
PEER REVIEWED
Faculty Perceptions of the Impact of Electronic Medical and Health Records in Optometric Education in the United States and Puerto Rico
Aurora Denial OD, FAAO, Daniel Bastian OD, FAAO, Gary Chu, OD, MPH, FAAO, and Amy Moy OD, FAAO
Abstract
Digital records, i.e., electronic health records (EHRs) and electronic medical Records (EMRs) are the current standard for documenting healthcare information. The purposes of this exploratory study were to gather information about the use of digital records in academic optometric settings in the United States and Puerto Rico and to assess faculty perceptions of the potential impact and implications of digital records in the teaching and learning process. The results indicated that most students have authority to enter data into the majority of the digital record. Potential influences of digital records in teaching and learning were identified in the areas of time for documentation, development of clinical reasoning, and student behaviors.
Key Words: electronic medical records, electronic health records, digital records, optometric education
Introduction
In 2001, the Institute of Medicine, which was established by the National Academy of Sciences as an independent advisory organization, advocated for the extensive use of information technology that would “lead to the elimination of most handwritten clinical data by the end of the decade.”1 This information technology (digital records) became known as electronic health records (EHRs) and electronic medical Records (EMRs). EMRs are digital medical records that contain the standard medical and clinical data collected in one provider’s office.2 EMRs were designed to reduce medical errors and improve quality of care.1 Although the content can vary, most EMRs include clinical documentation (notes), patient data (demographics, lab results, problem/diagnosis list, medication list, psychosocial history, other test results), computerized order entry for medications and tests, clinical messaging, and decision support systems (alerts, warnings, reminders).3 EHRs are a digital collection of individual office visits (EMRs) and other health information. EHRs go beyond the information collected by one office or provider.2 EHRs can be shared and provide information about an individual or populations.2 As such they have the potential to enhance clinical care and impact research, public health policies and education.4
Digital records are a tool for documenting healthcare information and data used in caring for a patient. An important question to ask is whether this tool goes beyond documentation and has an impact on other areas such as student learning. Clinical reasoning, the cognitive process that clinicians use to care for patients, is based on data, information and evidence.5 Clinical reasoning can be defined as “thinking through the various aspects of patient care to arrive at a reasonable decision regarding the prevention, diagnosis or treatment of a clinical problem in a specific patient.”5 The digital record is a new method of documenting the data and information that can be used to drive the clinical reasoning process of clinicians.
Statistical data have shown a widespread increase in the use of digital records among healthcare providers and hospitals over the past few years.6,7 The Office of the National Coordinator for Health Information Technology reported in 2015 that 3 out of 4 (76%) non-federal acute care hospitals had adopted at least a basic digital record, and more than 8 out of 10 (83%) physicians had adopted a digital records system.6,7
Digital records are also becoming commonplace in academic healthcare settings.8-10 In recent years, all optometric education institutions in the United States have implemented a digital record system in at least their main academic clinics.11 In medical education, several advantages and disadvantages of increased digital records use have been identified. Advantages include ease of reviewing notes, availability of information, medical support tools, ease of organizing notes, and potential use of patient registries.8 Disadvantages include increased time spent charting, impact on clinical reasoning, impact on the development of student/patient rapport, and information overload.8
There is a paucity of information available about the use of digital records in optometric education. A search of PubMed, Medline, and VisionCite using the MeSH terms “electronic medical record” or “electronic health record” and “optometry teaching environments” or “optometric health care education” yielded no relevant articles. The purposes of this exploratory study were to gather information about the use of digital records in academic optometric settings in the United States and Puerto Rico and to assess faculty perceptions of the potential impact and implications of digital records in the teaching and learning process.
Methods
All faculty members who were listed in the Association of Schools and Colleges of Optometry database as having clinical responsibilities were eligible for inclusion in the study. In May 2016, a link to a survey was e-mailed to 790 optometric faculty members who met the inclusion criteria. The survey consisted of 35 questions and sought information about the demographics of faculty users of digital records, and about the implementation, use and impact of digital records in clinical education. Seven of the questions were multiple-choice, four of the questions required a yes/no response, and 21 of the questions required a response along a four-point Likert-type scale (1 = strongly disagree; 2 = disagree; 3 = agree; 4 = strongly agree). A comment section was included.
Instrumentation
The survey was initially developed from a review of the literature and the investigators’ clinical experience. A draft of the survey was fine-tuned by a focus group consisting of five clinical educators from the New England College of Optometry. The focus group refined questions and provided feedback on the readability and soundness of each question. To aid in simplicity, the terms EMR and EHR were used interchangeably in the survey. The intention was for faculty to reflect on the digital records used in their clinical setting. The survey was administered via the web-based system SurveyMonkey®. The survey was re-sent to all potential participants two weeks after the initial deployment. The formatting of the survey by SurveyMonkey® ensured that each participant could only respond once. Information obtained by the survey was confidential and anonymous. The survey is shown in Appendix A.
Data analysis
All data analysis was conducted using IBM SPSS version 25 (Chicago, IL) with alpha set at p < 0.05. Measures of central tendency were conducted for all continuous variables, and percent and proportions were calculated for all categorical variables. Within-subjects analysis of variance with the Bonferroni technique to control for inflated Type I error was employed to determine differences among survey items. A series of Spearman’s rho correlations was conducted to determine the relationships between items from the survey and the following demographic variables: (a) age, (b) years practicing optometry, (c) years using EMRs, (d) number of clinical students, and (e) months using the current EMR system. Results of the a priori power analysis using G*Power (V3.1) software indicated a sample of N = 67 to achieve a moderate effect size of 0.30 with a 0.80 power and alpha set at p < 0.05 (two-tailed). The comments were analyzed using a grounded theory approach. The authors identified relevant comments with emerging themes and reached a consensus on the themes.
The study was reviewed by the Institutional Review Board at the New England College of Optometry and given an exempt status.
Results
The final overall response rate for the survey was 34% (265) of the clinical faculty members from optometry schools in the United States and Puerto Rico. The assumptions for linearity and normality were met for all variables.
 Table 1. |
 Table 2. |
 Table 3. |
The median age of the respondents was between 36-45 years (mean 44 years). Respondents had 4-7 years of digital record experience. Thirty-two percent of the respondents had been practicing for more than 25 years. Eighty-seven percent of the respondents practiced in an optometric institution’s eye clinic, 11% in a community health center, and 2% in a private practice setting. The Compulink system was the most used overall (48%). Eighty-six percent of the respondents reported using digital records specifically designed for eye care, and 96% reported using paper charts in the past. The majority of participants (66%) indicated that they felt students were well-trained in the use of digital records before arriving in clinic, and 84% indicated that students were exposed to using a digital record system in the preclinical environment. Most faculty (78%) reported being comfortable using their current digital record, and 69% reported not receiving formal training in the use of digital records as a teaching tool. The majority of respondents (85%) reported that students had authority to enter data into the EMR; 91% reported students could enter medication updates; 93% reported students could enter allergies; and 89% reported students could enter tests and interpretations. This data is shown in Table 1.
Statistically significant differences were found among the challenges in using digital records in a teaching environment F(5, 259) = 79.52, p < 0.001, η2 = 0.62. Pairwise comparisons using the Bonferroni technique to control for inflated Type I error indicated that time for documentation is the greatest challenge, while too much data is the least challenging. Descriptive statistics related to challenges in using digital records are presented in Table 2. Statistically significant differences were also found among the advantages in using digital records in a teaching environment F(3, 262) = 128.96, p < 0.001, η2 = 0.60. Pairwise comparisons using the Bonferroni technique indicated that legibility of records and ability to access past records easily are the greatest advantages, while use of templates is the least advantageous. Descriptive statistics related to advantages in using digital records are presented in Table 3.
The majority of faculty (74%) reported that time spent by students and faculty for documentation in the digital record takes away from time spent teaching. Respondents were split 50/50 on the perception of a digital record as a useful learning tool. The majority (78%) did not agree with the statement “The EHR has positively impacted my enthusiasm for teaching.”
Fifty-eight percent of the respondents perceived that the inherent prompts (i.e., templates) and layout of a digital record system hinder students’ development of clinical reasoning. Fifty-two percent of the respondents reported that they give students their undivided attention including direct eye contact during case presentation. Fifty-nine percent of the respondents did not agree with the statement “As a clinical instructor, I tend to rely more on information from the EHR than a student’s oral case presentation.”
Student behaviors as reported by faculty are impacted by digital records in frequency of copying and pasting data (67%
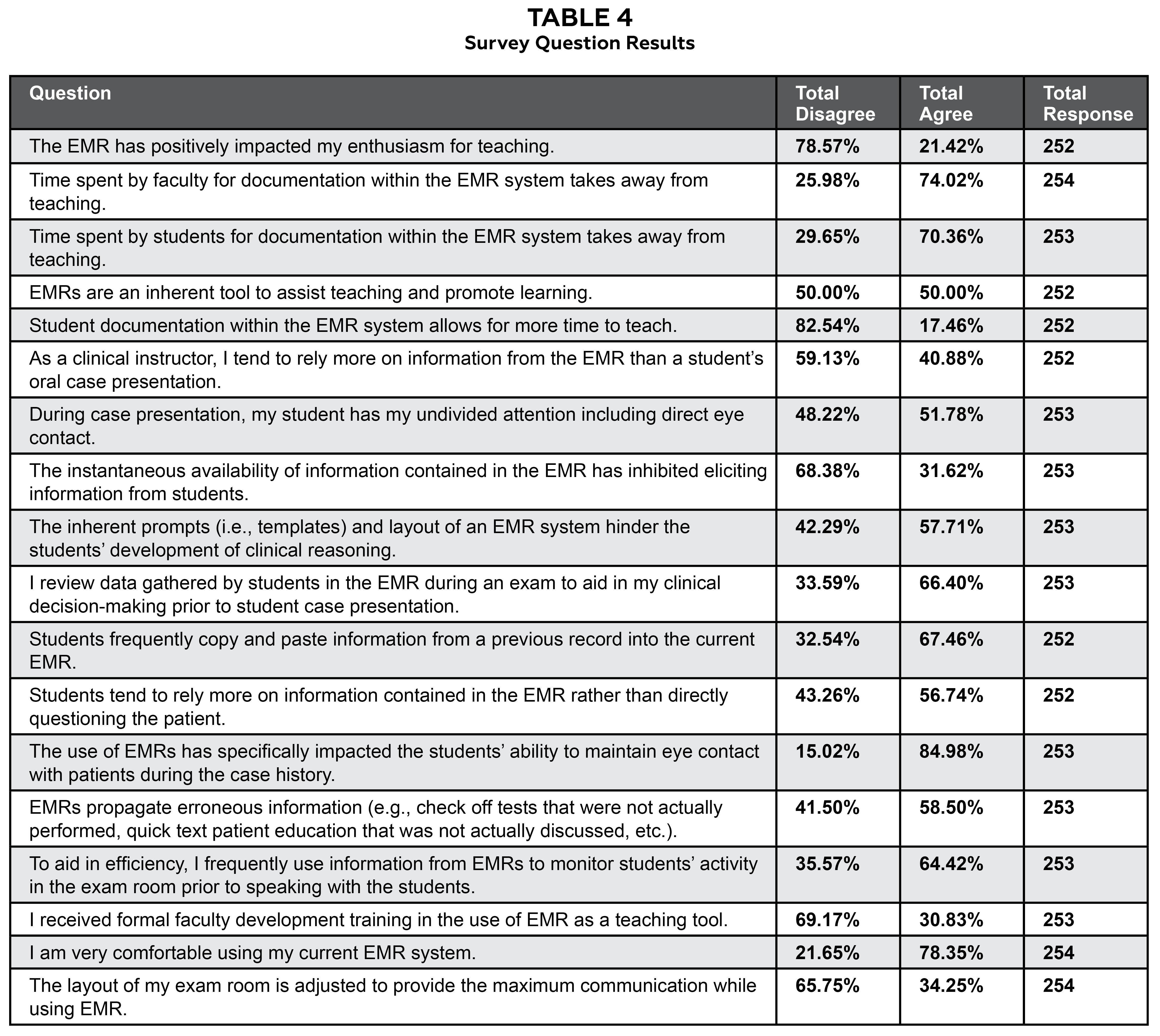 Table 4. |
 Table 5. |
 Table 6. |
agreed), relying more on information contained in the EHR rather than directly questioning the patient (57% agreed), writing before entering data into the computer (62% agreed), and ability to maintain eye contact with the patient during case history (85% agreed). Table 4 lists responses to survey questions. Table 5 lists descriptive statistics.
There were statistically significant correlations between faculty age and their (a) experience using a digital record system, and (b) the number of students they supervise in the clinic at a given time. The relationships between the demographic variables with the items from the survey are shown in Table 6. According to the data, older respondents and those practicing longer are statistically more likely to agree with items Q15 (time spent by faculty for documentation within the EMR system takes away from teaching), Q19 (during case presentation, my student has my undivided attention including direct eye contact), Q26 (the use of EMRs has specifically impacted the students’ ability to maintain eye contact with patients during the case history), and Q29 (I received formal faculty development training in the use of EMRs as a teaching tool).
In addition, longer-time users of digital records are statistically more likely to agree with items Q19 and Q26. However, older respondents are less likely to agree with Q25 (students tend to rely more on information contained in the EMR rather than directly questioning the patient) and Q20 (the instantaneous availability of information contained in the EMR has inhibited eliciting information from students). No statistically significant relationships were found between months using the current EMR system and any of the survey items.
Finally, instructors with more clinical students are statistically more likely to agree with items Q21 (students frequently copy and paste information from a previous record into the current EMR) and Q32 (EMRs propagate erroneous information). In contrast, instructors who were supervising fewer clinical students are statistically more likely to agree with items Q18 (as a clinical instructor, I tend to rely more of information from the EMR than a student’s oral case presentation) and Q22 (to aid in efficiency, I frequently use information from EMRs to monitor students’ activity in the exam room prior to speaking with students).
 Table 7. |
 Table 8. |
Table 7 depicts faculty comments related to teaching and the use of digital records. Qualitative analysis revealed a theme of decreased time for teaching with the use of digital records. Most of the comments expressed the challenges related to teaching and EMRs. However, two comments expressed the advantages of EMRs in teaching. Table 8 depicts comments related to clinical reasoning and the use of digital records. Qualitative analysis revealed a theme of a negative impact on the development of critical thinking related to the use of digital records. All comments expressed a negative sentiment with regards to the development of clinical reasoning skills.
Discussion
The implementation of digital healthcare records in optometric settings has necessitated an evaluation of this method of documentation within the academic setting. In the survey, faculty perceptions of the potential impact and implications of digital records in the teaching and learning process focused on time for clinical teaching, student behaviors, and the development of clinical reasoning. Information gathered about the use of digital records addresses preparing students for success in patient care, which includes appropriate documentation in digital health records and clinical communication.
Student usage of the individual components of digital records
The majority of respondents indicated that students have the authority to enter data into the digital record, including updates of current medications, allergies, and tests and interpretation. Student use of EMRs is an important component in the educational process. The Association of Schools and College of Optometry states, “The school or college of optometry shall ensure that before graduation each student will have demonstrated: effective communication skills, both oral and written, as appropriate for maximizing successful patient care outcomes.”12 Additionally, the Accreditation Council on Optometric Education dictates that the optometric curriculum must prepare graduates for entry level practice, which includes the following standards:
- 2.9.1 The graduate must be able to identify, record and analyze pertinent history and problems presented by the patient.
- 2.9.8 The graduate must be able to effectively communicate orally and in writing with other professionals and patients.
- 8.2.4 The patient record must allow for efficient review of the patient’s condition and any pertinent previous care provided at the program’s clinical facility.13
Appropriate documentation is a learned skill and an essential component of patient care. Students must be given the opportunity to practice and receive feedback in all areas of documentation to ensure they achieve competency by graduation. In medical education, it is an accepted belief that student documentation enhances patient care and the student’s education.14 Gliatto et al. state that “this hands-on experience has provided a way for students to reflect on patient encounters, learn proper documentation skills and attain a sense of being actively involved in and responsible for the care of patients.”15 The survey revealed that in most sections of the digital record students have the authority to enter data. The majority (85%) of optometric sites and instructors give students the authority to document in the EMR. This gives the students the opportunity to learn and practice documentation skills. In contrast, Wittels et al. found that only 63% of emergency medicine clerkships allowed medical students to document a patient encounter.16 These differences may reflect differences in billing policies, patient safety issues or environments (inpatient hospital care vs. outpatient care). According to the survey, optometry students participate less in some sections, such as data for billing, demographics, generating referrals, ordering additional tests, and ordering additional medications, than in other sections. Student documentation in all sections should be encouraged to provide a comprehensive educational experience.
Impact on teaching
Based on the survey responses, time spent on documentation by both students and faculty reduces the amount of time available for clinical teaching. The majority of comments related to teaching loudly echoed a concern for lost teaching time. Older respondents and those practicing longer were more likely to agree that faculty documentation within the digital record takes away from teaching. This may reflect differences in comfort levels related to technology and learning. Most clinical faculty are responsible for providing a high level of patient care, maintaining clinical productivity and educating students. In any given clinical session, there is a limited amount of time. In most clinical environments, a constant high level of patient care while maintaining productivity is necessary to ensure financial stability. Therefore, clinical teaching becomes vulnerable to any reduction in time. An important question to ask is why documentation in digital records is so slow. Slowness in documentation could be attributed to the inherent design of digital records, changes in student behaviors, or inadequate/ineffective training. The survey revealed that most faculty members feel that students are exposed to digital records in the preclinical environment and are well-trained before arriving in clinic. However, the study did not determine the students’ level of skill after training, type of training or the specific amount of time dedicated to training, which may influence the speed of documentation. Student behaviors such as writing findings on paper before entering data into the computer could contribute to a slower and less efficient student. The reasons some students write before entering data was not explored in the study. Theoretically, students may write before entering data because they are not confident in their findings or efficient in the use of the computer or data entry. Seventeen percent of the respondents perceived that student documentation allows more time to teach. This group tended to be younger with less years in practice.
Faculty members were split on the potential use of digital records as a tool for assisting teaching and learning. Younger respondents with fewer years in practice were more likely to agree that digital records are a useful tool to assist in teaching and promote learning. The most significant advantages of digital records identified were ability to access past records, ability to access patient information, and legibility of records. In a national study by Hammoud, these same advantages were identified in medical education.8 Theoretically, these characteristics have the potential to aid in teaching and learning. However, the advantages afforded by digital records may be offset by the perceived loss of teaching time.
Student behaviors
Identifying changes in student behaviors related to digital records as perceived by faculty can be helpful in guiding teaching strategies. The ability to maintain eye contact with a patient during case history and the use of the copy and paste features were perceived changes in student behavior related to the use of digital records. Faculty who were older, practiced longer and had been using digital records longer were more likely to agree with the students’ loss of eye contact. Most faculty agreed that the design of the exam room had not been adjusted to maximize communication while using a digital record. Faculty who felt that the layout of the exam room had been modified tended to be younger with fewer years in practice. The ability to communicate and develop a relationship with the patient is an essential tool in rendering a high level of patient care.17 Poor eye contact while using digital records reflects poor communication skills and may impact the development of rapport with the patient.18 Students in the preclinical environment need to develop and practice communication skills that allow for the gathering of appropriate data while fully maintaining eye contact and efficiently entering data into the digital record. Suggestions for improving eye contact may include altering exam room layout to maximize communication, instructing the student to look at the patient and move away from the keyboard during the case history, and using defined breaks from conversations with patients to enter data.
The tendency for students to copy and paste information was perceived by a majority of survey respondents. This has serious consequences related to ethics, medical errors and propagation of incorrect information. In 2001, a study within the Veterans Administration System revealed that “20% of notes showed evidence of copying with an average of 1.01 errors per copied note.”19 In a 2009 physician survey, 90% of the physicians who wrote notes used the copy and paste function.20 In optometric education, anecdotal information indicates that many students copy and paste information as a means of decreasing documentation time. In clinic, students are learning and it is the clinical instructor’s job to instruct them on the potential negative consequences related to copying and pasting information. All institutions and clinical environments should have a clear policy on copying and pasting during documentation. Unethical practices, poor patient care and increased liability should not be a mere click away.
Clinical reasoning
One of the goals of clinical teaching is the development of clinical reasoning. Faculty perceived digital records to impact the development of clinical reasoning in three areas: student reliance on templates, use of copy and paste features, and the presentation of clinical data/thought process. Most digital records contain multiple templates as well as the capability of adding free text. The majority of faculty in this study (58%) perceived digital records to hinder the development of clinical reasoning. This perception was also reiterated in the faculty comments on clinical reasoning. In medical education, a major challenge of digital records was the potential barrier to the development of clinical reasoning skills.8
Clinical reasoning involves gathering, synthesizing, analyzing and critically reviewing information/data. Historically, questioning during the case history allows the clinician to gather information, generate an initial hypothesis and refine the hypothesis based on a patient’s response. The use of templates can impact reasoning because questions are asked as dictated by the template and not by the student’s thought process. Therefore, and in order to ensure that a student is applying clinical reasoning, faculty should challenge the student’s thought process to demonstrate that adequate skill, advancement and progression are achieved.
Another potential barrier to the development of clinical reasoning skills is the copying and pasting of information, specifically the assessment/diagnosis and management. The majority of faculty agreed in the survey that students utilize this feature. Respondents with more students to supervise were more likely to agree that students too frequently copied and pasted information from a previous record into the current digital record. Perhaps faculty with more supervisees are more exposed to repetitious notes and thus are more able to detect frequent copying and pasting. The final assessment/diagnosis and management lists represent coming to a conclusion by gathering, analyzing and evaluating appropriate information, examining assumptions and identifying any biases. If students are allowed to copy and paste this part of the note, it may negatively influence the development of clinical reasoning skills.
Student case presentation represents the oral presentation of data and a student’s clinical reasoning.21 A majority of faculty (64%), especially those who were younger with fewer years in practice, indicated using digital records to get information to monitor a student’s activity, and (66%) indicated using digital records to aid in instructor decision-making before student case presentation. Additionally, 59% of the respondents reported relying on information from the student’s oral case presentation rather than the digital record, and 52% indicated that students have the clinical faculty member’s undivided attention during case presentation. As an educational tool, case presentation allows the clinical instructor the opportunity to gain insight into a student’s reasoning while allowing the student the opportunity to perfect the skill. In medicine, case presentation can take 2-7 minutes.21 Clinical faculty often balance the more efficient acquisition of information from a digital record with the educational experience of case presentation. Student need, productivity requirements and patient care may dictate during any given patient encounter where and how information is acquired. In the survey, age, years in practice and years using digital records were associated with providing undivided attention to students, which suggests that experienced clinicians might more easily recognize the value and educational benefit of case presentation.
Interestingly, respondents with fewer students were more likely to rely on information from the digital record than on the student’s oral case presentation. One possible explanation is that faculty with fewer students may have a better understanding of their students’ abilities and can with greater confidence simply rely on the digital record rather than investing in the time of an oral case presentation. This explanation is partially supported by the fact that respondents with fewer students are also more likely to use information from the digital record to monitor students’ activity in the exam room prior to speaking with students.
The goals of clinical faculty are to educate and take care of patients. The value of case presentation must be recognized and balanced with the efficient acquisition of information.
Limitations of the study
The study was limited by the sample size, lack of data related to respondents’ specific institution, blurring of the terms EMR and EMR in the survey, and lack of specificity in some of the questions. The overall response rate to the survey was 34%, representing 265 respondents. The individual response rate for each question varied between 265-252 respondents because a response to each question was not mandatory to complete the survey. There is no agreement in the literature on acceptable response rates.22 However, response bias or non-response error is always more of a risk with a lower response rate.22 Data were not collected related to the name of each respondent’s institution. This may have introduced a bias if, for example, a large number of faculty from one institution responded. In the survey, the participants were instructed to use the terms EHR and EMR interchangeably. Although the digital record that most faculty are completing after each encounter is an EMR, the interchangeable use of the terms may have blurred the specific components of the digital record that were impacted. In hindsight, more specificity in some of the questions such as the length and type of training received by students and faculty, level of expertise in using digital records, type of data or text that students copy and paste, and the specific level of impact on enthusiasm for teaching would have been helpful.
Conclusion
Digital records constitute the present and future landscape of health care and have become a vital component of clinical care. The results of this study indicate that students have authority to use several parts of the digital record. Further, the results indicate that time related to documentation within digital records impacts the educational process. Additionally, the study indicates that faculty perceive digital records as having an impact on student behaviors and the development of clinical reasoning skills. Age, years in practice and years using digital records are indicators for the perception of faculty documentation affecting teaching time, providing undivided attention to students during case presentation, and the perception of an impact in student eye contact with patients. To maximize use of digital records in patient care and clinical education, tools such as educational guidelines and template assistance need to be developed to guide faculty and students during the teaching and learning process. The study raises several issues for future investigation, including what specifically about digital records takes more time, whether the training and skill level of students impact the time for documentation, whether digital records impact enthusiasm for clinical optometric teaching, what specific type of training is received by faculty, what is the impact of the training, how template design impacts the development of clinical reasoning skills. In an effort to develop educational strategies, future areas of research may include students’ perception of digital records, Medicare compliance, ethics and medical errors, implementation strategies and lessons learned from past experiences.
Acknowledgments
We extend gratitude and appreciation to the members of our focus group who provided insight and comments for the survey: Drs. Crystal Lewandowski, Judith Darrow, Thomas Andrea, Meng Meng Xu and James Aylward.
Special thanks to Elena Bilodeau for technical assistance and Taylor Cleland and Sophia Koevary for editing.
Data from this study were presented at the 2016 American Academy of Optometry Annual Meeting in Anaheim, Calif.
References
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the quality chasm: using information technology. Washington (DC): National Academies Press, 2001. Available from: https://www.ncbi.nlm.nih.gov/books/NBK222274/.
- Health IT and health information exchange basics [Internet]. Washington, DC: Health IT.Gov; c2014 [cited 2016 Feb 23]. Available from: https://www.healthit.gov/providers-professionals/electronic-medical-records-emr.
- Keenan CR, Nguyen HH, Srinivasan M. Electronic medical records and their impact on resident and medical student education. Acad Psychiatry. 2006 Nov-Dec;30(6):522-527.
- Institute of Medicine Committee on Data Standards for Patient Safety. Board on Health Care Services. Key capabilities of an electronic health record system: letter report. Washington, DC: National Academies Press, 2003. Available from: https://www.ncbi.nlm.nih.gov/books/NBK216105/.
- Hawkins D, Elder L, Paul R. The Thinker’s Guide to Clinical Reasoning. Dillon Beach CA: Foundation for Critical Thinking Press; 2010, P. 3-5.
- Charles D, Gabriel M, Searcy T. Adoption of electronic health record systems among U.S. nonfederal acute care hospitals: 2008-2014 [Internet]. Washington (DC): National Coordinator for Health Information Technology, c2015 [cited 2016 Feb 23]. Available from: https://www.healthit.gov/sites/default/files/data-brief/2014HospitalAdoptionDataBrief.pdf.
- Heisey-Grove D, Patel V. Any, certified, and basic: quantifying physician EHR adoption through 2014 [Internet]. Washington (DC): National Coordinator for Health Information Technology: c2015 [cited 2016 Feb 23]. Available from: https://www.healthit.gov/sites/default/files/briefs/oncdatabrief28_certified_vs_basic.pdf.
- Hammoud MM, Margo K, Christner JG, Fischer SH, Pangaro LN. Opportunities and challenges in integrating electronic health records into undergraduate medical education: a national survey of clerkship directors. Teach Learn Med. 2012;24(3):219-24.
- Mintz M, Narvarte HJ, O’Brien KE, Papp KK, Thomas M, Durning SJ. Use of electronic medical records by physicians and students in academic internal medicine settings. Academic Medicine. 2009 Dec;84(12):1698-704.
- Hammoud MM, Dalymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med. 2012;24(3):257-66.
- Chu, Gary. Conversation with David Durkee, OD. July 10, 2016.
- Smythe J, Daum K. Attributes of students graduating from schools and colleges of optometry: a 2011 report from the Association of Schools and Colleges of Optometry. Optometric Education. 2011;37(1):5-10.
- Accreditation Council on Optometric Education. Professional optometric degree standards adopted by the Accreditation Council on Optometric Education (ACOE) at the ACOE Winter Meeting, Feb 19-21, 2016, Addendum 1 [cited 2017 Oct 23]. Available from: https://www.aoa.org/Documents/students/OD_Manual_08_2014_with_2017_standards_attached.pdf.
- Friedman E, Sainte M, Fallar R. Taking note of the perceived value and impact of medical student chart documentation on education and patient care. Acad Med. 2010 Sep;85(9):1440-4.
- Gliatto P, Masters P, Karani R. Medical student documentation in the medical record: is it a liability? Mt Sinai J Med. 2009 Aug;76(4):357-64.
- Wittels K, Wallenstein J, Patwari R, Patel S. Medical student documentation in the electronic medical record: patterns of use and barriers. West J Emerg Med. 2017 Jan;18(1):133-136.
- Stewart MA. Effective physician-patient communication and health outcomes: a review. CMAJ. 1995 May 1;152(9):1423-33.
- Richter Ettinger E. Professional Communications in Eye Care. Butterworth-Heinman 1993; pages 43-45.
- Weir CR, Hurdle JF. Felgar MA, et al. Direct text entry in electronic progress notes. An evaluation of input errors. Methods Inf Med. 2003;42(1)61-7.
- O’Donnell HC, Kaushal R, Barrón Y, et al. Physicians’ attitudes towards copy and pasting in electronic note writing. J Gen Intern Med. 2009 Jan;24(1):63-68.
- Wiese J, Saint S, Tierney LM. Using clinical reasoning to improve skills in oral case presentation. Semin Med Pract. 2002 Sept;5(3):29-36.
- Draugalis JR, Coons SJ, Plaza CM. Best practices for survey research reports: a synopsis for authors and reviewers. Am J Pharm Educ. 2008 Feb 15;72(1):11.

Appendix A.
Click to enlarge


