed genetic and environmental factors that may play a role in its etiology. For example, chronic eye rubbing in individuals with allergic conjunctivitis or cognitive delays. The histopathology leading to FES is not fully understood; however, several histological and biochemical changes are seen in the tarsus, conjunctiva and cornea of these patients. The tarsus in these individuals appears to display changes in elastin composition and quantity, inconsistent collagen findings, higher levels of matrix metalloproteinase (MMP) 7 and 9 and decreased meibomian gland lipid production compared with controls. The palpebral and bulbar conjunctival tissues in these patients also display signs of chronic inflammation including elevated levels of neutrophils, keratinization of the epithelium, mucin extravasation, decreased goblet cells and increased levels of MMP-2 in epithelium.6 These histological changes could be due to mechanical stress and alternating ischemia/reperfusion of tissue with side or stomach sleeping as well as intermittent systemic hypoxia during episodes of apnea.11
OSA is characterized by the collapse or narrowing of the upper airways leading to prolonged loss of ventilation and due to unfavorable upper airway anatomy and alterations in airway function during sleeping.11,12 There have been speculations as to how OSA correlates to FES, but the link is still not clearly understood. Histological comparison of the extracellular matrix of the pharyngeal wall revealed an increase in collagen type 1 and variable MMP-1 expression without significant difference between OSA patients and controls.11 Absence of inflammatory signs in samples support that inflammatory processes are located in airway tissue lining rather than deeper tissues.11 Also, greater numbers of inflammatory cells of mucosal and muscular tissue have been noted.11 It can be postulated that mechanisms involved in increased palpebral laxity may also be related to pharyngeal lateral wall laxity.11
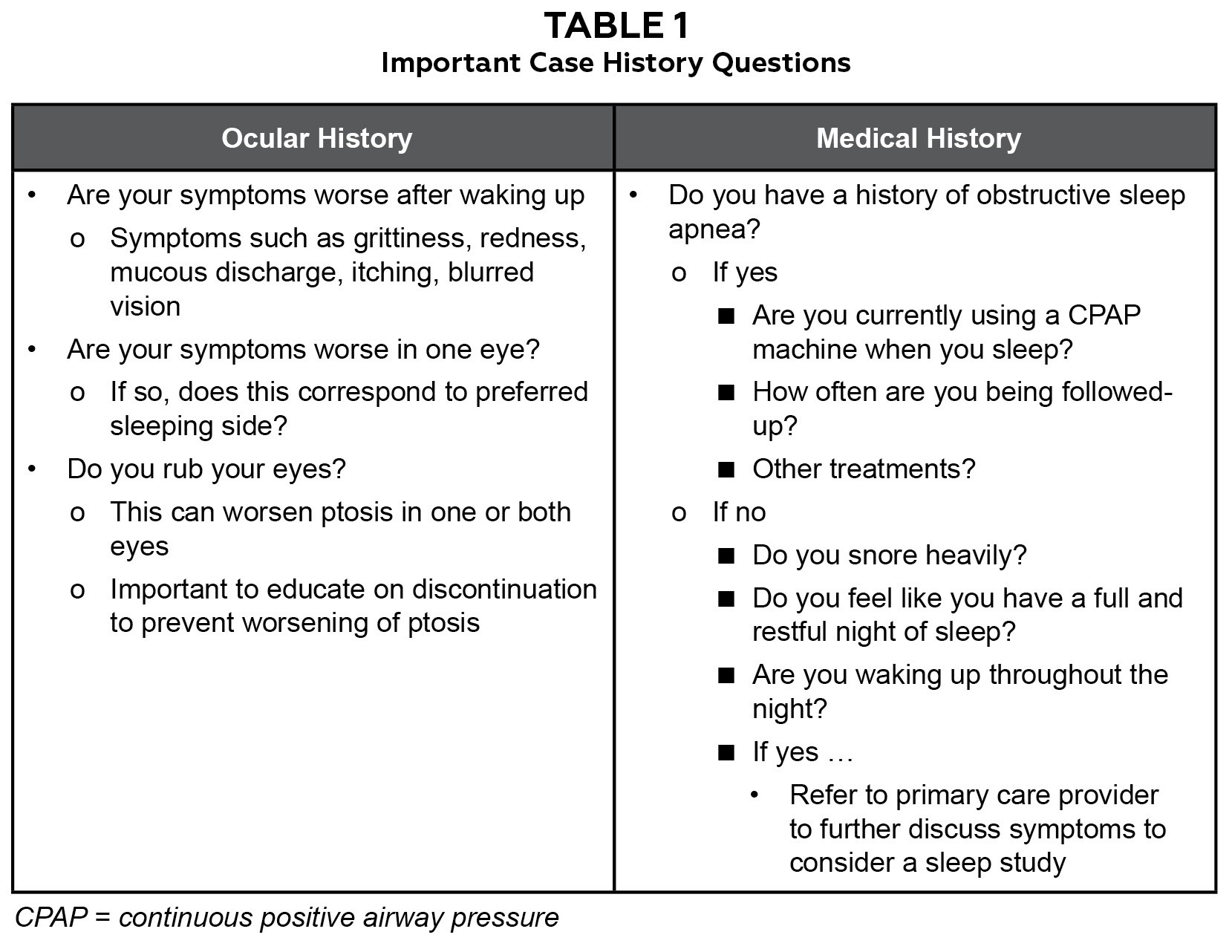
Table 1. Click to enlarge
OSA is a serious respiratory disease that can significantly impact various organ systems and, like FES, tends to be underdiagnosed.11,12 Among the most well-established risk factors are male sex, older age and obesity. Cardiac and pulmonary examinations are important as OSA prevalence is much higher (by 40% to 80%) in patients with heart failure, stroke, coronary artery disease, pulmonary hypertension, atrial fibrillation, hypertension and diabetes. OSA is also associated with increased risk of motor vehicle accidents and decreased quality of life. When examining patients with FES, it is important to ask about common clinical manifestations of OSA, which include snoring, episodes of gasping, choking, or witnessed apneas during sleep. If a patient is positive for these signs and/or symptoms of daytime sleepiness or fatigue despite sufficient opportunity to sleep, a referral for screening is indicated.12 Table 1 outlines questions that can be incorporated into the case history to help guide diagnosis and a management plan for these patients.
Managing FES from an eyecare perspective is important as well. Topical therapy options include lubricating drops and ointments, antihistamines and steroids for ocular dryness and inflammation. Lid taping, eye shields and taut sleep masks are helpful for nighttime ocular surface protection. Lifestyle modifications, such as sleep position or airflow adjustment, are also important initial management strategies. Some more recent and alternative therapies, including the use of topical steroids and 0.03% bimatoprost, have been used for treatment of FES.7 Prostaglandin F2α analogues, such as 0.03% bimatoprost, have been shown to cause prostaglandin-associated periorbitopathy such as enophthalmos, periorbital fat atrophy, eyelid retraction and deepening of the upper-eyelid sulcus. These changes are believed to be due to alterations in MMP and tissue inhibitor of metalloproteinases in adipose and collagen tissue.13
If management with medication is ineffective, oculoplastic surgical intervention, such as tarsal strip or lateral tarsorrhaphy, may be indicated for symptom relief and to preserve ocular surface integrity.7 Ophthalmology co-management and more frequent follow-ups should also be considered in FES patients with OSA due to associations between OSA and ocular diseases such as glaucoma, non-arteritic ischemic optic neuropathy and central serous chorioretinopathy.11
Teaching instructions and assessment methodology
This teaching case series is most appropriate for third- and fourth-year optometry students and optometry residents who have learned about dry eye and anterior segment disease in a didactic setting and can apply their knowledge clinically. Review of this case series should provide a better understanding of the pathogenesis of FES, its relation to OSA, and how it can lead to anterior segment signs and symptoms of dry eye. Also, students and residents should gain insight into the importance of appropriate case history, the eyecare provider’s role in the management of these conditions in an eye exam and in an interdisciplinary healthcare setting.
This teaching case series can be presented to students and residents in a grand rounds or journal club reading assignment for discussion in primary care, ocular disease or anterior segment clinic. Students and residents should develop differential diagnoses and discuss how to include assessment for FES in their dry eye workup. These cases should promote discussion of how to treat and manage patients with FES and proper interdisciplinary communication with other healthcare providers.
Assessment of student and resident learning can include group discussions of the cases and comparison of similar cases they may have encountered in the past. The discussions should focus on identifying patients with FES and the ocular treatment options. Management discussion should include systemic conditions that can be associated with FES and/or sleep apnea and co-management with other professionals. Another assessment tool can be presentation of anterior segment photographs of patients with various ocular surface conditions of varying severities, including floppy eyelids, and having students ask about and discuss symptoms, pertinent history and underlying causes and ultimately determine a treatment plan for each case.
Conclusion
FES is a highly underdiagnosed and often overlooked anterior segment condition. Knowledge of the characteristic signs and symptoms of this particular ocular surface presentation should enable proper diagnosis of FES. Routine optometric examinations can easily detect this and indicate further questioning to determine whether an OSA workup should be pursued. OSA can have significant systemic impact on patients, and optometrists should be able to help guide these patients to appropriate providers. Interprofessional collaboration is key in the management of the ocular and systemic needs of patients with floppy eyelid syndrome.
References
- Pham TT, Perry JD. Floppy eyelid syndrome. Curr Opin Ophthalmol. 2007 Sep;18(5):430-3. doi: 10.1097/ICU.0b013e3282ced08e.
- Culbertson WW, Ostler HB. The floppy eyelid syndrome. Am J Ophthalmol. 1981 Oct;92(4):568-75. doi: 10.1016/0002-9394(81)90652-8.
- Hashemi H, Rastad H, Emamian MH, Fotouhi A. Floppy eyelid syndrome and its determinants in Iranian adults: a population-based study. Eye Contact Lens. 2017 Nov;43(6):406-410. doi: 10.1097/ICL.0000000000000297.
- Eiferman RA, Gossman MD, O’Neill K, Douglas CH. Floppy eyelid syndrome in a child. Am J Ophthalmol. 1990 Mar 15;109(3):356-7. doi: 10.1016/s0002-9394(14)74572-6.
- Ezra DG, Beaconsfield M, Sira M, Bunce C, Wormald R, Collin R. The associations of floppy eyelid syndrome: a case control study. Ophthalmology. 2010 Apr;117(4):831-8. doi: 10.1016/j.ophtha.2009.09.029. Epub 2010 Jan 25.
- Salinas R, Puig M, Fry CL, Johnson DA, Kheirkhah A. Floppy eyelid syndrome: a comprehensive review. Ocul Surf. 2020 Jan;18(1):31-39. doi: 10.1016/j.jtos.2019.10.002. Epub 2019 Oct 5.
- De Gregorio A, Cerini A, Scala A, Lambiase A, Pedrotti E, Morselli S. Floppy eyelid, an under-diagnosed syndrome: a review of demographics, pathogenesis, and treatment. Ther Adv Ophthalmol. 2021 Dec 5;13:25158414211059247. doi: 10.1177/25158414211059247.
- Idowu OO, Ashraf DC, Vagefi MR, Kersten RC, Winn BJ. Floppy eyelid syndrome: ocular and systemic associations. Curr Opin Ophthalmol. 2019 Nov;30(6):513-524. doi: 10.1097/ICU.0000000000000617.
- Lee CC, Lai HT, Kuo YR, Lee SS, Lai CS. Floppy eyelid syndrome: an unfamiliar entity for plastic surgeons. Ann Plast Surg. 2018 Feb;80(2S Suppl 1):S40-S47. doi: 10.1097/SAP.0000000000001311.
- Shah-Desai S, Sandy C, Collin R. Lax eyelid syndrome or ‘progeria’ of eyelid tissues. Orbit. 2004 Mar;23(1):3-12. doi: 10.1076/orbi.23.1.3.28990.
- Cristescu Teodor R, Mihaltan FD. Eyelid laxity and sleep apnea syndrome: a review. Rom J Ophthalmol. 2019 Jan-Mar;63(1):2-9.
- Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021 Jul 20;144(3):e56-e67. doi: 10.1161/CIR.0000000000000988.
- De Gregorio A, Pedrotti E, Stevan G, Scala A, Lambiase A, Morselli S. Floppy eyelid syndrome and ectropion improvement after 1 month of 0.03% bimatoprost topical therapy. Am J Ophthalmol Case Rep. 2020 Sep 23;20:100938. doi: 10.1016/j.ajoc.2020.100938.

