
PEER REVIEWED
Graduating Optometry Student Perceptions
of Their Scleral Lens Fitting Knowledge
Jennifer S. Harthan, OD, Jennifer Fogt, OD, MS, Muriel Schornack, OD, Cherie Nau, OD, Amy Nau, OD, and Ellen Shorter, OD
Abstract
Although optometric programs have incorporated scleral lens (SL) education into their curricula, student experience with SL fitting varies widely. This survey study describes the SL fitting and training experiences of optometry students graduating from U.S. schools and colleges. Participants (323) were fourth-year students preparing to graduate in 2020 (19% response rate). Students appeared to have insufficient SL fitting practice. The median number of SL evaluations completed before graduation was 5 (range 0-110), and 63% of respondents reported performing fewer than 10 fits. Students with an interest in fitting SLs may wish to pursue additional training opportunities, such as residency, to acquire more experience and achieve sufficient proficiency.
Key Words: scleral lens, education, curricula, students, contact lens
Background
Following their introduction in 1983,1 scleral lenses (SLs) were primarily utilized by providers in tertiary care centers or specialty contact lens practices to treat severe eye disease. As SLs have become more commercially available, their prescription has expanded into community eyecare practices.2 With this expansion, SL education has been incorporated into the contact lens curricula of U.S.-based schools and colleges of optometry.3 A 2019 survey of optometric educators showed that ideal SL fitting characteristics taught include central corneal clearance of 206.3 + 44 µm, 62.1 + 23.6 µm of limbal clearance, and one clock hour or less of conjunctival vascular compression at the landing zone.3 Thus, graduating students theoretically have at least cursory experience with SL evaluation prior to entering practice.
The 2019 survey of educators also revealed considerable variability in the number of SL evaluations performed by students during their optometric training. Because SL education is relatively new and many current practitioners had to learn fitting after graduation from optometry school,2 recent graduates should possess some initial advantage in their SL knowledge and experience before entering practice compared with previous generations of students. Given the limited clinical experience of new graduates, didactic SL education will guide their initial prescription and management of SLs as they enter practice. Quantifying and qualifying these students’ experience and understanding of SLs will provide guidance for ongoing development of SL education programs. In this study, fourth-year students at U.S. optometry schools and colleges were directly queried about their SL fitting experience during their training and were asked to define aspects of what they considered an ideal SL fit.
Methods
This study was reviewed and approved by the Institutional Review Board at the University of Illinois at Chicago. An electronic REDCap (Research Electronic Data Capture)4,5 24-item survey was designed by the Scleral Lenses in Current Ophthalmic Practice Evaluation (SCOPE) study team and hosted by the university. The complete survey is shown in Appendix A. A representative (American Optometric Association/American Academy of Optometry student liaison, contact lens educator, contact lens clinic chief, dean or director) from 23 of the U.S.-based schools and colleges of optometry was asked to distribute the survey link to fourth-year students at their respective institutions. The survey was active from February 15, 2020, through May 15, 2020. Two reminders were sent to representatives, but it was not verified that the survey was distributed to all fourth-year students. Surveys were completed anonymously with a chance to win a $100 gift card. Participants were not asked to identify the institution at which they received their training.
Participants were asked to identify the year in which SLs were introduced during their optometric education, and to estimate the number of SL evaluations they had personally performed during their clinical training. They were asked to describe aspects of what they considered ideal SL fitting characteristics (central corneal clearance, limbal clearance, landing zone alignment)6 along with methods they utilized to clinically evaluate SL fits (estimation of central and limbal clearance, assessment of landing zone alignment, and use of sodium fluorescein). Participants were able to type values for clearance estimations and SL diameters, which were then put into categories upon analysis. Additional aspects of SL prescription and management queried included identification of characteristics of poor lens fit that would prevent SL dispensing, and timing and components of follow-up exams. Finally, participants were asked to identify sources they planned to utilize to stay informed about new developments and best practices in SL prescription and management following graduation.
Participants were not required to respond to every question. Several items allowed participants to select multiple responses. Descriptive statistics are reported. Median scores for numerical responses are reported, with interquartile range (IQR) and range of all responses given. The IQR provides the range of the middle half of the data set rather than the spread of the whole data set.
Results
Of the estimated 1,725 potential graduating students from U.S. schools and colleges of optometry in 2020,7 323 (19%) fourth-year students completed the survey. More than half of all participants (58%, 187/323) reported SL education was introduced during their second year of optometry school. Thirty-one percent of students (101) were introduced to SLs during their third year. Two individuals reported SL education was not taught. The median (IQR) reported number of SL evaluations completed during training was 5 (13); (range 0-110; n = 323). Sixty-two percent (201) reported they had fit fewer than 10 SLs. The distribution of the number of SL fits reported by students can be found in Table 1.
Students were asked what they considered to be the ideal SL diameter. Of the 255 students who responded to this question, 237 indicated a diameter of 14 mm or larger was ideal. The median (IQR) ideal SL lens diameter was 16 (2) mm; (range 8-22) (Table 2).
Students were also asked to provide numerical responses to items related to ideal SL design and fitting characteristics (Table 3). The median (IQR) minimum acceptable central corneal clearance reported by students was 150 (100) µm; (range 0-500 µm; n = 272), and the median (IQR) maximum acceptable central clearance was 300 (150) µm; (range 0-700 µm; n = 271) (Table 2). The median (IQR) reported values for minimum and maximum acceptable limbal clearance were 50 (25) µm; (range 0-350 µm; n = 254) and 100 (125) µm; (range 0-600 µm; n = 253), respectively. Respondents indicated their willingness to accept vascular blanching or compression with SL wear, and most (71%, 190/266) reported no vascular blanching or compression should be considered acceptable. Approximately one-third of participants (20%, 52) indicated that up to one clock dial (30 degrees) of blanching or compression was acceptable, 8% (20) of students reported one quadrant (90 degrees) to be acceptable, 1.6% (4) reported two quadrants (180 degrees) to be acceptable, and no student reported three or more quadrants of blanching of conjunctival vasculature beneath the landing zone to be acceptable.
 Table 1. Click to enlarge |
 Table 2. Click to enlarge |
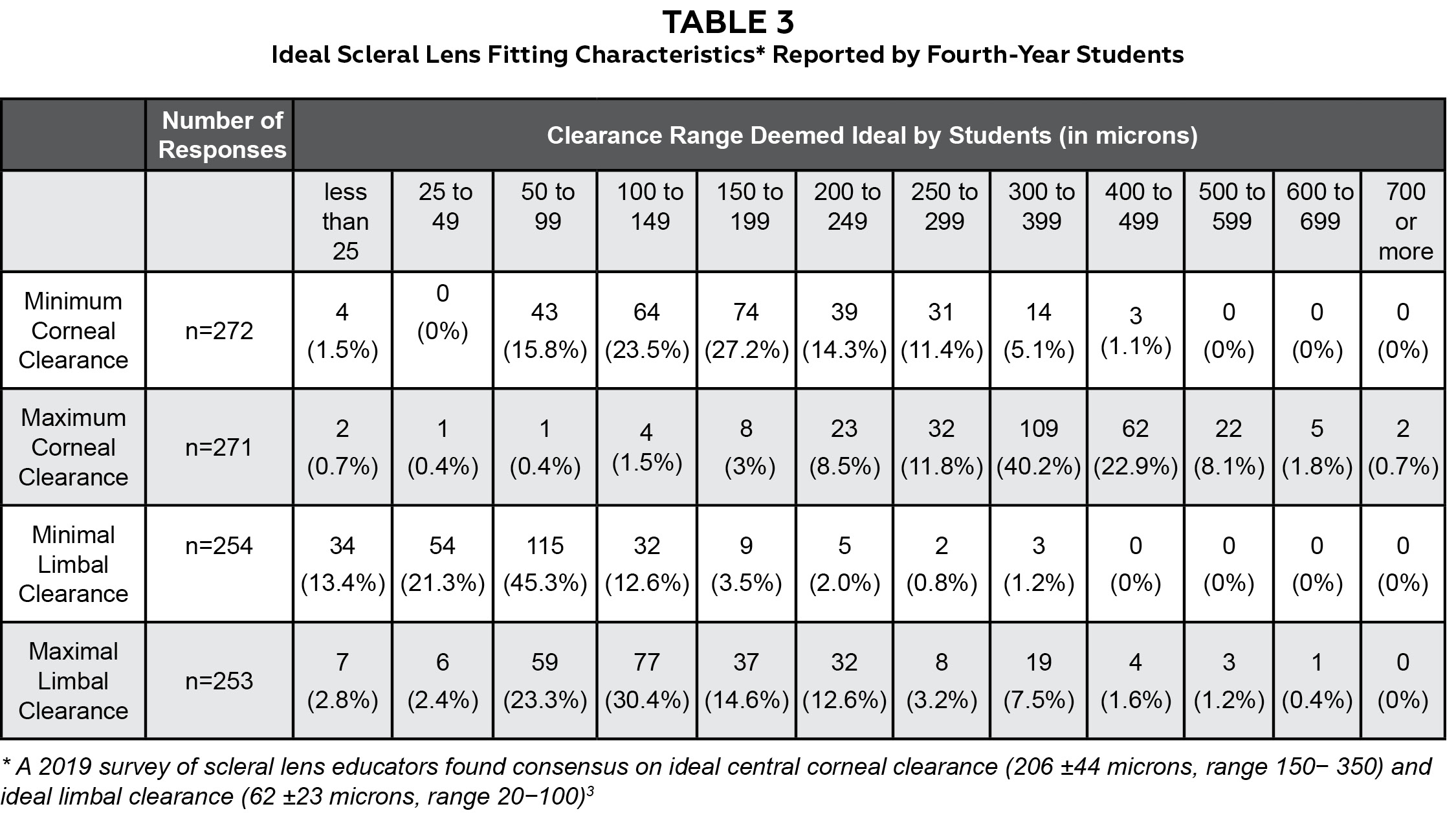 Table 3. Click to enlarge |
Most (86%, 225/263) students indicated they would plan to schedule SL follow-up visits at a specific time of day after a defined amount of wearing time. Ideal wearing time before a SL follow-up examination was reported as at least 2 to 4 hours by 59% (156) of students, 5 to 6 hours by 14% (36), 7 to 8 hours by 3% (7) and 30 to 60 minutes by 8% (20). There were 323 students who responded to questions regarding evaluation of corneal and conjunctival tissue following SL removal at a follow-up examination. Many students (70%, 227) reported evaluating for corneal staining, 61% (197) evaluated conjunctival staining, and 61% (196) looked for signs of persistent conjunctival impression following SL removal. Nine percent (30) reported routinely measuring corneal thickness following SL removal, and 2% (5) indicated they did not evaluate anterior ocular structures without the SL during follow-up evaluations. Approximately half of the students (48%, 124/261) reported that SL patients should be instructed to remove and re-apply their lenses during the day. Most participants (92%, 242/264) reported they educate their patients not to rinse their SLs with water.
There were 263 students who responded to how they intended to stay up to date on future developments with SLs following graduation. In-person and online continuing education were identified as anticipated primary sources of information (41%, 108 and 38%, 101; respectively). Only 9% (23) of participants intended to receive their SL information from industry representatives, and even fewer participants indicated they planned to personally utilize information presented in either contact lens trade journals (6%, 15) or peer-reviewed literature (6%, 17) to maintain updated knowledge regarding SLs following graduation.
Discussion
Although SLs are now included in didactic curricula for all optometric students, the amount of clinical experience with SLs that students attain during their training is highly variable and relatively limited.3 The responses of fourth-year optometric students were compared to a previously reported survey of scleral lens educators.3 More than half of the fourth-year students in this survey had completed fewer than 10 SL evaluations by the time of graduation. Some students (9%) reported no clinical exposure to SLs at all. In the 2019 survey, educators estimated students complete an average of 18 SL evaluations during training, suggesting overestimation of students’ SL clinical experience.3 Optometry students could potentially benefit from having at least 10 clinical opportunities to evaluate SLs.
Lack of clinical experience may explain deficits in students’ understanding of the basic definition of a SL. In some cases, students did not recognize essential features of scleral lens prescription and management including 7% of students who indicated the ideal SL diameter was less than 14 mm. Another potential area of improvement identified is related to clinical evaluation of patients using SLs. While educators nearly unanimously recognized the importance of removing SLs for anterior segment evaluation during follow-up examinations, only slightly more than half (61%) of students indicated they would evaluate for corneal or conjunctival staining at follow-up examinations.3 On the other hand, students appeared to be more concerned about other aspects of the SL fit compared with educators. While most students reported no scleral landing zone vascular blanching or compression was acceptable, most educators (46%) found one clock hour of blanching or compression (30 degrees) to be acceptable.3 This suggests students are relying on didactic education alone due to a lack of experience fitting SLs. Educators, who presumably have more experience fitting SLs, appear to accept that a perfect fit cannot always be achieved.3
While most students who participated in the current study received didactic education on SL prescription and management and had some clinical exposure to SLs during their clinical rotations, the responses suggest a sufficient level of clinical skill in SL management was not attained at the time of graduation. Developing both efficiency of the fitting process and proficiency in the management of conditions treated with SLs should be considered as SL curricula continue to evolve. Efficiency in the SL fitting process involves the ability to progress through initial evaluation and the fitting process with minimal delay. Although Macedo-de-Araújo et al. reported that the number of diagnostic lenses applied during initial evaluation and the total number of revised lenses ordered during the fitting process decreased significantly once a practitioner had completed 60 SL fits,8 it may not be necessary for students to see that many patients to achieve visual and physiologically successful fits. However, students who have minimal exposure to SL fitting during training might find incorporation of these devices into their practices financially and logistically challenging following graduation. Developing true proficiency in SL fitting does not necessarily directly correlate with the number of SL patients evaluated. Students who have evaluated a relatively large number of lenses on healthy eyes may be less proficient at identifying and managing issues related to SL wear than those who have evaluated a small number of lenses on more complex eyes.
Whenever possible, contact lens educators should emphasize the role of SLs in overall disease management in addition to identifying acceptable SL fitting characteristics when working with students. Concentration on the disease being treated would increase awareness of the importance of careful evaluation of the eye during SL follow-up visits. To provide more experience for students, clinical educators could consider allowing multiple students to work together on SL fitting in appropriate patients or offering additional fitting opportunities with educational workshops. Students who intend to incorporate specialty contact lens prescription into their practices may benefit from additional learning opportunities such as a contact lens residency (Accreditation Council on Optometric Education’s Cornea and Contact Lens Residencies9) or fellowship (American Academy of Optometry,10 Scleral Lens Education Society11). Referral to colleagues within the optometry community is an option for those who do not wish to engage in specialty contact lens practice. Limited experience with SLs during optometric education may lead some graduating students to avoid fitting them in private practice and may be one reason the number of SL practitioners entering this specialty each year appears to be plateauing.12
One limitation of the study may have been created by the sampling method used to recruit participants. Participation may have been impacted by the administrators’ willingness to circulate the survey to current fourth-year students, and student participation could have been impacted by the amount of emphasis placed on SLs in their respective institutions. This survey was deployed after the onset of the COVID-19 pandemic. Disruptions in clinical practice due to the pandemic potentially reduced the total number of patients (including patients wearing SLs) evaluated by students in the graduating class of 2020. Participants responding after their clinical experiences were put on hold at their institution conceivably influenced the number of SL fits evaluated and completed by the graduating class of 2020. The variability in the number of SL patients evaluated may also be explained by the type of externships completed. Students who match with schools with large specialty contact lens clinics or busy private practices perhaps gained considerably more experience in fitting and evaluating SLs compared with those who chose other externship opportunities.
Conclusion
There is considerable variability in the number of SL evaluations students are exposed to during their optometric training. While didactic training necessarily focuses on observation of aspects of the alignment between the SL and ocular surface, clinical emphasis on disease entities treated with scleral lenses along with concentration on the physiological effects of SL wear on the ocular surface may help students develop true proficiency in both SL fitting and disease management. Allowing students to work in groups or teams could provide additional opportunities to gain SL experience and to learn from each other. If students intend to incorporate SLs into their clinical practices, they may do well to avail themselves of additional educational opportunities, specifically residencies or fellowships, to further develop their SL knowledge and experience.
References
- Ezekiel D. Gas permeable haptic lenses. J Br Contact Lens Assoc. 1983 Oct;6:158-161. https://doi.org/10.1016/S0141-7037(83)80064-0.
- Nau CB, Harthan J, Shorter E, et al. Demographic characteristics and prescribing patterns of scleral lens fitters: the SCOPE Study. Eye Contact Lens. 2018 Sep;44 Suppl 1:S265-S272. doi: 10.1097/ICL.0000000000000399.
- Harthan JS, Schornack M, Nau CB, Nau AC, Fogt JS, Shorter ES. Current U.S. based optometric scleral lens curricula and fitting recommendations: SCOPE educators survey. Cont Lens Anterior Eye. 2021 Jun;44(3):101353. doi: 10.1016/j.clae.2020.07.004.
- Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009 Apr;42(2):377-81. doi: 10.1016/j.jbi.2008.08.010.
- Harris PA, Taylor R, Minor BL, et al.; REDCap Consortium. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019 Jul;95:103208. doi: 10.1016/j.jbi.2019.103208.
- Michaud L, Lipson M, Kramer E, Walker M. The official guide to scleral lens terminology. Cont Lens Anterior Eye. 2020 Dec;43(6):529-534. doi: 10.1016/j.clae.2019.09.006.
- Annual Student Data Report Academic Year 2020-2021 [Internet]. Rockville, MD: Association of Schools and Colleges of Optometry [cited 2023 March 9]. Available from: https://optometriceducation.org/wp-content/uploads/2021/05/ASCO-Student-Data-Report-2020-21.pdf.
- Macedo-de-Araújo RJ, van der Worp E, González-Méijome JM. Practitioner learning curve in fitting scleral lenses in irregular and regular corneas using a fitting trial. Biomed Res Int. 2019 Jan 28;2019:5737124. doi: 10.1155/2019/5737124.
- Accreditation Council on Optometric Education Accredited Optometric Residency Programs December 15, 2022 [Internet]. Accreditation Council on Optometric Education; [cited 2023 March 9]. Available from: https://theacoe.org/Affiliates/ACOE/Documents/ACOE/Current%20Residency%20Directory.pdf.
- Sections and Special Interest Groups [Internet]. Orlando, FL: American Academy of Optometry; [cited 2023 March 9]. Available from: https://aaopt.org/membership/sections-special-interest-groups/.
- Scleral Lens Education Society [Internet]. Scleral Lens Education Society; c2018 [cited 2023 March 9]. Available from: https://sclerallens.org/.
- Nau CB, Harthan JS, Shorter ES, et al. Trends in scleral lens fitting practices: 2020 Scleral Lenses in Current Ophthalmic Practice Evaluation survey. Eye Contact Lens. 2023 Feb 1;49(2):51-55. doi: 10.1097/ICL.0000000000000960.
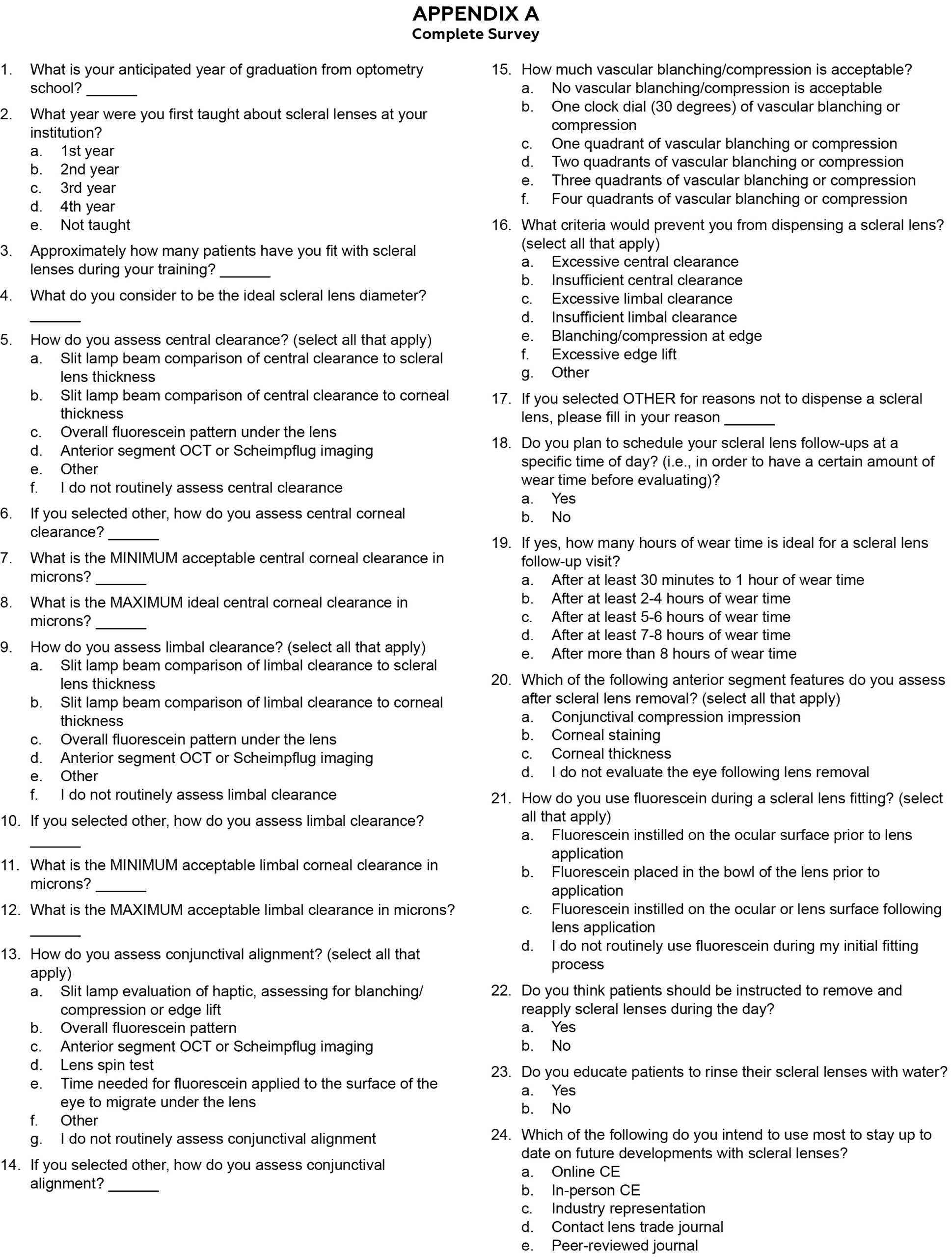
Appendix A. Click to enlarge

