PEER REVIEWED
“No Time to Finish”:
Electronic Health Records Documentation and Time
Daniel Bastian, OD, FAAO, Aurora Denial, OD, FAAO, DipOE, and Anthony J. Guarino, PhD
Abstract
Increased time for charting (documenting) has been found to be an unintended consequence of electronic health records (EHR). The purpose of this survey study was to investigate the perceived impact of time for charting with EHR on the academic optometric clinical environment. A survey was sent to 800 optometric clinical faculty. Results indicated that time spent on EHR charting is challenging and affects aspects of clinical faculty members’ personal and professional lives.
Key Words: charting, electronic health record, EHR, documentation, optometric education
Introduction
The Office of the National Coordinator for Health Information Technology (ONC) defines electronic health records (EHR) as “digital (computerized) versions of patients’ paper charts.”1 In 2009, the federal government passed the Health Information Technology for Economic and Clinical Health (HITECH) Act, which encouraged widespread adoption of EHR.2 The reasons for encouraging EHR implementation were to reduce medical errors, reduce cost of clinical care through technology and improve quality of care.2 The HITECH Act authorized the Centers for Medicare and Medicaid Services (CMS) to financially incentivize providers and hospitals that used certified EHR.2 The criteria set by CMS for receiving financial incentives were termed “meaningful use.” Doctors and offices able to demonstrate meaningful use received financial payments. In 2015, CMS began administering financial penalties to doctors or hospitals that do not use EHR.2 The healthcare field responded to the rewards and penalties by shifting to a predominately EHR-based documentation process for doctors and hospitals. Positive consequences of the shift included less likelihood of lost records, improved clinical statistics and increased legibility of doctor records. EHRs are now the standard in hospitals and medical offices across the country, including academic healthcare centers.3 EHR are present in all 23 U.S. optometric education institutions, at least in the main academic clinics.4 With EHR ubiquitous in health professions academic settings, an understanding of their impact on the delivery of education, patient care, provider job satisfaction and the workload of optometric educators and providers is needed.
The impact of electronic health records on the delivery of medical education has been investigated. Responding to an anonymous online survey, 59% of 1,515 trainees reported that clinical documentation in EHR decreased the quality of their education.5 Medical residents who responded to the survey reported that documentation requirements were onerous and excessive, and negatively impacted time spent with patients, overall patient care, physician well-being, time available for teaching and quality of resident education.5
Several studies identified increased time spent on electronic charting as an unintended consequence of EHR. A 2017 study involving 471 primary care physicians, Tai-Seale et al. found that over time physicians spent less face-to-face time with patients and allotted more time to EHR charting.6 In 2013, Block et al. reported that interns spent 12% of their time in direct patient care and 40% of their time using computers.7 Holmes et al. reported that increased time spent on EHR contributed to residents’ burnout.8
In optometric education, time spent on documentation was identified as a challenge in the 2018 study “Faculty Perceptions on the Impact of Electronic Medical and Health Records in Optometric Education in the United States and Puerto Rico.”9 Investigators surveyed 265 clinical optometric faculty members and reported a majority of respondents perceived time spent by students and faculty for documentation in digital records took away from time spent teaching.9 For most optometric educators, clinical sessions are composed of limited time for teaching and clinical productivity. Therefore, any additional task that potentially impacts time, such as charting within EHR, warrants investigation. Documentation in either a paper chart or an electronic chart takes time for an optometric educator, but we wanted to evaluate how EHR influence this and evaluate any potential unintended consequences of EHR charting. This exploratory study was a follow-up to the previously published study “Faculty Perceptions on the Impact of Electronic Medical and Health Records in Optometric Education in the United States and Puerto Rico.”9 Information about the time impact of EHR charting in the optometric environment is scarce. A search of PubMed, Medline and VisionCite using the MeSH (Medical Subject Headings) terms electronic health record, time and documentation revealed one article pertaining to optometry.
The purpose of this survey study was to investigate the perceived impact of charting time in EHR on the academic clinical environment.
Methods
All faculty members at optometry schools in the United States and Puerto Rico who were identified in the Association of Schools and Colleges of Optometry (ASCO) faculty database as having clinical responsibilities were eligible for inclusion in this study. The survey was developed from a review of the medical literature and the investigators’ clinical experience. The survey sought information about completion of EHR charting related to timely documentation, quality and quantity of clinical teaching and clinical productivity. The survey consisted of 8 Likert response questions (2 questions about teaching, 3 questions about productivity, and 3 questions about timely documentation). Additional questions were asked about type of EHR used, number of years using, and time for teaching. Eight of the questions required a response along a six-point Likert scale (1 = never; 2 = rarely; 3 = occasionally; 4 = moderate amount; 5 = always; and 6 = not applicable).
In May 2018, a link to the survey was e-mailed to 800 optometric faculty members who met the inclusion criteria. The survey was administered via the web-based Survey Monkey system. The formatting of the survey by Survey Monkey ensured that each participant could respond only once. A comment section was included. The survey was resent to all participants two weeks after the initial deployment. Information obtained by the survey was confidential and anonymous. The survey is included in Appendix A.
The data were analyzed using IBM SPSS version 25 (Chicago, Ill.). Percent and proportion were calculated for questions 1 to 8. The comments were analyzed using a grounded theory approach. The authors identified relevant comments with emerging themes and reached a consensus on the themes.
The study proposal was reviewed by the Institutional Review Board at New England College of Optometry and given an exempt status.
Results
The survey response rate was 202/800 (25.25%). A response to each question was not mandated. The mean number of years respondents reported using EHR was 6.61 (SD = 3.45), with a range from 1 to 20 years. All respondents reported use of EHRs. Although 11 different systems were reported, Compulink (40%) and NextGen (36%) were cited most (Table 1). Responses to questions 1-8 are tabulated in Table 2. The majority of survey participants reported that chart completion during regularly scheduled clinical sessions occurred never/rarely (44%), occasionally (14%), moderately (22%) and always (19%). Forty-one percent of participants reported they always/moderately sacrificed quantity of teaching to complete charts, while 22% occasionally sacrificed quantity of teaching to complete charts.
 Table 1. |
 Table 2. |
 Table 3. |
 Table 4. |
Quality of teaching was reported to be sacrificed never/rarely (51%), occasionally (19%) or moderately/always (27%). Impact on patient care, the refusal to see a non-emergency patient, in order to complete charts, was reported as never/rarely (78%), occasionally (8%) and moderately/always (4%). Clinical productivity was reportedly sacrificed to teach and complete charts never/rarely (66%), occasionally (8%) and moderately/always (8%). Respondents reported a mean decrease in teaching hours of 1.75 (SD = 2.46, 95% CI [1.34 – 2.16]).
The results from questions 1-8 were converted to binomial data to apply chi-square analysis on the probability of a given response. The responses for each question were given either a 0 or 1. If the response was never or rarely it was given a 0. If the response was occasionally or almost always it was given a 1. Table 3 shows the response, frequency and percentage for each question as binomial data. Table 4 converts the binomial data to chi-square values and p-values to help determine if a response was significant or by chance. Table 4 shows the responses for each question were statistically significant.
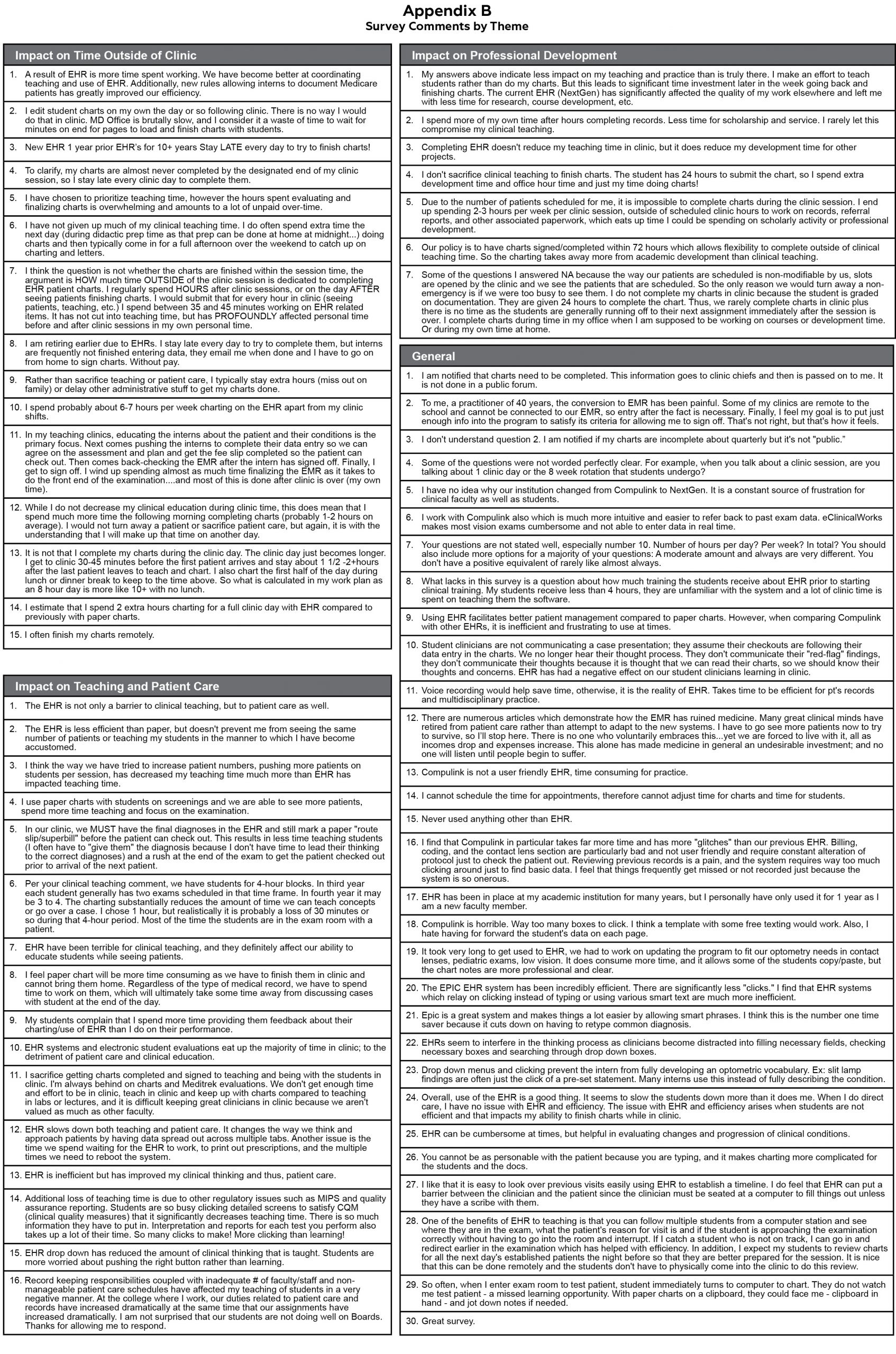
In addition to the 200 survey responses, 68 comments were received (Appendix B). Themes emerged related to the impact of EHR documentation on time outside of the clinical session, professional development and teaching/patient care. Many comments highlighted the inability to complete charts during a clinical session, necessitating staying late, working unpaid extra time, and finishing charts at home or at other times. Several comments conveyed that chart completion took time away from professional development. Many comments described the time required to complete EHR charting as challenging to teaching and patient care.
Discussion
This survey study collected information on the perceived impact of time for documentation in EHR on clinical productivity, teaching, and personal/professional time. The survey responses, statistical analyses and survey comments revealed that timely EHR documentation was a major challenge in optometric education settings. The time demands for completing patient records with EHR have been documented in health care. Research has explored the number of hours demanded of providers for every hour they are in clinic. Within the clinic day, for every hour physicians provide face-to-face care to patients, they spend nearly two additional hours on EHR and desk work.10 Outside office hours, physicians spend another 1-2 hours of personal time each night doing additional computer and other clerical work.10
Clinicians in this survey commented on a number of factors related to not completing their records in a clinic session. Factors included the speed or design/layout of EHR systems, the amount of information input required, and that both student and faculty member must review the record.
Respondents commented that they often have to finish their records at other times during their week, either at work or at home. One person stated, “To clarify, my charts are almost never completed by the designated end of my clinic session, so I stay late every clinic day to complete them.” Another reported, “I estimate that I spend two extra hours charting for a full clinic day with EHR compared to previously with paper charts.” And another noted, “I spend more of my own time after-hours completing records, less time for scholarship and service. I rarely let this compromise my clinical teaching.”
The demand for clinicians to finish their patient charts is multifactorial and contributes to the behavior of sacrificing time from other activities to complete records. One factor is the time requirement for processing billing for the visit. EHR are linked to hospital and clinic billing departments. In most clinics if a clinician does not finish his or her charts in a timely manner it could affect the insurance reimbursement. The potential for documentation mistakes is also a factor. The longer a clinician takes to finish a record, the greater the likelihood of documentation errors.11 Clinics and hospitals set time requirements for clinicians to follow so charts are documented in a timely manner, and practicing clinicians know they have to meet the requirements or be concerned about potential consequences. The survey comments revealed that other areas of faculty members’ professional and personal lives may be sacrificed in order to get charts done. One respondent wrote, “Completing EHR doesn’t reduce my teaching time in clinic, but it does reduce my development time for other projects.” Faculty who participated in the survey reported that time spent on service and scholarship are impacted because they use that time to complete their EHR from clinic sessions.
The survey also asked about time spent teaching optometric interns as it relates to the time clinicians need for charting. Responses revealed that at times clinicians choose to reduce the amount of time they spend teaching optometric interns in clinic because that time is needed to finish charts. However, respondents also provided comments indicating they do not sacrifice time for teaching and instead spend time outside of clinic hours to finish charting work. One respondent wrote, “Rather than sacrifice teaching or patient care, I typically stay extra hours or delay other administrative stuff to get my charts done.” Another wrote, “I don’t sacrifice clinical teaching to finish charts. The student has 24 hours to submit the chart, so I spend extra development time and office hour time, just doing my charts.” Optometric clinical educators should be commended on their commitment to clinical education despite the increase in time it takes to complete patient records.
In academic clinical environments, each clinical session allows a limited amount of time for teaching and clinical productivity. Clinical productivity implies sustainability for most clinics. Therefore, time devoted to clinical productivity, including providing a high level of patient care, usually must be maintained.
Survey respondents revealed in their comments that sacrifices have to be made to complete patient documentation. The time demanded by the need to complete patient charts has increased in the EHR era. Personal time, time with family, and professional development were cited by survey respondents as areas they sacrificed. Staying late, arriving to clinic early or finishing charts during other times were common themes among respondents. Respondents also commented that this extra time is an increase in hours spent working and unpaid. One respondent shared, “I think the question is not whether the charts are finished within the session time, the argument is HOW much time OUTSIDE of the clinic session is dedicated to completing EHR patient charts. I regularly spend HOURS after clinic sessions, or on the day AFTER seeing patients finishing charts. I would submit that for every hour in clinic (seeing patients, teaching, etc.) I spend between 35 and 45 minutes working on EHR related items. It has not cut into teaching time, but has PROFOUNDLY affected personal time before and after clinic sessions in my own personal time.” Another respondent noted, “I have chosen to prioritize teaching time, however the hours spent evaluating and finalizing charts is overwhelming and amounts to a lot of unpaid over-time.”
In a 2018 study, investigators explored the association between electronic health records and burnout among psychiatry residents and faculty.12 The study utilized a “burnout” survey and revealed that psychiatry residents and faculty showed signs of high emotional exhaustion, which was associated with burnout. The results demonstrated a high positive correlation between EHR use and burnout. Based on their survey results, the investigators concluded that EHR use may be an important area for program directors to monitor as they evaluate their psychiatric educators in seeking to minimize burnout and promote an environment of longevity and wellness.12 A study published in the Journal of Graduate Medical Education investigated EHR effects on work-life balance and burnout among primary care residents and faculty.13 Residents and faculty in 19 primary care programs were surveyed on work-life balance, burnout and EHR use. The exploratory study showed that more after-hours time spent on EHR was associated with burnout and less work-life satisfaction.13
The majority of clinical educators are given time for scholarship and service to promote their academic careers. Survey respondents commented that they often use that time to finish EHR charting from a previous clinical session. Sacrifices in personal and professional time may affect the sustainability, job satisfaction and longevity of clinical educators. The widespread shift to EHR use has brought benefits and costs. Access to information and statistical analysis have improved with EHR, but do those benefits outweigh the time it takes an optometric educator to document? Could the amount of time it takes to complete documentation with EHR adversely affect retention of clinical faculty members? Optometric education institutions may need to address this question as well as how EHR affect faculty satisfaction and work-life balance.
Limitations
The limitations of this study were response rate, question design, respondent bias and lack of data related to the respondents’ specific institutions. The response rate was 25.25%. This did not reflect responses from the majority of clinical educators across the optometric education field. The study explored only the perception of these 25%, which could vary from the majority. Therefore, the generalizability of the study may be impacted.
Some respondents commented that some of the questions were not clearly stated. For example, in Question 2 (My office notifies me in a public manner if my charts are not signed), the meaning of “public manner” was not provided. In Question 5 (I complete my charts with the optometry student before the end of the clinic session), the time length for a clinical session was not defined. In Question 10 (Estimate the number of hours your clinic teaching time has decreased since using EHRs in your clinical setting) the number of hours per day, week or month was not explicitly stated. Therefore, these questions relied on the interpretation of individual respondents. Another limitation of the study was that although it was anonymous, which should encourage honesty, it is possible that respondents did not want to honestly admit they are spending less time teaching or that the quality of their teaching has decreased because of EHR, representing a bias towards good teaching. This type of admittance can be held back even in an anonymous survey. To protect anonymity, data was not collected regarding the name of the institution of each respondent. Therefore, a large number of respondents may have been from one institution, introducing a potential bias.
Conclusion
An unintended consequence of EHR is increased time needed for documentation. Clinical faculty are particularly impacted because both student and faculty member need to complete and review documentation. The results of this study indicated that time spent on documentation within an EHR impacts aspects of clinical faculty members’ personal and professional lives. Uncompensated time for documentation may have an impact on recruitment, retention, professional development and career satisfaction for faculty members. Future studies are needed to quantitatively document how much additional time is needed to complete documentation within EHR in different clinical scenarios. Clinic and academic administrators may need to explore appropriate compensation for the additional time demands of EHR.
Acknowledgments
We extend gratitude and appreciation to Ashley Pierce for editing the manuscript and contributing to the formation of the tables. Special thanks to Chris Taylor, PhD, and Anthony J. Guarino, PhD, for help with the statistical analyses.
Data from this study were presented at the 2018 American Academy of Optometry Annual Meeting in San Antonio, Texas.
References
- What are electronic health records (EHRs)? [Internet]. Washington D.C.: HealthIT.Gov; [cited 2019 June 6]. Available from: https://www.healthit.gov/topic/health-it-and-health-information-exchange-basics/what-are-electronic-health-records-ehrs
- Electronic Health Records. 2016. NY: Pearson; 2016. History and Evolution of Electronic Health Records; p.1-33.
- Tierney MJ, Pageler NM, Kahana M, Pantaleoni JL, Longhurst CA. Medical education in the electronic medical record (EMR) era: benefits, challenges, and future directions. Acad Med. 2013 Jun;88(6):748-52.
- Chu G. Conversation with David Durkee, OD, July 10, 2016, as cited in Denial A, Bastian DA, Chu G, Moy A. Faculty perceptions of the impact of electronic medical and health records in optometric education in the United States and Puerto Rico. Optometric Education. Summer 2018;43(3):1-14.
- Christino MA, Matson AP, Fischer SA, Reinert SE, Digiovanni CW, Fadale PD. Paperwork versus patient care: a nationwide survey of residents’ perceptions of clinical documentation requirements and patient care. J Grad Med Educ. 2013 Dec;5(4):600-4.
- Tai-Seale M, Olson CW, Li J, et al. Electronic health record logs indicate that physicians split time evenly between patients and desktop medicine. Health Aff (Millwood). 2017 Apr 1;36(4):655-662.
- Block L, Habicht R, Wu AW, et al. In the wake of the 2003 and 2011 duty hour regulations, how do internal medicine interns spend their time? J Gen Intern Med. 2013 Aug;28(8):1042-7.
- Holmes EG, Connolly A, Putnam KT, et al. Taking care of our own: a multispecialty study of resident and program director perspectives on contributors to burnout and potential interventions. Acad Psychiatry. 2017Apr;41(2):159-166.
- Denial A, Bastian DA, Chu G, Moy A. Faculty perceptions of the impact of electronic medical and health records in optometric education in the United States and Puerto Rico. Optometric Education. Summer 2018;43(3):1-14.
- Sinsky C, Colligan L, Li L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. 2016 Dec 6;165(11):753-760.
- Thomas J. Medical records and issues in negligence. Indian J Urol. 2009 July;25(3):384-8.
- Domaney NM, Torous J, Greenberg WE. Exploring the association between electronic health record use and burnout among psychiatry residents and faculty: a pilot survey study. Acad Psychiatry. 2018 Oct;42(5):648-652.
- Robertson SL, Robinson MD, Reid A. Electronic health record effects on work-life balance and burnout within the I3 population collaborative. J Grad Med Educ. 2017 Aug; 9(4):479-484.

Appendix A. Click to enlarge

Appendix B. Click to enlarge