
PEER REVIEWED
Malagasy Health Institutions Offering Clinical Practice to Norwegian Optometry Students: A Reflexive Qualitative Study of Staff Members Experiences
Siri Nyen, MNSc, Ragnhild Arno, OD, Zo Sandra Tokiniaina, Irene Langeggen, Msc (Clin Optom)
Abstract
Significant numbers of students from universities in high-income countries travel to low-income countries to undertake clinical placement. The objective of this study is to investigate the experiences associated with hosting optometry students in eye clinics in Madagascar. We did focus group interviews with staff members and used a qualitative descriptive approach, with reflexive thematic analysis. The informants revealed challenges including language- and sociocultural barriers, lack of information about students’ goals and long-term plans. To enhance exchange programs, it is important to establish common meeting places, mandatory pre-departure language-and culture courses and establishing formalized agreements to incorporate mutual long-term goals.
Key Words: optometry students, host institutions, low-income country, international clinical placement, global education
Background
Madagascar, an island in the Indian Ocean, faces great challenges in providing proper health care for their population of approximately 30 million. Barriers to healthcare access include lack of infrastructure, lack of confidence in formal healthcare services, poor service quality, high costs, and low health literacy among the population. Frequently, the healthcare services are inadequately staffed, with outdated equipment and a lack of supplies.1,2,3,4. Eye care services are a low priority due to competing demands for health care funding.4 Madagascar has two ophthalmologists per million population, and in total two optometrists and 60 allied ophthalmic personnel for a population of 29 million.5 In contrast, Norway has 68 ophthalmologists per million population, and approximately 1,500 optometrists for a total population of five million.6
Norwegian optometry students’ clinical practice in Madagascar is contextualized against the backdrop of these healthcare challenges. The University of South-Eastern Norway (USN) is the only university in Norway offering bachelor, master, and PhD degrees in optometry. The bachelor students in Norway receive an international acknowledged degree upon graduation. The international perspective is brought to students both from external lecturers, study literature and exchange options abroad. An elective clinical course offers students a unique opportunity to travel abroad and participate in providing eye-health care services to local communities. During this experience, students are supervised by local clinical staff and are supported by interpreters who facilitate communication between the students and patients, Additionally, students benefit from the mentorship of non-governmental organization (NGO) mentors and USN supervisor. USN has since 2007 collaborated with a NGO in Madagascar, Lovasoa Cross Cultural Center (Lovasoa 4C). Since 2016, USN in collaboration with Lovasoa 4C, facilitates 12 weeks of practical clinical experience for final year Norwegian optometry students in several local health institutions. Prior to clinical practice the students conduct a language and culture course at Lovasoa 4C.
The Norwegian government views internationalization as a vital avenue for future Norwegian workers to gain indispensable skills in an increasingly global, multicultural, and digital society. In line with this perspective, the Norwegian government endorses the strategic goal of having 50% of Norwegian students to stay abroad upon graduation.7 There is an increasing number of health students from universities in high-income countries travelling to low-income countries to undertake international clinical placement. A growing number of studies found numerous positive outcomes for these students. These benefits include increased cross-cultural competence, personal and professional growth, and enhanced communication skills.8,9,10,11 However, the literature tends to overlook the perspective of host institutions. Several authors have raised concerns regarding the safety, appropriateness, and ethics of student activities abroad, particularly in medical programs during international health electives in the global south.12,13,14,15 Nonetheless, there is a noticeable gap in the existing literature as there are no studies specifically focused on the internship experiences of optometry students in the global south. The primary objective of this study is to investigate the expectations, experiences, challenges, and implications associated with hosting undergraduate optometry students from the perspective of the receiving institutions.
Methods
Study Design and Data Collection
This study has a qualitative descriptive approach using reflexive thematic analysis.16,17 We sought to get a broad analytic scope by allowing the potential for the development of innovative themes. We used focus group interviews to create data or insights that would be difficult to produce without the dynamics of the group. This article is written and follows the COnsolidated criteria for REporting Qualitative research (COREQ).18
Data Collection
Data was collected once at two main institutions receiving Norwegian optometry students for several years: an ophthalmic ward (OW) located in a mainland hospital and a general health center (GHC) supplying supplementary eye health care in an eastern coastal town.
The OW is a multidisciplinary clinic, staffed with three ophthalmologists, two refractionists, several nurses and eye health assistants. The OW engages in eye health care from out-reaches in villages to advanced surgery. Some of the staff members have professional English knowledge. The GHC lack eye-care personnel on a permanent basis. There is an optometric assistant present with limited English knowledge, who is trained through national courses and by Norwegian optometry students. This person provides simple refraction and spectacles. Staff consists of the director and two administrative personnel involved when optometry students attend GHC.
Both institutions were asked to participate in focus group interviews involving staff members who were involved, in one way or another, with Norwegian optometry students. A convenient time and place for focus group interviews was agreed in advance. Each staff member (informant) was informed orally and written (in Malagasy language) about the nature and purpose of the study. The informants were all above 18 years of age and signed informed consent.
The staff members were interviewed using semi-structured interviews. One focus group per institution was formed, one with one female and one male, another with three males only. The staff members attending the interviews had either administrative or clinical responsibilities for the students. The first interview was conducted in English by SN while ZT translated to Malagasy. SN is a Norwegian nurse who has lived 5 years in Madagascar and other African countries for several years. SN is experienced in receiving and providing administrative support for students travelling abroad. ZT is from Madagascar, has worked 10 years in Asia, and at Lovasoa 4C with Norwegian students for 5 years. The second interview was conducted by ZT in Malagasy and translated to English by ZT. Interviews (93 minutes and 53 minutes) were recorded and transcribed by ZT.
Analysis
We conducted a qualitative reflexive thematic analysis (RTA)19 of the interviews. The interpretation and coding of the interviews was carried out by SN, RA, IL and ZT. Microsoft Excel was used to manage the data. RA is a Norwegian optometrist, with experiences from clinical practice in Madagascar both as a student and twice as clinical supervisor for Norwegian optometry students. IL is an optometrist and associate professor at USN, project manager and responsible for sending optometry students abroad, since 1997. IL has lived 2 years in England and one in USA and has visited Madagascar once. All researchers possess multilingual and multicultural backgrounds and are conscious of their own assumptions while conducting RTA. Throughout the process, cultural and linguistic differences were frequently discussed.
RTA is individual native reading of the text, development of codes, subthemes, and overarching themes. We followed the process of RTAs as proposed by Braun and Clarke.19 As the first step, the researchers read and re-read the transcripts to gain familiarity with the data material. The researchers aimed to limit misinterpretation through discussions of understanding the text with ZT.
The meaning of the text, data item, was discussed and agreed upon by researchers. The code labels are the first phase in identifying segments of text, identified as interesting, relevant and meaningful.19 The code phase is the more latent step to develop candidate themes. The authors reflected between each step, to ensure that meaningful interpretation was conducted. The main themes were defined after a dynamic process of analysis. Table 1 presents the process of interpretation on how Malagasy staff members describe students’ traits and their role guiding students beyond health professional responsibilities. Informants were not a part of the analysis team.
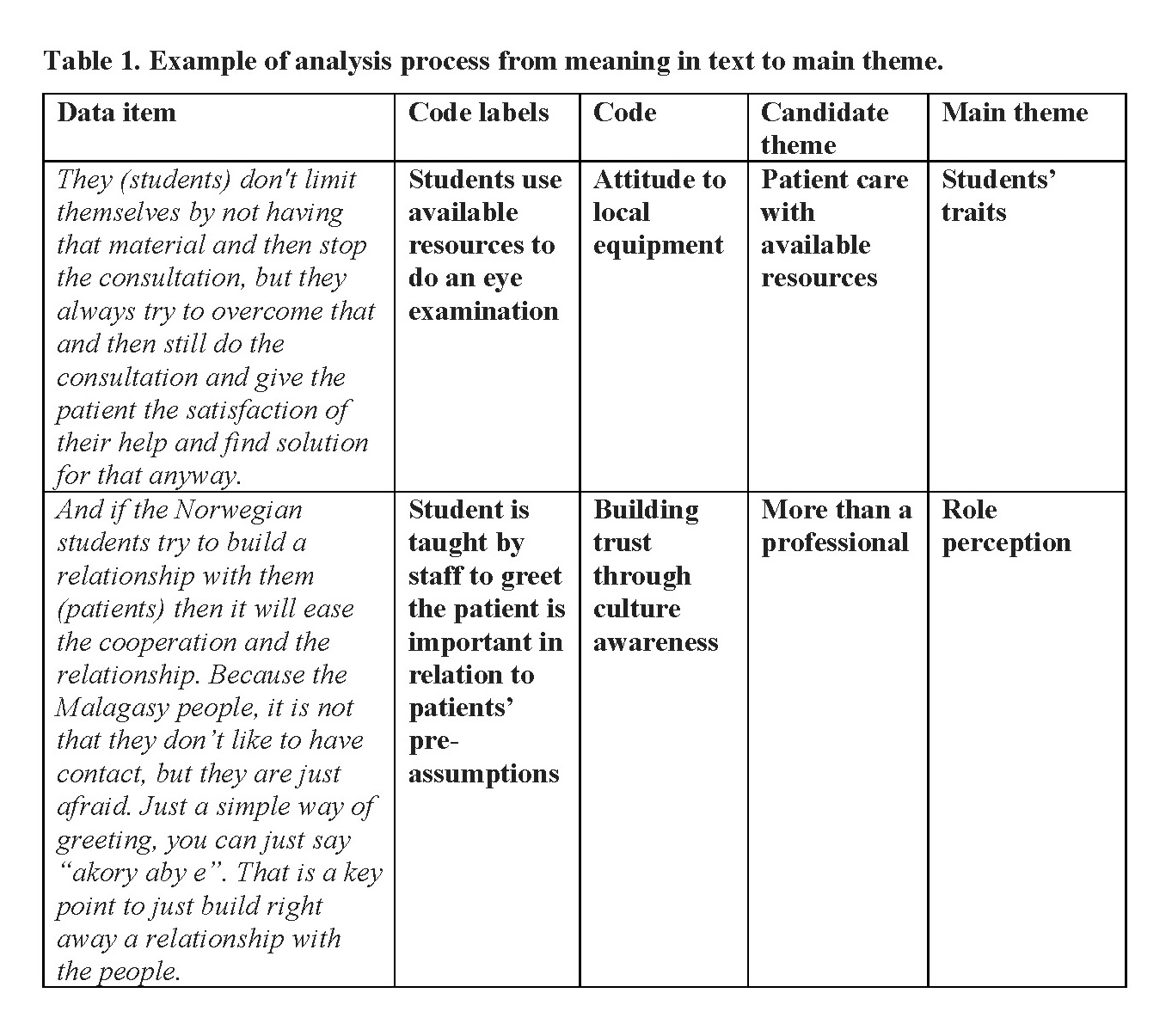
Table 1. Example of analysis process from meaning in text to main theme. Click to enlarge
Ethics
All participants were informed orally and in writing about the project’s aim. The informants were all above 18 years of age and signed the consent form. They were also informed that the information would be used to improve exchanges of students and the daily activities of the staff members as students were present. The study was approved by the Norwegian Agency for Shared Services in Education and Research, ref.nr. 592193.
Results
Three main themes (Table 2) emerged from the analysis: Role perception, Challenges and Opportunity awareness.
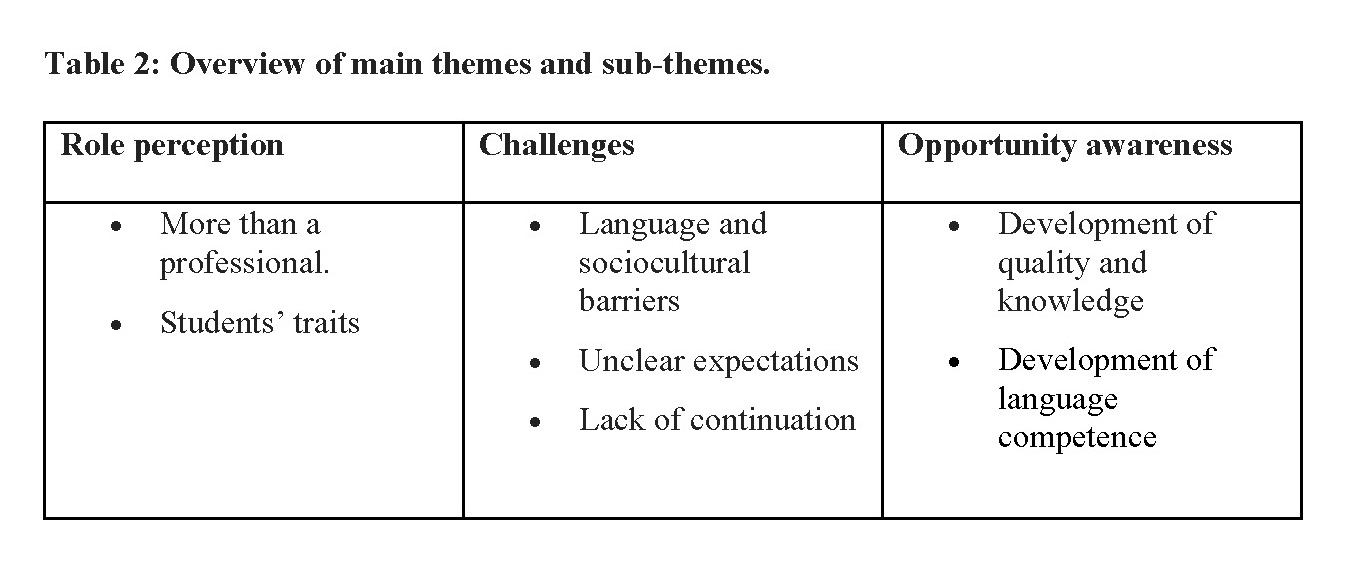
Table 2. Overview of main themes and sub-themes. Click to enlarge
Role Perception
Role perception refers to how the informants define their role. This concept includes two sub-themes: More Than a Professional and Students’ Traits.
More Than a Professional: All informants from both institutions seem to take responsibility, in various ways, for involving the students in work tasks and integrating them into the colleague group. These roles appear to have been clearly outlined among the staff before the students’ arrival. Both administrators and directors play crucial roles in introducing the students to clinic staff, facilitating their practice, and even serving as translators when needed. They stress the importance of ensuring that students receive proper introductions:
“When the students arrive here, we usually introduce them to the whole staff in order to know who those students are and where they are from. And what are they going to do here”. (i1)
Those in close contact with the students include the refractionists at OW and the trained worker at GHC. They work alongside the students daily, providing instructions on tasks within the practice place. These individuals play an important role in training the students in routines and the use of clinical instruments. Following initial guidance, they allow the students to try tasks independently, promoting a sense of autonomy.
“There are times, we give them a patient and let them treat him from the beginning, and they [the students] really start from the beginning [and do] all the steps according to theory […] We let them free to do it, but we are there next to them to assist in any case.” (i1)
The informants emphasize several times that the students should take the first initiative to greet the patients. Especially the informants from the GHC stress that an important element for establishing contact is that the students take the first step and that they greet people first.
“And if the Norwegian students try to build a relationship with them then it will ease the cooperation and the relationship. Because the Malagasy people, it is not that they don’t like to have contact, but they are just afraid. Just a simple way of greeting, you can just say “akory aby e”. That is a key point to just build right away a relationship with the people.” (i4)
Although the staff are not formally trained optometrists nor trained educators, they express mastering the field of assessing the students’ learning and performance:
“I personally can say that they know. It [optometry] is something that we do not master, but talking to them, you can hear that they know what they are doing.” (i4)
The trained worker at GHC says that he feels he can measure the students just from looking on the satisfaction of the patient:
“that if the patient were satisfied about the consultation and the result then it means that I can measure their knowledge that they master their profession.” (i5)
The informants’ narratives indicate that they all do what is in their power to help the students thrive, also to the extent outside the professional space. At the OW, they arrange morning prayer every day and students, staff and patients are invited to join. Although the sharing is in Malagasy, the students join regularly. The way the informants include the students is emerging in the following comment from the director:
“Sometimes there are some texts of the songs that are easy to translate then… for example the song number 440. Then I tried to translate the song for them. And I can see that they are happy when I do that. And as I2 said, we give them the song book and they are also trying to follow the song in Malagasy.” (i1)
Some of the informants from the OW do also take part in students’ life outside the clinic, facilitating the students stay in a new country:
“There was a time we brought them to the local market, I and X, we brought them to the Saturday market and the students were happy. They said they wanted to buy something, and they asked us. So, when they need something, they ask us without hesitation.” (i2)
The informants serve as cultural interpreters and local guides. Due to language, it appears easier for the OW staff to take part in students’ social life compared to the staff from GHC who have more problems communicating directly with the students when the translator is not there. Thus, the informants are not merely professionals’ advisors and helpers; they wear a variety of hats to make the students feel welcome and included.
Students’ Traits: Student traits refer to crucial characteristics of students, as identified by the host, that are deemed essential for a successful internship experience. The informants frequently highlight the students’ attitudes as important for the success of the internship program, often describing them as respectful, hardworking, and friendly. Despite language barriers the informants find that the students still managed to build relationships with the clients. The students attitude contributes to this:
“They are really good at welcoming the patients […]and they are good at making them feel comfortable.” (i2)
While the informants express concern about the equipment, they also note that the students effectively cope with the available resources:
“They always come and use what we have here. They don’t limit themselves by not having the material or stop the consultation. They always try to overcome that and then still do the consultation and give the patient satisfactory help and find solution for that anyway. Without the equipment.” (i4)
The informants emphasise the importance of the students’ taking initiative, showing interest and being sociable. At the OW, the students’ attendance in the morning prayer is appreciated, and shows the staff that the students want to take part and want to build relations with them as workers:
“It is even kind of natural for them. when they arrive at the same time as us and they attend the Morning devotion with us. And when we pray, they are there to listen and to observe. And sometimes when the cult is finished, they ask what the song was and then we sing it again.” (i2)
Challenges
Although the informants perceive receiving students as mainly a positive experience, their feedback in the interviews reveals some of the challenges they experienced. They highlight challenges linked mainly to language and sociocultural barriers, unclear expectations and lack of continuation.
Language and Sociocultural Barriers: The informants consider language competence to be vital for the students to fully derive benefits from the internship. They identify the language barrier as a significant challenge. Interestingly, the concern about language is predominantly associated with interactions between students and patients rather than between the informants and the students. According to the informants, students can handle simple questions and basic testing, but when it comes to patients describing their problems or the students explaining something, language barriers impede effective communication. I2 gives specific suggestions on what could help facilitating communication:
“I think they should have more vocabulary in the refraction. Some more vocabularies regarding refraction and the eyes, as the vocabularies are repeating in that field, and it will always be the same even in Malagasy.” (i2)
The informants at the CHG mention that it is a challenge that the students only learn the dialect of the city where the students do the language course. They suggest that the students should learn some words and phrases from the coastal area before they start their internship there.
The informants report that most patients have high respect towards the Norwegian students as they relate it to quality. However, the informants find that sometimes the communication barriers may cause frustration for the patients, so the staff feel they need to intervene:
‘If for example the student explains two or three times the same thing and the patient still doesn’t understand it, at that point we have to find another person to intervene and help so that the patient will not close up and then will not open up anymore.” (i4)
When asked why they think the patient ‘close-up’, one of the informants says that he believes it might be due to the low health literacy among people and the fear from the patient’s side of appearing ‘stupid’. They suggest that in addition to increasing the hours of language training before starting the students should also be more informed about context and culture, such as the issue of health literacy. The OW being a Christian clinic is also mentioned by the director to be something the students should know about without elaborating any problems related to it:
“It is good that they know it belongs to the Malagasy Lutheran church and that this should not be an obstacle from coming here.” (i1)
In addition, the informants highlight that the students should learn something about the difference in culture between the two different areas in which they do their practice:
“In the Highland, if you do not know each other you’re not forced to talk to each other. But here at the East Coast, if you see people then the students must be the first to say “akory aby”. It has an important impact to the patient, the first step that the students are doing with them. That is one of the cultural differences between the coast and the Highland.” (i5)
The use of a translator was also discussed among the informants. The professionals at the GHC appreciated that the students had a translator every day as none of their staff are fluent in English, while at the OW they saw some of the challenges of having a translator:
“I think it is not so good to have a translator. It is not necessary, and it is even more difficult to handle if there is the patient, the translator and then the student. I think that will even delay the work and that as I said it is not that necessary.” (i2)
Unclear Expectations: Although the informant narratives suggest that they feel that their role in relation to the students is clear to them, they say that they are not well informed about the students’ learning goals:
“If you are not an expert in that field it is hard to judge their level, and secondly if there were a definition in advance of the learning outcomes then it might be easier for us to measure accordingly.” (i1)
Informants from both institutions highlight the issue of insufficient or outdated equipment, which adds to the challenges arising from unclear expectations and becomes a source of concern. They express worry about whether students can effectively meet the university’s learning goals when faced with a shortage of essential equipment in their respective clinics.
“For us in our everyday work, we have some tools, but it is not sufficient. It seems the students must do some practice with low vision as optometrists, but we do not have tools for that. We don’t know if we are the ones who do not help them, or they are the ones who do not say that they should do that practice and that their practice might not be enough. For instance, there is need of this test but here we just have this [test]…. I am still wondering if that is part of the university expectation or not?” (i1)
Implicitly, the informants are suggesting a need for equipment, believing that providing it would enhance the students’ practical experience:
“So, if they could add some of those tools so that they can really exercise well with those materials. Because they can really do a lot of those practices with the patients that are coming here every day.” (i2)
In both institutions, there appears to be uncertainty surrounding the students’ time schedules. Informants at the GHC explain that there are instances when students commit to coming in the afternoon but fail to show up. They observe an increase in patient visits to the clinic when Norwegian students are present. Consequently, on the afternoon when the students did not arrive as scheduled, numerous patients were left waiting without receiving consultations from them.
The informants express that there is a lack of evaluation and feedback at the end of the students’ stay. They say that it would be useful to have some sort of evaluation to improve:
“We also want to know at the end of their stay here, how they experienced it. In general, they are always thankful, and we can see that they are happy, but we want to know more about their stay here. If there were things we could improve, what was missing?” (i2)
Lack of Continuation: The optometry students stay in Madagascar for 3 months every year, normally from January to April. Then they leave and a new group of students will arrive again next year. Accordingly, the informants find that there is a lack of continuity when the students leave:
“When the students are here, everything is fine. When they leave, then it seems that everything goes with them, and it doesn’t continue. Then when the others [the next student group] come, the thing is starting again.” (i1)
The disruption relates to the specific procedures the students do at the clinic as optometrists, and to specific equipment that the students often bring where it seems that the staff at the clinics don’t use the equipment given by the students when the students are not around:
“The solution to it is that, at least, if they want to leave something for us, then they should show to the workers here the procedure of Optometry and how to use those tools.” (i1)
The informants say that a solution would be that if the students train the workers, the workers can continue to use knowledge and equipment of optometry for their patients even when the students are not there. In addition, when a new group of students arrive, the workers can share their experience.
Opportunity Awareness
Opportunity awareness refers to the perceived possibilities that arise through the mobility program. Opportunity awareness includes two sub-themes: development of quality and knowledge sharing and development of language competence.
When asked how it has been for them to receive Norwegian students, all informants start their reply by saying something positive such as;
“For us, we do not have any problem” (i1) or “The cooperation with them has always been good “(i4).
When they elaborate on this, they focus on the opportunities that arise because of the exchange.
Development of Quality and Knowledge: Although there are narratives indicating that some of the patients, especially the children, may be a bit afraid of the foreigners, the informants say that most people link Norwegian students with quality. The informants from the GHC report that they see that when the Norwegian students are there, they do have more patients coming than normal.
“When we say there will be consultation from Norwegian students, we always receive many patients. This means that people here consider always that it will be…they expect high quality of things when it comes to Norwegian students.” (i5)
“The fact that they see the person is white, they already have this trust that the service quality is higher. Yes, the patient thinks that the quality of the service will be higher.” (i4)
The informants acknowledge and value the optometry expertise that the students bring with them, recognizing its significance for their clinics. This appreciation is expressed in various ways, with the director of the OW seeing the arrival of Norwegian students not only as an opportunity to build competence and establish meaningful relationships, but also as a means to achieve a larger goal:
“There is not much optometry in Madagascar. There is a promotion in the ministry in Madagascar. And what we have experienced till now is that it is really helping us because in our eye-clinic, there is the refraction service. And the refraction service has a big link with optometry. That’s why we say that it is good to have them to improve. And the advantage of having them is that there is an exchange and a relationship. But as a goal it would be nice to have an optometry service here after some years.” (i1)
At both institutions, the competence and quality that Norwegian students bring are recognized. Since the GHC has fewer human resources compared to the OW, establishing their own optometry service is deemed unrealistic. Nonetheless, the students contribute significantly through capacity-building activities, particularly in training clinic staff. This is considered a crucial endeavor for both clinic improvement and reputation enhancement. The trained worker emphasizes the valuable learning experience gained from the students:
“I didn’t know how to use the equipment for optometry before, only the glass. But when they arrived, they gave me a little book and then they taught me when they were here. They trained me on how to receive people and how to do with people even with the glass. And then I go deepen in that book. And I can say from the month of May until now I have received around 120 people.” (i3)
The new equipment is used by the students and enables the students to conduct a variety of activities in the clinic. However, the informants express that there is a need for more equipment.
“It could be set as a goal that in three or four years from now, being optometry student in Madagascar will not be difficult for those who are coming here. That we start slowly to have the needed equipment about it so that it is not going to be difficult for the others anymore.[..]” (i1)
Development of Language Competence: The informants see it as a value that by receiving students, they get the opportunity to improve their own language competence. That is specifically mentioned by the OW. While they say that language is a major obstacle for the students to be able to work independently, they perceive it as a possibility for themselves:
“It is also advantageous for us that they are not so good in Malagasy. Then we can also improve our English vocabulary.” (i1)
Discussion
The primary objective of this study is to investigate the expectations, experiences, challenges and implications associated with hosting undergraduate bachelor optometry students from the perspective of the receiving institutions. To our knowledge, ours is the first research to focus on host perceptions in the global south regarding receiving Nordic optometry students.
The Respectful Relationship
Our results indicate a dedicated effort by staff at both clinics to ensure the inclusion and well-being of the students. The staff willingly take on diverse roles, serving as translators, mentors, guides, professionals and intercultural interpreters, even though these responsibilities are not explicitly assigned. While other studies report how time-consuming it is to follow up on foreign students,13,20,21 the informants in our study do not report similar feelings. In addition, the informants portray the optometry students mainly in positive terms, describing them as respectful, empathic, positive and serious. This positive impression stands in contrast to other studies that have reported negative traits among students such as inflexibility, apathy in clinical care and the attitude of being ‘medical tourists’.13,22 The systematic review conducted by Lu et al.,14 encompassing the experiences of nearly 400 hosts across 25 Low-and Middle-Income Countries (LMICs) hosting mostly medical students from high-income countries (HICs), highlighted instances of power dynamics stemming from racial differences, including feelings of discrimination and disrespect among host clinicians in some studies.13,20,23 The reasons for these different findings may be manifold. The absence of negative traits reported by our informants could be in part due to the mandatory pre-departure training and weekly coaching sessions undergone by the students in our study context. Such training is recognized as effective in preventing ethical issues during internships in low-resource settings.8 The divergence could also be attributed to the perception of optometry students in our context as valuable resources rather than burdensome responsibilities.
Whatever the reason for these differences in findings, we believe that the foundation for healthy relationships between the students and local staff lies in the respectful attitude demonstrated by both parties. The informants actively involve the students in various work tasks, fostering a sense of collegial fellowship and encouraging independence with support when needed. Students are invited to join field trips and participate in social gatherings, including prayer services. In reciprocation, the students demonstrate interest in the patients, staff and local context by asking questions about language and culture, and they approach their work with seriousness. The participation of students in events like prayer services is seen by staff and patients as contributing to a sense of unity. This dynamic creates a reciprocal cycle of mutual engagement and understanding.
While the lack of language competence posed challenges in student-patient communication, it created opportunities for communication between students and staff. This is in line with previous research on host perceptions in a low-income setting with foreign midwifery students and medical electives.21,24 In our study, students search for assistance from staff when faced with language barriers and utilized occasions like morning prayers to request help with language. The observed close relationship between students and staff was particularly evident at the OW. In contrast, at the GHC, the presence of a translator was frequent, potentially acting as a barrier to developing close relationships. However, while the staff at OW viewed the language situation as advantageous for improving their English proficiency, it does not negate the need for additional language training for the students. The informants underscored that students should acquire more vocabulary, particularly related to the field of optometry, to enhance their ability to communicate effectively with patients and work more independently.
Common Meeting Places, Formal Agreements and Collaborations
While the informants express confidence in their roles regarding the students, they revealed critical gaps in regards of information flow, such as the students’ learning goals and schedules. Informants were also concerned about their institution’s equipment to support students towards their learning objectives. This is in line with other research where hosts report unclear goals and objectives for short-term medical students, emphasizing a common challenge of inadequate communication between partners involved in student mobility.14 The same review found that many host institutions struggle with inadequate mechanisms to provide feedback on visitors to sending institutions.14 In Kumwenda et al.’s study,13 informants suggested that better organization of students occurred when tutors from sending institutions established links with the host site. Establishing direct contact between the sending institution and the receiving institution appears crucial, not only relying on a facilitating partner. We propose that to enhance information flow, there should be regular meetings, preferably physical but at least online, between the responsible individuals from the host institution, the university and (in our context) the local facilitator. These meetings should occur before the students’ arrival, midway through their stay, and at the end of the program to ensure the sharing of information regarding goals, schedules, expectations and feedback. Although this approach may be time-consuming, it is likely to be more sustainable in the long run, contributing to the maintenance of motivation and proficiency among all participants.
There is a lack of empirical studies describing what hosts in low-income countries gain by receiving students. While student participants often report positive experiences, only a limited number of programs establish mechanisms that ensure sustained, ongoing benefits for the institutions involved.25 McMahon et al.21 found that receiving international medical students had a positive effect on the prestige of the host institution in the eyes of the local community which is similar to our findings. In addition, some of the informants in our study mention that they have been trained by optometry students, and the institutions have also received some equipment from them. However, there is a lack of formalized or long-term planning involved in both the training and equipment provided by the students for the clinic. The informants are explicit about the untapped potential for them to gain even more from receiving international students, indicating that certain opportunities for mutual learning and development of their institutions remain unrealized. In Lu et al.’s study,14 the informants emphasize the need for more long-term sustainable programs that include capacity building for host institutions and individuals. Ouma and Dimaras26 suggest a more equal partnership in the design phase and through relevant preparation or reciprocal support, such as staff training opportunities. A formalized agreement between the university and the host institutions would be useful to optimize the possibilities within international cooperation and student exchange.
Awareness of Underlying Attitudes
Simultaneously, we wonder why staff members did not seek more information about students’ goals or schedules, when students were present. The hesitancy of informants to request additional information may be attributed to issues of culture, lack of time or power dynamics, white privilege or ethical concerns identified in previous research within contexts with a colonial legacy.27 In addition, instances where students commit to coming in the afternoon, but fail to show up without notice, could be perceived as a manifestation of white privilege. This suggests that despite staff descriptions of students as respectful and friendly, an underlying attitude of not being accountable to anyone may exist among the students. Such behavior would be unacceptable in a Norwegian setting, where students are expected to be present at the designated practice place on time. Both sending institutions and students should be cognizant of these dynamics. Although conversations on these topics may pose challenges, it is crucial to acknowledge that factors such as skin color play significant roles in determining power and status, with being white often conferring advantages. Our study illustrates this as well through patients associating whiteness with quality. As a proactive measure, we propose the integration of discussions about power and privilege into pre-departure training for low-income countries.
Limitations
We consider it to be a strength that all authors have been involved in student exchange to Madagascar for many years and are familiar with the field and the context in which the study has been done. Recognizing potential challenges related to cultural dynamics and power imbalances, particularly concerns about informant openness during interviews, the presence of one Malagasy author, ZT, played a crucial role in establishing a trustworthy environment. This facilitated attendees to express honest feelings, experiences and future thoughts.
Despite language barriers, the careful interpretation of interview meanings is asserted through discussions and analysis presented in this article. Language barriers have been present during the process of transcription and translation, and might have influenced the findings, but when quotations have been unclear, authors have consulted ZT.
Due to the small sample size, the findings of this study cannot be generalized. However, the richness of data material obtained through these focus group interviews adds to the study’s credibility. As a result, we believe there is potential for the findings to be transferable to similar contexts. It is also a strength of the study that the analysis of the data was a long-term continuous process with thorough discussions between the authors.
Conclusion
Our study reveals the importance of clear communication between involved institutions. Conducting meetings, either in person or through available online platforms, is imperative to facilitate the exchange of information regarding goals, schedules, expectations and evaluation. One of our recommendations is the implementation of a predeparture compulsory in depth language- and culture course for outbound students. This course should encompass specific terms related to their field of practice, customized to the local context, and include elements of cross-cultural communication and perspectives on power imbalances. We underscore the value of reciprocity and recommend establishing formalized agreements to incorporate mutual long-term goals. For future research, we recommend exploring further the experience of host institutions receiving international health care students.
Acknowledgements
The authors would like to thank the Norwegian Directorate for Higher Education and Skills (HK Dir), for funding the project: ‘Clinical practice in Madagascar – international perspective on quality of student life and eye health services.’ This study is a part of the project.
References
- Favero R, Dentinger CM, Rakotovao JP, et al. Experiences and perceptions of care-seeking for febrile illness among caregivers, pregnant women, and health providers in eight districts of Madagascar. Malar J. 2022 Jul 7;21(1), 212. doi: 10.1186/s12936-022-04190-x
- Harimbola DR, Mizumoto K. Individual and Household Risk Factors for Severe Acute Malnutrition among Under-Five Children in the Analamanga Region, Madagascar. Int J MCH AIDS. 2018;7(1), 217–225. doi: 10.21106/ijma.248
- Marks F, Rabehanta N, Baker S, et al. A Way Forward for Healthcare in Madagascar? Clin Infect Dis. 2016 Mar 15;62 Suppl 1, S76-79. doi: 10.1093/cid/civ758
- Randrianaivo JB, Anholt RM, Tendrisoa DL, Margiano NJ, Courtright P, Lewallen S. Blindness and Cataract Surgical Services in Atsinanana Region, Madagascar. Middle East Afr J Ophthalmol. 2014 Apr-Jun;21(2), 153–157. doi: 10.4103/0974-9233.129767
- Country Map and estimates of vision loss – Madagascar [Internet]. London: The international Agency for the Prevention of Blindness [cited 2025 January 5]. Available from: https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/countries/madagascar/
- Country Map and estimates of vision loss – Norway [Internet]. London: The international Agency for the Prevention of Blindness [cited 2025 January 5]. Available from:https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/countries/norway/
- St. 7 (2020–2021). (2020). En verden av muligheter—Internasjonal studentmobilitet i høyere utdanning. Kunnskapsdepartementet. https://www.regjeringen.no/no/dokumenter/meld.-st.-7-20202021/id2779627/
- Greaker TK, Grudt SK, Aune I. Norwegian nursing students’ experience during clinical placement in an African country: Communication, relationship building and nursing identity. A qualitative study. Nurs Open. 2023 Mar;10(3), 1803–1810. doi: 10.1002/nop2.1440
- Hovland OJ, Johannessen B. Sykepleierstudenter utvikler kulturell kompetanse på utveksling i Tanzania. Sykepleien Forskning. 2018;73782, e-73782. doi: 10.4220/Sykepleienf.2018.73782
- Jeffrey J, Dumont RA, Kim GY, Kuo, T. Effects of international health electives on medical student learning and career choice: Results of a systematic literature review. Fam Med. 2011 Jan;43(1), 21–28.
- Ulvund I, Dadi GB, Sundal H. (). Nurses benefit from international clinical placement as nurse students: A qualitative study. Nurse Educ Today. 2023 Feb;121, 105663. doi: 10.1016/j.nedt.2022.105663
- Kolars JC, Cahill K, Donkor P, et al. Perspective: Partnering for medical education in Sub-Saharan Africa: seeking the evidence for effective collaborations. Acad Med. 2012 Feb;87(2), 216–220. doi: 10.1097/ACM.0b013e31823ede39
- Kumwenda B, Dowell J, Daniels K, Merrylees N. Medical electives in sub-Saharan Africa: A host perspective. Med Educ. 2015 Jun;49(6), 623–633. doi: 10.1111/medu.12727
- Lu PM, Mansour R, Qiu MK, Biraro IA, Rabin TL. Low- and Middle-Income Country Host Perceptions of Short-Term Experiences in Global Health: A Systematic Review. Acad Med. 2021 Mar 1;96(3), 460. doi: 10.1097/ACM.0000000000003867
- McCarthy AE, Petrosoniak A, Varpio L. The complex relationships involved in global health: A qualitative description. BMC Med Educ. 2013 Oct;13, 136. doi: 10.1186/1472-6920-13-136
- Braun V. Thematic Analysis: a practical guide. London: SAGE; 2022.
- Byrne D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Quality & Quantity. 2022;56(3), 1391–1412. doi: 10.1007/s11135-021-01182-y
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007 Dec;19(6), 349–357. doi: 10.1093/intqhc/mzm042
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006 Jan;3(2), 77–101. doi: 10.1191/1478088706qp063oa
- Keating EM, Haq H, Rees CA, et al. Reciprocity? International Preceptors’ Perceptions of Global Health Elective Learners at African Sites. Ann Glob Health. 2019 Mar 15;85(1), 37. doi: 10.5334/aogh.2342
- McMahon D, Shrestha R, Karmacharya B, Shrestha S, Koju R. The international medical elective in Nepal: Perspectives from local patients, host physicians and visiting students. Int J Med Educ. 2019 Nov 22;10, 216–222. doi: 10.5116/ijme.5dc3.1e92
- Rees C, Keating E, Lukolyo H, et al. Host clinical preceptors’ perceptions of professionalism among learners completing global health electives. Int J Med Educ. 2018 Jul 27;9, 206–212. doi: 10.5116/ijme.5b40.6e4b
- Lukolyo H, Rees CA, Keating EM, et al. Perceptions and Expectations of Host Country Preceptors of Short-Term Learners at Four Clinical Sites in Sub-Saharan Africa. Acad Pediatr. 2016 May-Jun;16(4), 387–393. doi: 10.1016/j.acap.2015.11.002
- Bull MA, Geraghty DS, Dube MM, et al. Facilitating midwifery students on an international placement: Clinical facilitator perspectives. Nurse Educ Pract. 2020 Oct;48, 102869. doi: 10.1016/j.nepr.2020.102869
- Hegwood M. A Critical Reflection on the Role of Power and Privilege in Conducting International Development Research. Purdue J Serv Learn Int Engagement. 2020 Jan;7(1). doi: 10.5703/1288284317234
- Ouma BD, Dimaras H. Views from the global south: Exploring how student volunteers from the global north can achieve sustainable impact in global health. Global Health. 2013 Jul 26;9(1), 32. doi: 10.1186/1744-8603-9-32
- Renaud-Roy E, Bernier N, Fournier P. Host perspective on academic supervision, health care provision and institutional partnership during short-term electives in global health. Med Educ. 2020 Apr;54(4), 303–311. doi: 10.1111/medu.14027
- Kim J, Olaiya MT, De Silva DA, et al. Global stroke statistics 2023: Availability of reperfusion services around the world. Int J 2024;17474930231210448. doi: 10.1177/17474930231210448

