Learning Environment: Students’ Perceptions Using DREEM Inventory at an Optometry Institute in Pakistan
Dr. Qamar Riaz, Dr. Shazia Sadaf, and Dr. Abdul Hameed Talpur
Abstract
Purpose: Educational environment is an important component of a curriculum and an indicator of the quality of its graduates. A number of factors are responsible for shaping the educational environment. This study was undertaken to measure the educational environment of an optometry institute in Pakistan as perceived by its students. Methods: This was a cross-sectional survey conducted at Isra School of Optometry, Karachi, Pakistan, using the Dundee Ready Educational Environment Measure (DREEM). The DREEM questionnaire was administered to all the students of the institute, maintaining anonymity. Global and domain scores for the institute and across different years were calculated using non-parametric tests. Results: For a total of 78 students (90%) who returned the completed questionnaires, the median DREEM score was 61.5% (123/200). The highest percent score was observed for “students’ perceptions of academic self” (72%) and the lowest for “students’ perceptions of teachers” (56.8%). There was significant difference in the perceptions of students in different years of education. Conclusion: Median DREEM score was more positive than negative. The study highlighted strengths of the program and areas requiring improvement. Remedial measures addressing the areas identified would improve the quality of the educational environment and thus the program.
Key Words: Dundee Ready Educational Environment Measure, educational environment, optometry, perception
Introduction
Educational environment refers to the whole range of components and activities within which learning happens. This includes faculty, teaching and learning methods, learning resources, monitoring and evaluation. Educational environment has been shown to directly affect students’ performance both at undergraduate and graduate levels.1 An educational environment that is not conducive to learning not only impedes learners’ ability to acquire new knowledge, thus hindering their growth as professionals, but also adversely affects their social life and contribution in the community.2 The availability of a learner-friendly environment becomes even more essential in disciplines that are directly related to health care and patient interaction.3 Optometry is one such profession where optometrists are trained to prescribe and fit lenses to improve vision, and to diagnose and treat common eye diseases using topical diagnostic and therapeutic drugs and non-surgical procedures.4
Optometry is an emerging discipline in Pakistan with only three institutes offering graduate programs in vision sciences or optometry. Isra School of Optometry is the only such institute in the province of Sindh. It has been functioning since 2006 and caters to students from other provinces as well. Its facility is equipped with a library, many lecture halls and tutorial rooms, a laboratory and a computer room with internet access. It offers a four-year program during which students gain competence in the theory and contemporary practice of optometry with the aim of protecting, advancing and promoting the vision and eye health of people not only in Pakistan but also in other countries. Currently, 87 students are enrolled in Isra School of Optometry: 31 in the first year, 24 in the second, 20 in third, and 12 in the final year. The higher numbers of students in the earlier years is indicative of the development of the program over the years.
As with any other program, it is crucial to periodically evaluate the educational environment of the institute as perceived by its students. This helps to identify areas with deficiencies so that measures can be taken to improve them if required. It may also provide the evidence to support continuation of current practices/methods of teaching and learning so they can be shared with other institutes that wish to replicate them. A number of studies have been done to evaluate the educational environment of medical and nursing5 colleges internationally and in Pakistan.6,7 No study that explores the educational environment of an optometry institute has been found, but some studies have suggested means for improving learning and teaching strategies in an optometry institute.
A number of instruments have been used in the literature to measure educational environments in medical and allied healthcare education, both at undergraduate and postgraduate levels. However, the Dundee Ready Educational Environment Measure (DREEM) continues to be the most widely used instrument. The DREEM questionnaire was originally developed at Dundee and released as AMEE Medical Education Guide No. 23 by Genn in 2001 and has been accepted as an international instrument for assessing the educational environment.8 It has been widely used as an instrument to collect information about the educational environment in many undergraduate health profesional institutions across countries, cultures and nationalities.9 The instrument’s validity has also been established in Pakistan.10,11
The aim of this study was to explore areas of strength and weakness in the educational environment at the Isra School of Optometry as perceived by its students using the DREEM questionnaire.
Materials and Methods
A prospective, cross-sectional, descriptive study was conducted at the Isra School of Optometry in Karachi in August 2013. The validated DREEM questionnaire12 was used to identify perceptions of students at Isra School of Optometry regarding their educational environment, i.e., areas perceived as positive and strengths of the program and areas that might require improvement, so that appropriate timely interventions could be made.

DREEM is a 50-item, self-administered, closed-ended inventory based on students’ perceptions of five areas directly related to their educational environment. These areas are: learning, teaching, academic self-perception, atmosphere, and social self-perception. Items are scored on a 5-point Likert scale as follows: 4 = strongly agree, 3 = agree, 2 = unsure, 1= disagree, and 0 = strongly disagree. However, 9 of the 50 items (number 4, 8, 9, 17, 25, 35, 39, 48 and 50) are negatively phrased statements and were scored reversely, i.e., 0 for strongly agree, 1 for agree, 2 for unsure, 3 for disagree, and 4 for strongly disagree. The instrument has a total possible score of 200, which is indicative of the ideal educational environment. The Practical Guide described by McAleer and Roff13 for interpreting the overall and subscale scores, and the number of items in each subscale is given in Table 1.
Items with a mean score greater than 3 mainly represent strong areas, while items with a mean score of less than or equal to 2 are indicative of problem areas that require immediate review and remediation. Items with a mean score between 2 and 3 reflect areas that are neither strengths nor weaknesses but could possibly be enhanced.
Data collection
Data was collected using the self-guided DREEM questionnaire administered on the last day of end-of-year exams. This time was selected to ensure maximum participation. Also, by this time every student would have spent at least a year in the institute — time sufficient to understand the educational environment and develop perceptions regarding it. Students were briefed about the aims of the study and the importance of high levels of participation during a face-to-face session in a lecture hall. The DREEM questionnaire was distributed as a hard copy to all 87 students of the institute. The students were asked to return the completed questionnaire on the same day to help ensure a high response rate. Because participation was voluntary, return of the completed forms was taken as consent to participate. Confidentiality was maintained by keeping the forms anonymous and having them collected by a researcher who was not a faculty member at the institute. Approval from the institutional ethical review committee was obtained to conduct the study. The study adhered to the tenets of the Declaration of Helsinki.14
Statistical Package for Social Sciences (SPS) version 19 was used for analyzing the data. The completed surveys were manually entered into a Microsoft Excel data sheet and exported to SPS for descriptive and inferential statistical analysis. Medians and interquartile ranges were used to express a measure of central tendency, and non-parametric analytical methods were used. Kruskal-Wallis non-parametric one-way analysis of variance and pair-wise comparisons using a non-parametric multiple comparison procedure were conducted to measure significant differences between the DREEM score and domain scores across different years of education. Significance was taken at p < 0.05.
Results
A total of 78 students returned the completed questionnaire, giving an overall response rate of 90%. This rate was 90.3% (n=28) for year 1, 83.3% (n=20) for year 2, 90% (n=18) for year 3, and 100% (n=12) for year 4 students.

Among the 78 respondents, 36 (46%) were male and 42 (54%) were female. The mean age of the students was 21.4 years (minimum 18 years and maximum 25 years).
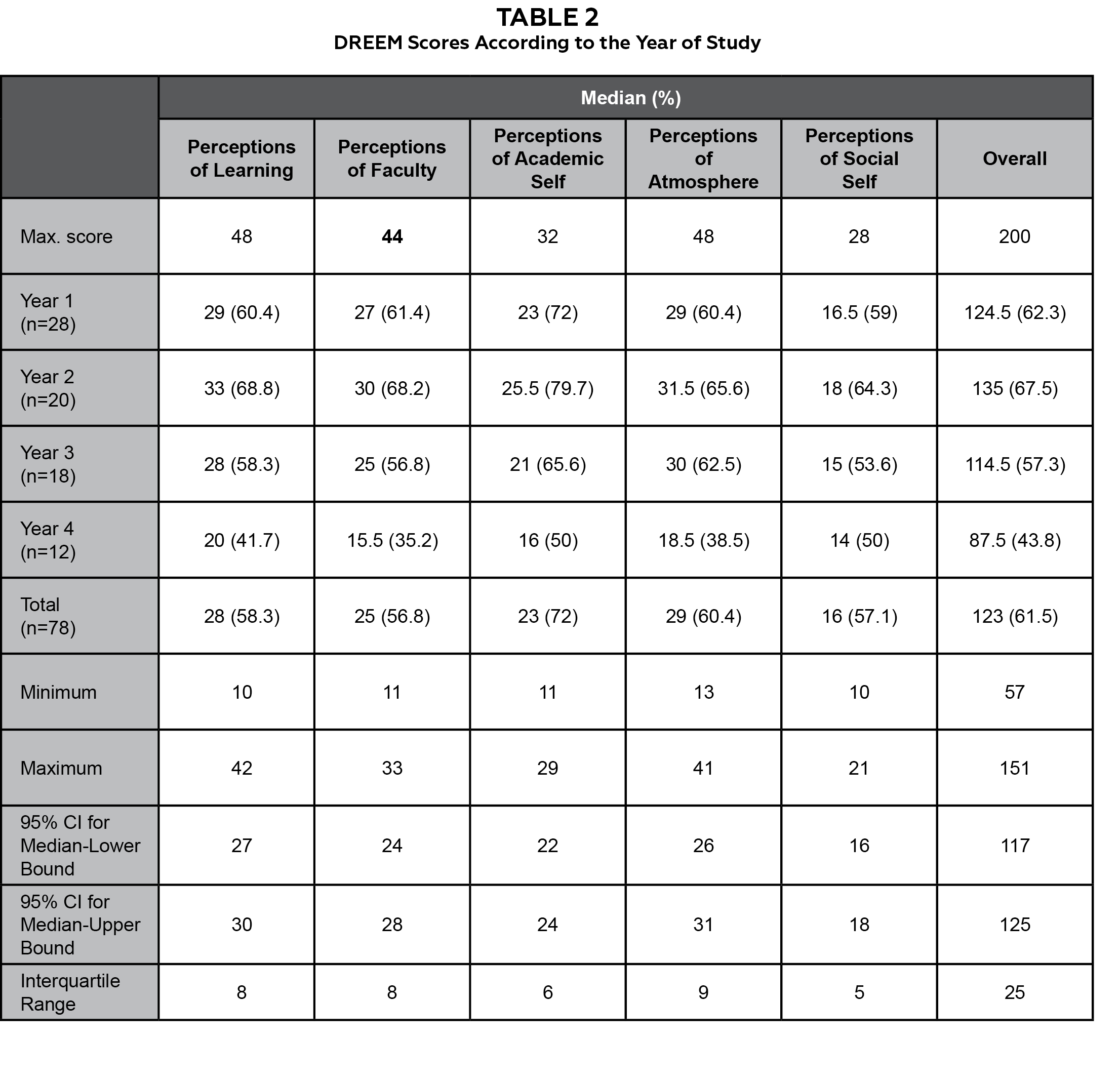
The total (median) DREEM score for all the respondents was found to be 123/200 (61.5%). The domain scores for the whole group were compared on a percentage basis because of the different maximum score of each domain. The highest percent score was observed for the “students’ perceptions of academic self” domain (72%) and the lowest for the “students’ perceptions of teachers” (56.8%). By year, the median score was highest for year 2 (135, 67.5%) and lowest for year 4 (87.5, 43.8%). The overall scores of the program and that of years 1 (124.5), 2 (135) and 3 (114.5) indicated students’ perceptions of the educational environment as “more positive than negative.” However final-year students perceived the educational environment as having “plenty of problems.”

In order to have a better understanding of the weaknesses and strengths of the educational environment at Isra School of Optometry, the median scores of the five domains and corresponding items of DREEM were also comparatively interpreted using the guide described by McAleer and Roff.13 Tables 2 and 3 show median scores for the five essential domains of the DREEM questionnaire according to the year of study.
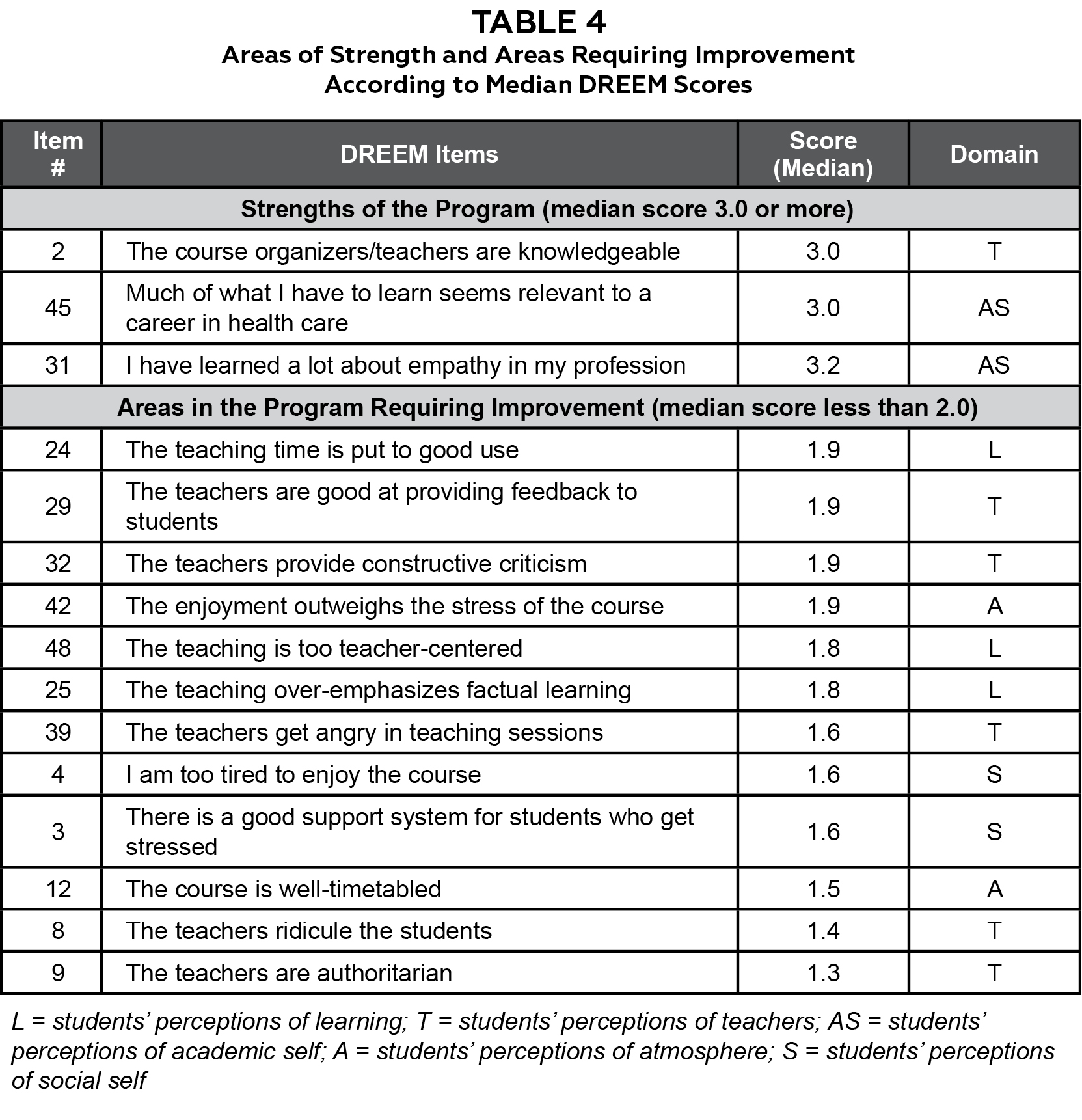
The scores for all five domains of the first 2 years were better, indicating positive perceptions regarding all domains of the DREEM questionnaire, than the final-year scores, which gave negative perceptions of the educational environment. For year 3, the perceptions scores were positive for all the domains except “students’ perceptions of social self,” which was only borderline positive, indicating room for improvement. Final-year students viewed teaching negatively (13-24) and perceived faculty to be “in need of some training” (12-22). Final-year students’ academic self-perception was “feeling more on the positive side” (17-24), and “atmosphere” according to their perceptions “needed change as there are many issues” (13-24). Final-year students’ “perception of social self” was “not too bad” (15-21). The difference in the scores in the five domains among the students in different years of study is evident in Figure 1. Some of the common areas identified as strengths or requiring improvement on the basis of the higher and lower median overall DREEM scores are presented in Table 4.
Discussion
This is the first study to report students’ perceptions of the educational environment using a validated survey regarding an undergraduate optometry program. The students’ perceptions about the educational environment at the institute were evaluated using the DREEM questionnaire. It is more focused to the environment, both classroom and clinical, experienced by students in medical and healthcare-related fields.
The overall response rate of 90% was very good for voluntary participation. This, on one hand, is a sign of students’ confidence and trust of the survey methodology. On the other hand, it might be an indication of the students’ desire to share their views about their educational environment in order to bring improvement.
The global score at Isra School of Optometry (123) using the DREEM, is similar to that reported from Nigerian medical schools.6 Although there has been no established objective consensus on an acceptable DREEM score in the medical literature, our score is better than those reported from traditional medical schools in Saudi Arabia (102/200),15 Srilanka (103/200)16 and India (107.44)17 and a nursing college in Malaysia,5 suggesting a more positive educational environment. However, much effort is needed to achieve the standards of education as set by Roff et al. for Nepalese students (130/200),6 and for students in a medical school in the United Kingdom (143/200),18 which is the highest DREEM score reported so far, indicating an environment highly conducive to learning.
When the scores of the students in different years of education were compared, it was observed that the year 1 and 2 students had more positive perceptions of the educational environment than year 4 students. This difference was also true for every domain of the DREEM inventory. Reduction in scores in the final year of training is a finding that has previously been observed in medical19 and nursing schools.20 A number of reasons have been suggested for this tendency, including higher expectations17 at the time of admission, gradual loss of interest over time, and increased stress secondary to involvement in clinical activities, often leading to depression.21 Unsatisfactory or unpleasant clinical placement experiences, attitudes of placement staff, workload, students’ perceived unpreparedness secondary to inadequate knowledge and skills expected, and lack of support in the care of patients have been factors identified as reasons for stress after involvement in clinical activities.22 All of this may cause loss of interest among students and affect their academic achievement and ultimately their patient care, often resulting in dropout from semesters or programs. Different methods have been employed by institutes to enable students to handle stress. This may include provision of psychological support, counseling and sessions/workshops on stress management.23 A formal mentorship program has also been shown to improve the academic achievement of students and decrease dropouts.24 Reviewing the academic and clinical schedule of the students to ensure balance between clinical workload, formal teaching and time for recreational/extracurricular activities can also contribute to reduction in students’ stress levels.25 Program directors need to look into the matter more closely to ensure retention of students in the program and the discipline of optometry.
Only three areas were identified as strengths of the educational environment indicated by an itemized score of 3.0 or more; one was related to the “students’ perceptions of teachers” and two were related to the “students’ perceptions of academic self” subscale. Most students perceived their teachers to be knowledgeable. They appreciated the relevance of the curriculum to the needs of the profession of optometry and the fact that they learned empathy during the course.
An item-wise analysis of different domains of perceptions identified key areas requiring evaluation and modification. Twelve out of 50 items scored less than 2.0. The majority of these items were in the “students’ perceptions of teachers” (5 items out of 12) followed by “students’ perceptions of learning” (3 items out of 12), indicating dissatisfaction with the faculty and teaching and learning at the institute. Educational environment is not limited to the physical infrastructure. Faculty play an important role in developing an environment that is conducive to learning. Some simple steps can improve the faculty-learner interactions and thus build a trustful and respectful relationship required for optimal teaching and learning at the institute. Steps may include involving the students in setting of ground rules, using interactive teaching strategies, encouraging students to ask questions without fear of being humiliated for lack of knowledge, and maintaining the content and session time balance. Sharing of information related to learning objectives and type and time of assessments well in advance and creating student-related institutional policies can also minimize the distance between the faculty and the students. Students should be provided with regular, timely and focused feedback on performance in a manner that is respectful and constructive for the learner and serves as a learning strategy rather than a cause for demotivation. Students who are having difficulties in learning need to be identified early and provided additional support. The teaching and learning strategies should follow the principles of adult learning. Using strategies that are interactive and promote critical thinking will not only reduce boredom and stress among students but is also likely to produce more competent and confident optometrists.
Students’ initial experience with clinical practice can affect their approach to clinical situations as well as their desire to excel further in the discipline. The strikingly low score for the “students’ perceptions of the faculty” by the final year highlights the need for the training of faculty as clinical preceptors in order to enable them to meet the expectations of students while maintaining their clinical workloads.26 Also, the management should ensure that the faculty are getting adequate breaks, are not overworked, and have a physical environment where they can relax and concentrate on work. This can help even faculty tempers and create a congenial environment both for the faculty and the students. The faculty should also know their role as teachers and as positive role models.27 Conducting regular course evaluations can also serve as a tool for assessment of the course and that of the faculty members.
The study also identified the group of learners (final-year students with lowest overall median and subscale scores) that require maximum support and guidance for acquiring the required knowledge and skills and gaining confidence to practice independently.
The DREEM questionnaire was helpful in providing valuable insight into how optometry students at Isra School of Optometry perceive their educational environment. It is important to have this information because students’ perceptions of their educational environment significantly impacts their behavior, academic performance and sense of well-being. The study not only identified the strengths of the program but also helped greatly in identifying limitations or the areas of the educational climate at the institute that require improvement. Attempts should be made to identify causes of dissatisfaction among the students and design appropriate remedial measures for weak areas in order to enhance the educational experience. The effect of such remedial measures would be evident in the form of improved students’ perceptions regarding their educational environment. Introducing a system of periodic but regular evaluation of the educational environment (maybe by using the DREEM questionnaire) and devising remedial strategies incorporating students’ feedback could help program managers and organizers to raise and/or maintain the quality of the educational environment. Further studies are recommended to evaluate the relationship between educational strategies and educational environment and identification of factors causing stress in clinical years and at work.
Conclusion
The median DREEM score of students at Isra School of Optometry was comparable to other medical and nursing institutes’. The study identified the strong and the weak areas of the educational environment and indicated critical need for faculty training, improving teacher-student interaction, ensuring constructive feedback to students, rescheduling of timetable by redistribution of teaching and working hours, restructuring clinical experience, and developing a support system for the students. Program managers need to take steps to improve the quality of the educational environment and thus the program by addressing the areas identified.
References
- Hutchinson L. Educational Environment. BMJ. 2003;326(7393):810-2.
- Audin K, Davy J, Barkham M. University quality of life and learning (UNIQoLL): an approach to student wellbeing, satisfaction and institutional change. J Further High Educ. 2003;27(4):365-82.
- Soemantri D, Herrera C, Riquelme A. Measuring the educational environment in health professions studies: a systematic review. Med Teach. 2010;32(12):947-52.
- Ah‐Chan JJ, Sanderson G, Vote BJ, Molteno AC. Undergraduate ophthalmology education survey of New Zealand ophthalmologists, general practitioners and optometrists. Clin Experiment Ophthalmol. 2001;29(6):416-25.
- Said NM, Rogayah J, Hafizah A. A study of learning environments in the Kulliyyah (Faculty) of Nursing, International Islamic University Malaysia. MJMS. 2009;16(4):15-24.
- Roff S, McAleer S, Ifere OS, Bhattacharya S. A global diagnostic tool for measuring educational environment: comparing Nigeria and Nepal. Med. Teach.2001;23(4):378-382.
- Khan JS, Tabasum S, Yousafzai UK, Mukhtar O. Measuring the medical education environment in undergraduate medical colleges across Punjab, Pakistan. Biomedica. 2011;27(1):14-8.
- Genn JM. AMEE Medical Education Guide No. 23 (Part 1): curriculum, environment, climate, quality and change in medical education – a unifying perspective. Med Teach. 2001;23(4),337-44.
- Basaw B, Roff S, McAleer S, Roopnarinesingh S, De Lisle J, Teelucksingh S, Gopaul S. Students’ perspectives on the educational environment, Faculty of Medical Sciences, Trinidad. Med Teach. 2003;25(5):522-6.
- Khan JS, Tabasum S, Yousafzai UK, Fatima M. DREEM ON: validation of the Dundee Ready Education Environment Measure in Paksitan. J Pak Med Asoc. 2011;61(9):885-8.
- Jawaid M, Raheel S, Ahmed F, and Aijaz H. Students’ perceptions of educational environment at public sector medical university of Pakistan. J Res Med Sci. 2013;18(5):417-21.
- Roff S, McAleer S, Harden RM, Al-Qahtani M, Ahmed AU, Deza H, Groenen G, Primparyon P. Development and validation of the Dundee Ready Education Environment Measure (DREEM). Med Teach. 1997;19(4):295-9.
- McAleer S, Roff S. Part 3: A practical guide to using the Dundee Ready Education Measure (DREEM). AMEE Medical Education Guide No.23 curriculum, environment, climate, quality and change in medical education; a unifying perspective. Edited by Genn JM. Dundee, UK: Asociation of Medical Education in Europe; 2002.
- World Medical Association. Declaration of Helsinki. Ethical principles for medical research involving human subjects. 2009.
- Al-Hazimi A, Al-Hyiani A, Roof S. Perceptions of the educational environment of the medical school in King Abdul Aziz University, Saudi Arabia. Med Teach. 2004;26(6):570-73.
- Jiffry MTM, McAleer, Fernandoo S, Marasinghe RB. Using the DREEM questionnaire to gather baseline information on an evolving medical school in Sri Lanka. Med Teach. 2005;27(4):348-52.
- Mayya S, Roff S. Students’ perceptions of educational environment: a comparison of academic achievers and under-achievers at Kasturba Medical College, India. Educ Health (Abingdon). 2004;17(3):280-91.
- Miles S, Leinster S. Medical students’ perceptions of their educational environment: expected versus actual perceptions. Med Educ. 2007;41:265-72.
- Demirören M, Palaoglu Ö, Kemahli S, Özyurda F, Ayhan HI. Perceptions of students in different phases of medical education of educational environment: Ankara university faculty of medicine. Med Educ Online. 2008;13:8.
- Hamid B, Faroukh A, Mohammadhosein B. Nursing students’ perceptions of their educational environment based on DREEM model in an Iranian university. Malays J Med Sci. 2013;20(4):56-63.
- Zawawi AH, Elzubeir M. Using DREEM to compare graduating students’ perceptions of learning environments at medical schools adopting contrasting educational strategies. Med Teach. 2012;34 Suppl 1:S25-31.
- Eick SA, Williamson GR, Heath V. A systematic review of placement-related attrition in nurse education. Int. J Nurs Stud. 2012;49(10):1299-309.
- Hyun J, Quinn B, Madon T, Lustig S. Mental health need, awarenes, and use of counseling services among international graduate students. J Am Coll Health. 2007;56(2):109-18.
- Campbell TA, Campbell DE. Faculty/student mentor program: effects on academic performance and retention. Res. in High Edu. 1997;38(6):727-42.
- Shaikh BT, Kahloon A, Kazmi M, Khalid H, Nawaz K, Khan N, Khan S. Students, stress and coping strategies: a case of Pakistani medical school. Educ Health (Abingdon). 2004;17(3):346-53.
- Burns C, Beauchesne M, Ryan-Krause P, Sawin K. Mastering the preceptor role: challenges of clinical teaching. J Pediatr Health Care. 2006; 20(3):172-83.
- Crues SR, Crues RL, Steinert Y. Role modelling – making the most of a powerful teaching strategy. BMJ. 2008;336(7646):718-21.