
PEER REVIEWED
Differentiating Causes of Pediatric Madarosis
Matthew T. Vaughn, OD, FAAO
Abstract
Trichotillomania (TTM) is classified as a body-focused repetitive behavior of repeated pulling out of one’s hair, resulting in hair loss. This rare condition may present in the optometric setting in the form of pulling out one’s eyelashes or eyebrow hair. This case report discusses an adolescent girl who repeatedly pulls out her eyelashes, attempting to relieve her symptoms caused by anterior and posterior blepharitis and dry eye. The differential diagnoses and management of eyelash trichotillomania will be discussed. In the pediatric population, the standard treatment is cognitive behavioral therapy, which focuses on habit reversal training. It is imperative that the optometric clinician be aware of the condition and how to manage a patient who may be suffering from it, emphasizing co-management with a psychological specialist.
Key words: trichotillomania, madarosis, pediatric, blepharitis, habit reversal training, cognitive behavioral therapy
Background
The purpose of the following case report is to teach optometry students and residents about considering medical conditions outside the realm of eye care when diagnosing and managing pediatric patients. This care report is appropriate for third- and fourth-year optometry students and optometric residents who have completed didactic course work in conditions affecting the eyelids and lashes and can apply that knowledge to the clinical setting. While the ultimate diagnosis may be relatively rare, madarosis itself is not uncommon in the pediatric population.
Trichotillomania (TTM) is classified as a body-focused repetitive behavior of pulling out of one’s hair, resulting in hair loss. The estimated lifetime prevalence of TTM is 1-3%, which is likely underestimated due to the feelings of shame and denial among its sufferers.1 The few epidemiological studies that have been conducted consist only of those who came forward about the hair pulling and sought treatment.
The disorder often begins at puberty but can certainly occur in childhood or early adulthood. If TTM begins in infancy (termed “baby trich”) or early childhood, the hair pulling is usually self-limiting and prognosis is excellent. Pubescent children and adolescents have a more guarded prognosis, as there is usually underlying psychological distress contributing to the act. TTM is more prevalent in females than in males, with the divide becoming more biased toward females as patient age increases. There is no racial difference in the prevalence.2
This rare condition may present in the optometric setting in the form of pulling out one’s eyelashes or eyebrow hair. In the pediatric population, the standard treatment is cognitive behavioral therapy, which focuses on habit reversal training.3 It is imperative that the optometric clinician be aware of the condition and how to manage a patient who presents with this condition.
Case Description
Case History
A 10-year-old Indian female presented to the pediatric eye clinic at a city hospital complaining of loss of eyelashes and “severe eyelid itching” for the past 2 months. Her ocular history included mild refractive amblyopia secondary to high hyperopic astigmatism in the right eye. She wears bifocal glasses with full distance correction with an add to improve her esophoric posture at near. She also has a history of mild dry eye syndrome and mild anterior and posterior blepharitis in both eyes, which was being treated with artificial tears, warm compresses and lid hygiene, with fair compliance. There was no history of allergic conjunctivitis. Her dilated fundus examination had historically been unremarkable in both eyes.
Her medical history had previously been unremarkable, but at this visit, she reported that her scalp hair had recently been thinning and falling out “in clumps in the shower.” There was no history of acute illness prior to the eyelash or hair loss and no history of atopic or thyroid disease. She took no medications and had no known allergies.
When questioned further about her missing eyelashes, the patient readily admitted that she had been removing them herself. She reported looking in the mirror when she felt her eyelids itch and she saw “little white flakes” in her eyelashes. She then promptly removed her eyelashes attempting to relieve the itching. Her parents confirmed a history of eye rubbing but declined witnessing her pulling out her eyelashes. Her parents reported that she was in the 4th grade and was doing exceptionally well in all subjects. However, they also reported that she put an immense amount of pressure on herself to succeed in academic endeavors. She was very mature for her age and had a difficult time making friends with her peers.
Initial Presentation
The patient’s best corrected visual acuity was 20/25- OD and 20/20- OS in her 3-month-old pair of glasses: OD +6.25 -1.75 x110, OS +4.50 -0.75 x070, ADD +1.00. The patient reported excellent compliance with full time spectacle wear.
Slit lamp exam revealed madarosis of the upper and lower lids of both eyes, with the upper lids affected more than the lower lids, and the temporal aspects of the lids were more affected than nasal. The remaining lashes were broken and of varying lengths. There was also moderate flaking on the remaining lashes and stenosed Meibomian glands on the upper and lower lids. Conjunctivas were white and quiet, without papillae, follicles, or chemosis. Corneas were clear, without Fluorescein staining [Figure 1a and 1b]. The rest of the anterior and posterior segments were unremarkable. Upon physical examination, the patient’s long, brown scalp hair appeared diffusely thin, while her eyebrows had normal thickness.
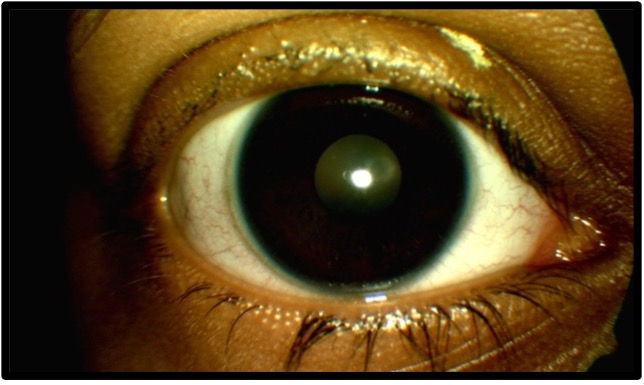
Figure 1a. Initial presentation OD, anterior segment photo. Click to enlarge
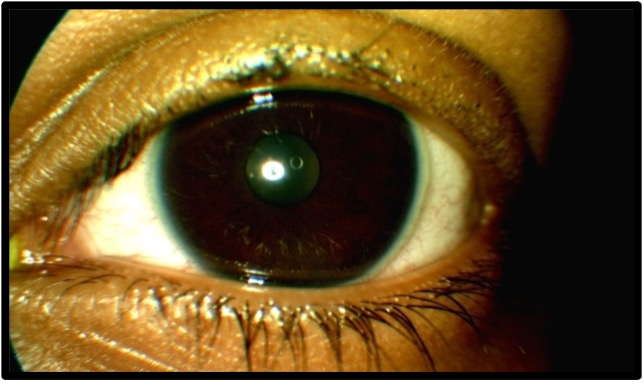
Figure 1b. Initial presentation OS, anterior segment. Click to enlarge
Differential Diagnosis
The primary differential diagnosis was madarosis of the upper greater than lower eyelids in both eyes secondary to trichotillomania; caused by anterior blepharitis, Meibomian gland dysfunction and dry eye syndrome. Other differentials included telogen effluvium (TE) and alopecia areata (AA).
Treatment and Management
After determining that the underlying stimulus to eyelash removal was the irritation caused by anterior and posterior blepharitis, a twice-daily lid hygiene regimen was prescribed. The patient was to use a lid scrubs product to lightly clean the eyelids twice a day, in addition to warm compresses twice a day for posterior blepharitis. Anterior segment photos were taken to document the presenting appearance of the patient’s lids and lashes.
The patient was thoroughly educated that the act of hair pulling was harmful to her and to fight the urge to pull as much as she could. As a competing response, she was instructed to perform supplemental lid scrubs whenever possible if she felt the urge to pull out her eyelashes. The family was also educated on the importance of follow-up to monitor not only the health of her lids and lashes, but also the status of the hair pulling. They were instructed to return for follow-up in 3 months.
Due to the concurrent diffuse scalp hair loss that the patient presented with, a consultation with a pediatric dermatologist was recommended and subsequently arranged through the patient’s pediatrician. At this consultation, the dermatologist suspected telogen effluvium secondary to stress or thyroid dysfunction, so blood work was ordered. The results of the blood testing revealed normal thyroid hormone levels, but a deficiency of vitamins D and B7. The doctor’s recommendations were vitamin D and B7 (biotin) supplements and to cut the patient’s hair. If the weight of the patient’s long hair was putting undue stress on the follicles, this would add to the effects of TE. The patient did start taking supplements but opted not to cut her hair.
A referral to a psychologist was also recommended due to the possible psychological issues related to the hair pulling and scalp hair loss. Her parents opted not to pursue this referral just yet; they wanted to start with the blepharitis treatment and supplements but agreed to remain open about consulting a psychologist if the pulling persisted.
Follow-Up Care
Follow-Up #1 (3 months later): The patient reported compliance with the lid hygiene and warm compress regimen but did admit to pulling out her lashes a few times since her last appointment. She had begun taking vitamin D and biotin supplements with a slight reduction in the amount of scalp hair loss, but her medical history was otherwise unchanged. Upon slit lamp examination, there was mild regrowth of lashes on the upper lids, but temporal madarosis was still present in both eyes. Anterior segment photos were taken [Figure 2a and 2b]. The treatment regimen was reviewed with the patient and compliance was reinforced. The parents again opted to hold off on the psychology referral. A 3-month follow-up was then scheduled.

Figure 2a. Follow-up #1, 3 months after initial presentation, OD, anterior segment photo. Click to enlarge
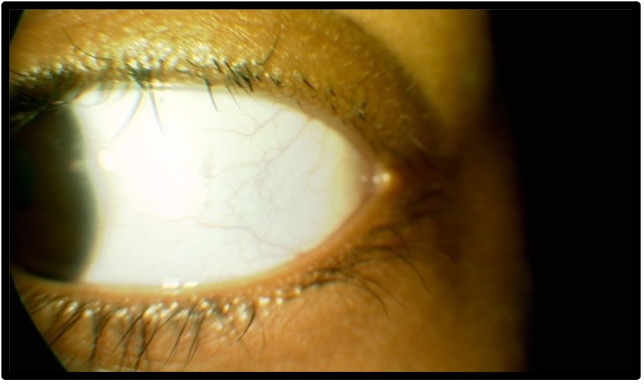
Figure 2b. Follow-up #1, 3 months after initial presentation, OS, anterior segment photo. Click to enlarge
Follow-Up #2 (3 months later): The patient presented reporting complete abstinence from pulling out her eyelashes. Her scalp hair was now also returning to its normal thickness. She reported full compliance with her lid hygiene/warm compresses regimen and was taking her vitamin supplements. Slit lamp examination showed continued regrowth of lashes, yet a few patches of madarosis remained in each eye. Anterior segment photos were taken [Figure 3a and 3b]. As at the last follow-up, the treatment regimen was reviewed, and the importance of compliance was stressed. Since the condition was improved, the parents again deferred consultation with a psychologist. The patient was instructed to return in 3 months.
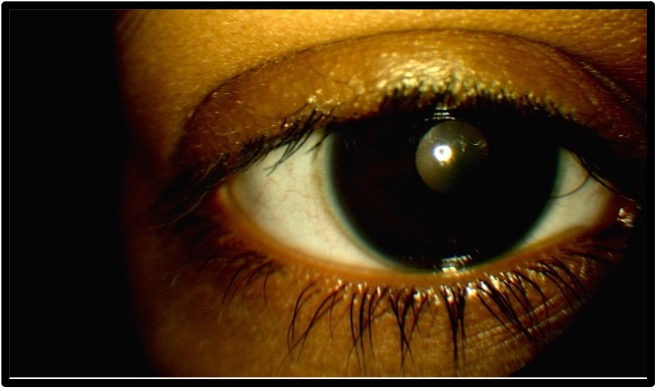
Figure 3a. Follow-up #2, 6 months after initial presentation, OD, anterior segment photo. Click to enlarge
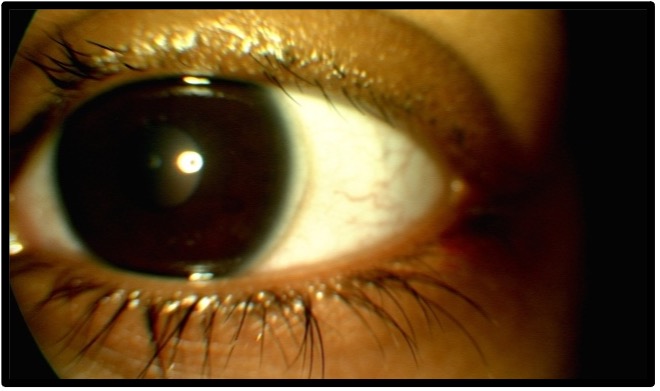
Figure 3b. Follow-up #2, 6 months after initial presenhttps://journal.opted.org/wp-content/uploads/2025/04/WS125P232Fig3b.jpg” target=”_blank” rel=”noopener”>Click to enlarge
Follow-Up #3 (3 months later): The patient once again reported full compliance with blepharitis treatment and that she had refrained from pulling out her lashes since the last visit. She also reported fuller scalp hair and that her hair density was returning to normal. The lash density was now beginning to appear more normal, with still some thinning temporally on each upper lid [Figure 4a and 4b]. Once again, treatment and compliance were reviewed with the patient, and she was instructed to return in 3 months for her annual comprehensive exam.
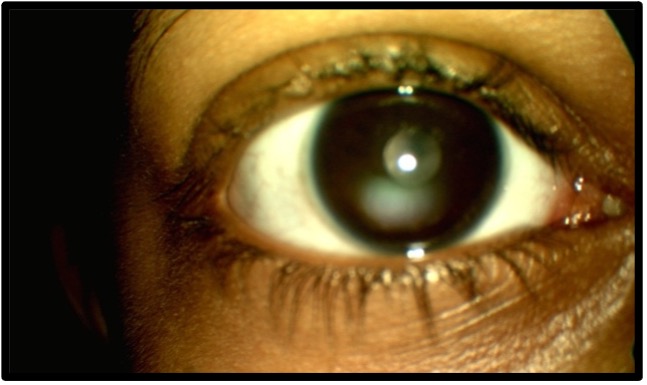
Figure 4a. Follow-up #3, 9 months after initial presentation, OD, anterior segment photo. Click to enlarge
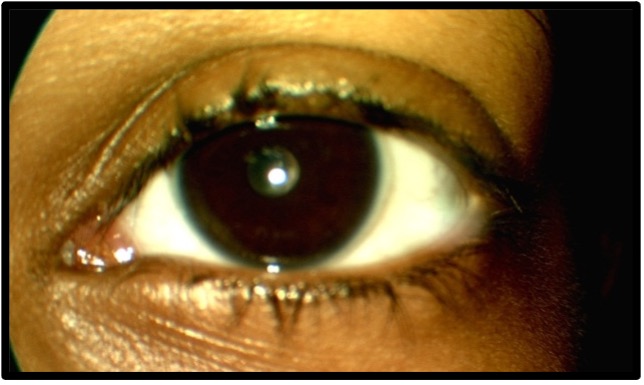
Figure 4b. Follow-up #3, 9 months after initial presentation, OS, anterior segment photo. Click to enlarge
Follow-Up #4 (3 months later, 1 year after treatment initiation): The patient proudly reported that she hadn’t pulled her eyelashes in almost 1 year, was compliant with her blepharitis treatment, and reported never even feeling the urge to pull anymore. The density of her scalp hair had stabilized, and her medical health was unchanged. On slit lamp examination, her lashes were essentially completely regrown, without patches of madarosis, and free of flakes and stenosed glands [Figure 5a and 5b]. The patient was educated that though she may not feel the urge to pull any longer, these feelings may resurface again in the future. She was educated to continue with lid hygiene and warm compresses, and to return for an amblyopia follow-up and anterior segment follow-up in 3 months.

Figure 5a. Follow-up #4, 13 months after initial presentation, OD, anterior segment photo. Click to enlarge
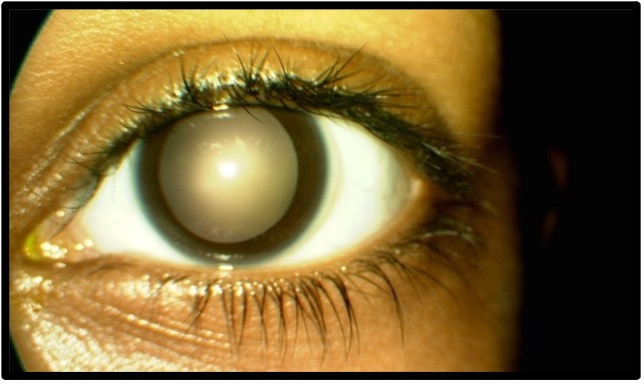
Figure 5b. Follow-up #4, 13 months after initial presentation, OS, anterior segment photo. Click to enlarge
Follow-Up #5 (3 months later): The patient reported reduced compliance with her regimen of lid scrubs and hygiene but denied pulling any eyelashes. On slit lamp examination, there was one patch of madarosis on the left upper lid, with broken lashes in the surrounding area [Figure 6a and 6b]. Despite the previous control of her TTM, the patient’s decreased compliance with the treatment plan had caused a relapse, and she had resumed the automatic pulling of her eyelashes. The patient and parents were apprised of the present findings, and the importance of keeping up with the prescribed treatment plan (warm compresses and lid scrubs twice a day, as well as additional lid scrubs upon feeling an urge to pull out lashes) was strongly stressed.
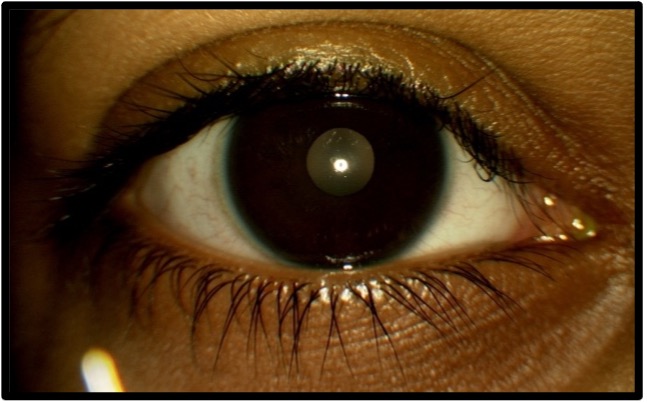
Figure 6a. Follow-up #5, 16 months after initial presentation, OD, anterior segment photo. Click to enlarge
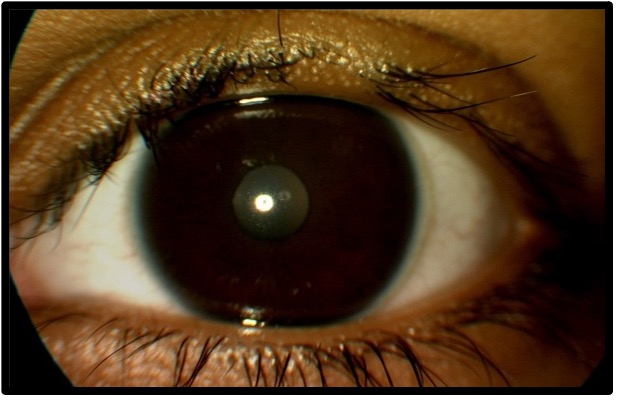
Figure 6b. Follow-up #5, 16 months after initial presentation, OS, anterior segment photo. Click to enlarge
Educators Guide
Key Concepts
- Recognizing the clinical signs of madarosis in a pediatric patient
- Delineating differential diagnoses of the loss of eyelashes
- Systemic and psychological correlations to this clinical finding
- Accurately diagnosing the condition, treating what is within optometrists’ scope and co-managing with other professionals
Learning Objectives
At the conclusion of the case, participants should be able to:
- Identify the clinical signs of madarosis
- Delineate causes of eyelash loss, including behavioral/psychological etiologies
- Understand the ocular manifestations sometimes associated with psychological conditions
- Accurately diagnose, treat and refer for co-management eyelash trichotillomania in a pediatric patient
- If manual eyelash removal is suspected, confirm this history by professionally and sensitively eliciting admission of the behavior
- Identify a patient’s triggers for the behavior of hair pulling
Discussion Questions/Points
- Describe the signs and symptoms of madarosis
- Discuss the differentials of the loss of eyelashes and of trichotillomania
- How would you educate your patient who is habitually pulling out their eyelashes?
- What types of medical and mental healthcare providers would you co-manage this case with?
Teaching Methodology
- The case report can be delivered to students and/or residents in a grand rounds or case discussion format, in a didactic setting or clinical discussion in pediatrics or anterior segment clinics
- Utilizing problem-focused instruction, learners can concentrate on the patient’s complaint of madarosis and explore various causes and management options to address this unique complaint
- Using case-focused instruction, learners can use their foundational knowledge of eye care, supplemented by additional phycological and dermatological information from the instructor, to find out-of-the-box solutions using their analytical skills.
- Students and residents should be able to talk through the analysis of signs and symptoms, development of differentials, as well as the optometric and co-management of the condition.
Learning Assessment
- Change small details in the case and have learners discuss how management would change, e.g. if the patient did not admit to pulling out her eyelashes
- Based on the pharmacological review in treating adults with TTM, have students delineate differential diagnoses and treatment options in an adult patient with similar complaints
- Practice correspondence skills by having students write reports to other providers, including pediatricians, dermatologists and psychologists
Discussion
Trichotillomania, from the Greek trikhos (hair), tillein (to pull out, to pluck), and mania (madness), is classified in the fifth edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as a body-focused repetitive behavior of pulling out of one’s hair, resulting in hair loss. It falls under “Obsessive-Compulsive and Related Disorders,” but is not exclusively related to obsessive-compulsive disorder (OCD). In older editions of the DSM text, TTM was described as a manifestation of OCD and was treated as such. However, in the DSM-5, a distinction is made, though the connection remains.1
There are five diagnostic criteria that help describe the condition: (1) repetitive pulling out of one’s hair, resulting in hair loss, (2) repeated attempts to decrease or stop hair pulling, (3) the hair pulling causes clinically significant distress or impairment in social, occupational, or other important areas of functioning, (4) the hair pulling or hair loss is not attributable to another medical conditions (e.g. a dermatological conditions), and (5) the hair pulling is not better explained by the symptoms of another mental disorder (e.g. attempts to improve a perceived defect or flaw in appearance in body dysmorphic disorder).1
In very young patients who pull their hair out, the pulling usually takes place beyond the child’s consciousness and is termed “automatic.” It is often compared to a self-soothing strategy, such as thumb sucking, which the child will eventually outgrow. If the TTM manifests at puberty or during the teenage years, there tends to be a split between automatic pulling and purposefully pulling out one’s hair, or “focused” pulling. As patients approach early adulthood and adulthood, the pulling tends to drift more toward exclusively focused. Adult patients with TTM have a poorer prognosis, as the underlying cause of the pulling tends to be more psychological.2
It was once believed that the adult-type style of hair pulling was universal among all persons experiencing TTM. Traditionally, the act of pulling was preceded by a buildup of stress, angst, or anxiety, and was followed by an immense feeling of relief. However, as more attention is paid to the rare and unique condition, it has become apparent that children do not experience that same emotional cycle of angst and relief. It is thought that this is because young children do not have the mental expressivity or emotional capacity to recognize the urges that adults readily experience.4 In older adolescence, of course, education- and social-related stress can be experienced.
Lewin et al found that among 133 youths aged 10 to 17 with TTM, 45% reported symptoms of depression and 40% reported symptoms of anxiety.5 In this study, older children reported more severe symptoms, and earlier age of onset was also correlated to more severe reported symptoms. While our patient did not report any feelings of anxiety or depression, a consultation with a psychologist or psychiatrist was an option for future referral.
The patient discussed in this case report solely pulled her eyelashes, but this is not the most common place from which those with TTM pull. One study reported that a large majority of children aged 8-17 with TTM pull from their scalp (73%), mostly on their dominant side.6 Eyelash pulling still accounts for a sizable percentage of hair pulling at 39%. Almost half of the participants of this study reported pulling from more than one site. Other pulling sites include eyebrows (32%), other body hair (10%) and even pubic hair (5%).
This knowledge complicates this case, as the patient was experiencing scalp hair loss/thinning as well. First, it is plausible that the patient was withholding the fact that she was pulling from her scalp as well. However, she was very mature for her age and had no reason to lie regarding her hair issues. Additionally, her scalp hair loss appeared to be more diffuse than focal. These facts support the diagnosis of telogen effluvium for her scalp and trichotillomania for her eyelashes.
There is no accepted standard of care for the treatment of TTM in adults or children, but there is a convergent consensus in the psychology and psychiatry community that cognitive behavioral therapy (CBT), also known as habit reversal training (HRT) is the first line treatment.7 However, there is a lack of practicing clinicians experienced in CBT specifically for TTM and thus, older, less effective treatment are often prescribed. Since the disorder was erroneously and almost exclusively linked to psychiatric conditions, pharmacological therapy with selective serotonin reuptake inhibitors (SSRIs) was the mainstay of treatment decades ago. Recent studies dispute this notion, proving that SSRIs have no greater effect than placebo.3
In adults, several medications have been studied as possible treatments for TTM. The opioid antagonist naltrexone, which is used in the treatment for addiction (e.g., alcoholism, gambling addiction), provides a reduction in pulling behaviors and urges in adult patients and the use of the drug was not associated with any major side effects.8 The oral medication olanzapine, an atypical neuroleptic, has also been found to be superior to placebo in decreasing the frequency of hair pulling in adults, but was associated with significant unfavorable side effects.9 One of the most recent and promising pharmacological treatments for TTM in adults is N-acetylcysteine (NAC), which is an over-the-counter mucolytic agent with glutamate modulating properties. Not only has a recent study found that NAC was significantly superior to placebo in reducing hair pulling and urges in adults with TTM, but the reduction rates were comparable to the most effective known treatment, CBT.10 Further, the supplement has a rather favorable side effect profile and is readily available in health food stores. However, when NAC was studied in children, the study participants did not respond as positively as adults did in terms of reduction in hair pulling behaviors when compared to the placebo group.11 In this study, 25% of NAC-treated children and 21% of placebo-treated children were judged as treatment responders and the difference was not significant. Peabody et al proposed using bimatoprost (Latisse®, Allergan; Irvine, CA), a prostaglandin analog with positive effects on eyelash growth, in patients with eyelash trichotillomania to grow lashes back faster. Although this may seem counterintuitive, the authors recommended only using the drug in patients whose mania has been under control, either with medication or after successful CBT. They quoted the benefits of improving patients’ self-image, reinforcing compliance and serving as an importance adjunctive therapy in the treatment of TTM.12
As evidenced by NAC, described above, childhood TTM responds very differently to medical treatment. Many of the promising therapies for adults have been shown to have little or no effect on children. This is not terribly surprising, as the mechanism behind most children’s automatic hair pulling is different from adults’ conscious focused pulling.
The most effective form of treatment for adults and children alike with TTM is cognitive behavior therapy, concentrating on habit reversal. Adults with TTM have been treated with CBT since the 1980s13,14 and one substantial problem that is encountered is relapse. Keijsers et al found that their study participants experienced a dramatic reduction in both the urge to pull and actual pulling after treatment and an increased ability to resist the urge starting at the second therapy session.15 The initial improvements in the study were maintained through the 6-week duration of therapy in all patients. Unfortunately, at the 3-month and 2-year follow-up interviews, the progress the patients had made had decreased by 49% and 70%, respectively, compared to post-treatment levels. The researchers also found that only pre-treatment levels of depression uniquely predicted the 2-year follow-up results. The results of this important study dictate the need for strict and regular follow-up for all TTM patients, likely for life. As in the case of many addictions, the urges that plague these patients at the height of their affliction may resurface at any time throughout the rest of their lives.
The first open trial of CBT for TTM in the pediatric population was not published until 2007. Tolin et al found that 77% of participants were classified as “treatment responders,” and 32% were “excellent responders.”16 Six-month follow-up numbers were expectedly lower, with 63% and 32%, respectively. Still, this study gave support to further study of cognitive behavioral therapy for the treatment of TTM in the pediatric population. Similar results were found by Franklin et al, with 75% of the CBT study participants were classified as treatment responders, compared to 0% of the control group.17 This finding was sustained when symptoms were reassessed after 8 weeks. This absence of relapse was in stark contrast to other trials of adults with TTM, but the authors were not hasty in assuming that relapse was not a problem in the pediatric population. These results supported the importance of treating TTM in childhood, as the probability of a life free from hair pulling was more favorable if treated earlier in life.
Using the published literature as a guide, the treatment and management of this patient was focused on improving signs and symptoms of the underlying ocular disorder (blepharitis and dry eye), while utilizing the treatment itself as HRT to directly compete with the act of pulling out eyelashes (lid scrubs). The patient’s pediatrician was involved during the entire process and a psychology referral was discussed repeatedly with the patient and her family. Close, careful follow-up was used to monitor for relapse and, when it occurred, adjust the management plan.
These advances in the therapeutic treatment of TTM in the pediatric population are good news, but this line of treatment is often not accessible to TTM sufferers. Many clinicians do not practice CBT nor incorporate HRT into their treatment.18 However, over the past 10 years, a growing consensus in the pediatric, dermatologic and psychological communities stresses behavioral approaches for the youngest sufferers, augmenting with pharmacotherapy in older adolescents with associated psychiatric disorders.7
Finally, it is important to appreciate the interprofessional nature of the care of patients with TTM. After repeated suggestions, the patient’s family declined a psychology referral for their daughter. For whatever reason they declined, another professional’s opinion on the case would have been helpful. The optometrist’s patient education may be the only professional guidance a patient receives, so one must ensure that they educate thoroughly.
Differential Diagnosis
The leading differential diagnosis for the patient’s eyelash loss was trichotillomania (TTM), or the compulsive pulling out of hair (or eyelashes), resulting in noticeable hair loss. The patient’s self-admitted history of pulling out her eyelashes due to eyelid itching led to the diagnosis of eyelash trichotillomania secondary to moderate anterior and posterior blepharitis. Though the history made this diagnosis the most probable, differentials should still be considered. Additionally, a full social history should be taken from the patient and their guardians to rule out forms of abuse that may be leading to the behavior. In cases where subjective complaints conflict with objective findings, the possibility of abuse must be considered. As with any psychological condition in children, the pediatrician should be involved in all aspects of management as well. One must remember that optometrists are mandated reporters of child abuse, and any suspected signs of abuse should not be ignored.
Differential diagnoses for the patient’s madarosis included telogen effluvium (TE), alopecia areata (AA) and trichotillomania of the eyelashes.
Telogen effluvium is the premature entry of hair cells into the telogen phase of the hair growth cycle, which is resting phase. These hairs will then shed at a rate three times faster than normal healthy hair and mainly affects the scalp. The hair is often described as coming out “in clumps” with daily brushing or in the shower. There are many known causes of this condition and the commonality between them all is physical or mental stress. Examples of physical stress known to cause TE include high fever, surgery, pregnancy or childbirth, hospitalization, hemorrhage, crash diets, eating disorders and contact dermatitis caused by hair dyes. Emotional stress, such as death of a loved one, loss of a job, or any significant change in one’s life may trigger acute TE as well. Additionally, myriad systemic conditions may cause TE, such as thyroid conditions, iron deficiency, pancreatic disease, systemic lupus erythematosus, HIV-1 infection and general dietary inadequacy. Several drugs are known to cause TE, like anticonvulsants, anticoagulants, anti-thyroid agents, lithium, lamotrigine and the HPV vaccine.19 The patient was not taking any medications and reported no medical conditions. Although telogen effluvium does not normally affect the eyelashes, this differential diagnosis must be considered for the patient’s scalp hair loss.
Alopecia areata (AA) is a medical condition in which hair is lost in round patches, usually from the scalp. The etiology is thought to be an autoimmune attack on hair follicles, but the exact mechanism in unknown. The classic presentation of remaining hair is what is referred to as “exclamation mark hairs.” The distal part of the hair shaft is of normal caliber, while the proximal part is thinned toward the follicle, resembling an exclamation mark. This condition was ruled out due to the diffuse nature of the scalp hair loss. AA can affect other sites of the body and isolated eyelash AA exists as well. Isolated eyelash AA was ruled out due to the patient’s self-admitted pulling out of her eyelashes. Alopecia totalis is the loss of all head hair (scalp, eyebrows and eyelashes), but this was ruled out due to the diffuse loss of scalp hair and normal thickness of her eyebrows. For the same reasons, alopecia universalis, or the loss of all body hair, was also ruled out.20,21
Teaching Methodology and Assessment
This case report is appropriate for third- and fourth-year optometry students and optometric residents who have completed didactic course work in conditions affecting the eyelids and lashes and can apply that knowledge to the clinical setting. The case can be used to emphasize the importance of a thorough case history, including social aspects of patients’ lives. Further, a spotlight on co-management of patients with other health professionals is reinforced. If a patient does not follow through with a referral, effective patient education is crucial in this case.
The case report can be delivered to students and/or residents in a grand rounds or case discussion format, in a didactic setting or clinical discussion in pediatrics or anterior segment clinics. Utilizing problem-focused instruction, learners can concentrate on the patient’s complaint of madarosis and explore various causes and management options to address this unique complaint. Using case-focused instruction, learners can use their foundational knowledge of eye care, supplemented by additional phycological and dermatological information from the instructor, to find out-of-the-box solutions using their analytical skills. Students and residents should be able to talk through the analysis of signs and symptoms, development of differentials, as well as the optometric and co-management of the condition.
Assessment of learners’ understanding of the key concepts can include discussion of how management would differ if some details of the case were different, such as if the patient did not admit to pulling her lashes. Learners should be able to objectively describe the presentation of the condition captured by slit lamp photos included in the report. The follow-up photos can then be used to assess whether learners can appreciate and describe the progress in resolution of the madarosis. Finally, interprofessional correspondence can be practiced by asking students to write referral letters to different medical professionals involved in the care of this patient.
Conclusion
This case emphasizes the importance of considering systemic and psychological differential diagnoses of madarosis presenting in a pediatric patient. Though pediatric TTM is rare, the cause of the patient’s removal of her eyelashes is not. The author has also encountered eyelash TTM secondary to moderate allergic conjunctivitis. A thorough medical and social history is important in differentiating the cause of madarosis. Co-management with pediatrics, dermatology and psychology or psychiatry was critical to correct diagnosis and management and the patient’s overall wellbeing. For children experiencing TTM, CBT with a mental or behavioral health provider focusing on habit reversal and relapse prevention is the ideal treatment.
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders : DSM-5-TR. Fifth edition, text revision. ed. American Psychiatric Association Publishing; 2022:pages cm. doi: 10.1176/appi.books.9780890425787
- du Toit PL, van Kradenburg J, Niehaus DJ, Stein DJ. Characteristics and phenomenology of hair-pulling: an exploration of subtypes. Compr Psychiatry. 2001;42(3):247-56. doi:10.1053/comp.2001.23134
- Bloch MH, Landeros-Weisenberger A, Dombrowski P, et al. Systematic review: pharmacological and behavioral treatment for trichotillomania. Biol Psychiatry. Oct 15 2007;62(8):839-46. doi:10.1016/j.biopsych.2007.05.019
- Harrison JP, Franklin ME. Pediatric trichotillomania. Curr Psychiatry Rep. Jun 2012;14(3):188-96. doi:10.1007/s11920-012-0269-8
- Lewin AB, Piacentini J, Flessner CA, et al. Depression, anxiety, and functional impairment in children with trichotillomania. Depress Anxiety. 2009;26(6):521-7. doi:10.1002/da.20537
- Panza KE, Pittenger C, Bloch MH. Age and gender correlates of pulling in pediatric trichotillomania. J Am Acad Child Adolesc Psychiatry. Mar 2013;52(3):241-9. doi:10.1016/j.jaac.2012.12.019
- Melo DF, Lima CDS, Piraccini BM, Tosti A. Trichotillomania: What Do We Know So Far? Skin Appendage Disord. Jan 2022;8(1):1-7. doi:10.1159/000518191
- De Sousa A. An open-label pilot study of naltrexone in childhood-onset trichotillomania. J Child Adolesc Psychopharmacol. Feb 2008;18(1):30-3. doi:10.1089/cap.2006.0111
- Van Ameringen M, Mancini C, Patterson B, Bennett M, Oakman J. A randomized, double-blind, placebo-controlled trial of olanzapine in the treatment of trichotillomania. J Clin Psychiatry. Oct 2010;71(10):1336-43. doi:10.4088/JCP.09m05114gre
- Grant JE, Odlaug BL, Kim SW. N-acetylcysteine, a glutamate modulator, in the treatment of trichotillomania: a double-blind, placebo-controlled study. Arch Gen Psychiatry. Jul 2009;66(7):756-63. doi:10.1001/archgenpsychiatry.2009.60
- Bloch MH, Panza KE, Grant JE, Pittenger C, Leckman JF. N-Acetylcysteine in the treatment of pediatric trichotillomania: a randomized, double-blind, placebo-controlled add-on trial. J Am Acad Child Adolesc Psychiatry. Mar 2013;52(3):231-40. doi:10.1016/j.jaac.2012.12.020
- Peabody T, Reitz S, Smith J, Teti B. Clinical management of trichotillomania with bimatoprost. Optom Vis Sci. Jun 2013;90(6):e167-71. doi:10.1097/OPX.0b013e318294c158
- Azrin N, Nunn R, Frantz S. Treatment of hair pulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exper Psychiatry. 1980;11(11):13-20.
- Ninan PT, Rothbaum BO, Marsteller FA, Knight BT, Eccard MB. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. Jan 2000;61(1):47-50. doi:10.4088/jcp.v61n0111
- Keijsers GP, van Minnen A, Hoogduin CA, Klaassen BN, Hendriks MJ, Tanis-Jacobs J. Behavioural treatment of trichotillomania: two-year follow-up results. Behav Res Ther. Mar 2006;44(3):359-70. doi:10.1016/j.brat.2005.03.004
- Tolin DF, Franklin ME, Diefenbach GJ, Anderson E, Meunier SA. Pediatric trichotillomania: descriptive psychopathology and an open trial of cognitive behavioral therapy. Cogn Behav Ther. 2007;36(3):129-44. doi:10.1080/16506070701223230
- Franklin ME, Edson AL, Ledley DA, Cahill SP. Behavior therapy for pediatric trichotillomania: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. Aug 2011;50(8):763-71. doi:10.1016/j.jaac.2011.05.009
- Franklin ME, Zagrabbe K, Benavides KL. Trichotillomania and its treatment: a review and recommendations. Expert Rev Neurother. Aug 2011;11(8):1165-74. doi:10.1586/ern.11.93
- Grover C, Khurana A. Telogen effluvium. Indian J Dermatol Venereol Leprol. 2013;79(5):591-603. doi:10.4103/0378-6323.116731
- Islam N, Leung PS, Huntley AC, Gershwin ME. The autoimmune basis of alopecia areata: a comprehensive review. Autoimmun Rev. Feb 2015;14(2):81-9. doi:10.1016/j.autrev.2014.10.014
- Modjtahedi BS, Kishan AU, Schwab IR, Jackson WB, Maibach HI. Eyelash alopecia areata: case series and literature review. Can J Ophthalmol. Aug 2012;47(4):333-8. doi:10.1016/j.jcjo.2012.04.013

