
PEER REVIEWED
The State of Optometric Education in India,1958-2022
Anitha Arvind, BS(Opt), MOptom, PhD, FBDO(o/s), FIACLE, FBCLA, Kovin Shunmugam Naidoo, PhD, Peter C. Clarke-Farr, PhD
Abstract
Optometrists with varying levels of optometric education provide eyecare services to the public in India. This study aimed to review and compare the curricula in diploma (2-year program) and degree (4-year program) colleges in India with the curricular support elements developed by the World Council of Optometry (WCO). Optometry curricula from 32 colleges were reviewed. Of the 20 degree colleges included in the study, 83% (n = 17) included all the enabling science subjects listed by the WCO while 34% (n = 4) of the diploma colleges included these subjects. The majority (n = 19, 93%) of the degree colleges included all the core optometry subjects in their curricula compared with 57% (n = 7) of the diploma colleges in the study. This study highlighted the need for harmonization of optometric education for a uniform national competency-based curriculum as well as the establishment of an accreditation body to ensure consistency in optometric education in India.
Keywords
Background
Blindness and vision impairment are two of the most significant public health issues in India, which is home to 20.5% of all cases of blindness in the world, 22.2% of the world’s low vision population and 21.9% of individuals with vision impairment.1 Cataract is the leading cause of avoidable blindness in India, followed by uncorrected refractive errors.1,2,3 Cataract accounts for 66% of all avoidable or preventable blindness while uncorrected refractive errors (30%) are the major cause of vision impairment.4 In India, which has a population of more than 1 billion, there is a huge burden on ophthalmologists to tackle eyecare issues, especially the escalating prevalence of avoidable blindness and vision impairment.1,2,3 The ophthalmologist-to-population ratio is 1:25,000 in urban areas and 1:219,000 in rural areas, which underscores a substantial workforce imbalance between the two settings.5-9 One needs to undergo 8 years of training to become an ophthalmologist in India. On their own, ophthalmologists, who are expensive to train and few in number, cannot fulfill the country’s current unmet eyecare needs.
Medical professions such as ophthalmology and other branches of medicine are regulated and accredited by the Indian Medical Association. Although the practice of optometry is recognized as an allied health profession by the Ministry of Health and Family Welfare, it is yet to be regulated. In India there is no regulatory body governing either the dispensing of optical appliances or optometry eye care, and this has led to various levels of certificate and diploma programs.
With respect to optometry and spectacle provision, published data show that India has 9,000 optometrists who have undergone a minimum training of 4 years and 40,000 optometrists who have undergone a training of 2 years.10 It is estimated that 115,000 4-year trained optometrists would be required to give far-reaching eye care to individuals in the country.11 India has a dearth of optometrists because of scarcity not only in number but also in terms of education and training. This shortage is due to the scarcity of schools that provide 4-year education programs in optometry according to globally accepted standards. Most eyecare needs in India are instead addressed by eyecare personnel who undergo a 2-year training program.12 Currently, holders of optometry diplomas (2-year) and optometry degrees (4-year) are employed and offering services to the public at the primary and secondary eyecare levels with no differentiation with respect to salary or roles and responsibilities.
Development of optometry in India
Optometry was born in India approximately 65 years ago and has grown ever since. It was recognized as a profession in India to lessen the burden of refraction on ophthalmologists and address the vision care needs of a growing population by the National Program for Control of Blindness and Visual Impairment (NPCB&VI) set up by the Indian government.13 Under NPCB&VI, the government of India established its first school of optometry (2-year program) in 1958 at the Gandhi Eye Hospital in Aligarh.13 The 2-year trained optometrists were recognized by NPCB&VI and employed as Mid-Level Ophthalmic Personnel (MLOP) or Para Medical Ophthalmic Assistants (PMOAs) in the eye hospitals run by state and central government. Before the establishment of the first school of optometry, opticians who learned the trade as apprentices carried out the bulk of optical work and sight testing. There were only a few formally trained opticians from abroad.14 By 1969, seven schools of optometry were established offering a 2-year program of instruction leading to a Diploma in Refraction and Optometry (DROpt) or a certificate of completion.14 Refraction plays a limited role in eye examinations, and many ocular conditions can go unnoticed in a test that measures only refractive status; therefore, the need for a comprehensive optometry school arose. The first undergraduate 4-year degree program was established in 1985. Since then, several schools and colleges of optometry have been established that offer optometric education at the undergraduate, postgraduate and doctoral levels. A report by the India Vision Institute (IVI) suggested that as of July 2015, 164 institutions were providing optometry as a primary eyecare program in India.15 According to the Indian Optometry Federation, an optometrist is someone receiving formal optometry training for a duration of 2 years or more.6 This definition was adopted for this study.
Despite significant progress in establishing schools of optometry across the country, optometry in India has yet to define a governing body to regulate the profession, which has resulted in optometrists with varying levels of skill and competency offering services. Due to the unregulated environment, the training levels and scope of optometric practice in India have been divided in the past. In recent years, tremendous progress has been made toward establishment of a unified, standardized, regulated profession to meet the eyecare needs of the population at large.10
2-year diploma optometrists
A 1969 optometric services survey in Delhi, India, showed there were three types of practices related to the education level of the practitioner.14 The first type comprised foreign-trained optometrists who successfully managed all the optometric needs (primary eye care) of their patients. The second type comprised holders of 2-year DROpt qualification. This type knew the significance of the tests they performed, were aware of the complexities of the visual system, and showed more concern for patients’ visual welfare, though they were not managing all their of their patients’ optometric needs. The third type were opticians who learned the trade as apprentices and were offering merchandise and sales services more so than visual welfare services.14 Ocular conditions and ocular manifestations of systemic conditions went undetected when services were rendered solely toward refraction and spectacle dispensing. This was a concern for ophthalmologists who maintained that optometrists and opticians should be under ophthalmological supervision to ensure proper patient management.
4-year degree optometrists
The drawbacks of the 2-year diploma program led to the development of the 4-year degree program. In 1985, the Sankara Nethralaya Eye Hospital in Chennai established the Elite School of Optometry (ESO), the first to offer a 4-year baccalaureate in optometry. In 1994, ESO became an affiliate of the Birla Institute of Technology and Science (Pilani) and began offering Bachelor of Science (BS) and Master of Philosophy (MPhil) programs and, later, a doctoral program (PhD).16 Following the Birla/ESO affiliation, the Bausch + Lomb School of Optometry was established in Hyderabad and other institutions began offering a 4-year degree program.16 Since then, 124 schools of optometry offering a 4-year degree program have been established.15 The University Grants Commission (UGC) is India’s statutory body responsible for maintaining standards in higher education, and it has recognized optometry as a course that could be offered at the undergraduate, postgraduate and doctoral levels in the university setting.17 State governments in the recent past have recognized the 4-year degree program in optometry and give institutional recognition to the optometry course. However, not all states have adopted this.
The degree programs are 4 years and include 1 year of internship at an eye hospital. The curriculum implemented across the degree colleges has been adapted from the Common Minimum Optometry Curriculum (CMOC) suggested by the Association of Schools and Colleges of Optometry India (ASCO-India) (Table 1). At the undergraduate level in the first year, the curriculum covers the basic sciences and other subjects such as communication and computers. In the second year, ocular-related sciences, optics and some practical subjects are undertaken. The third-year curriculum is dedicated to core optometry and specialty subjects such as contact lenses, binocular vision, low vision care, pediatric and geriatric optometry, public health, research methodology and clinical exposure, as well as preparing students for internship when they are in the fourth year.
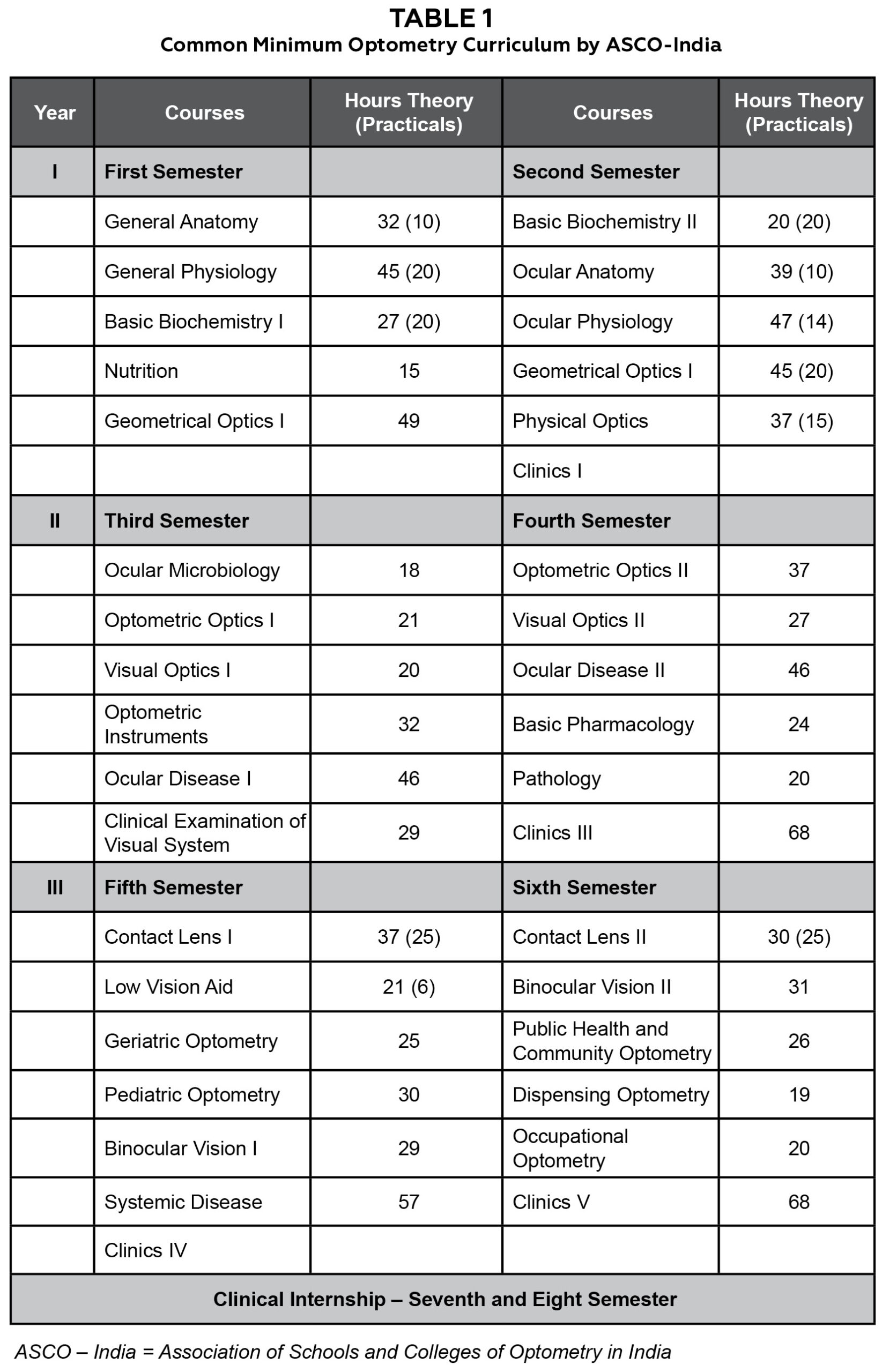
Table 1. Click to enlarge
World Council of Optometry curricular elements
In 2013, the World Council of Optometry (WCO) adopted a document on curricular components for an optometry program ― “Curricular Support Elements for an Optometry Program” ― for schools and colleges planning to begin or overhaul an optometry program.18 The document considers 15 elements from an exhaustive eye assessment and builds up the education program content from the information and aptitudes that support every component. The WCO identified eight enabling science subjects and 15 core optometry subjects that should be incorporated into the curriculum to prepare an optometrist to provide comprehensive eyecare service.
Among the 15 curricular elements recognized by the WCO, 10 elements are parts of a comprehensive eye examination, one element relates to patients’ well-being, three elements are specific to assessment and care of pediatric, low vision and geriatric patients, and one element is linked with patient care involving continuous professional development and practice-based learning.
No empirical broad-based research has been conducted to evaluate the current state of optometric education in India. Therefore, this study aimed to review and compare the existing curricula in diploma (2-year program) and degree (4-year program) colleges in India with the curricular support elements developed by the WCO.
Methods
A document survey study, which involved schools and colleges offering diplomas and degrees in optometry, was used for this research. A list of schools and colleges of optometry in each zone of India was compiled based on information obtained by ASCO-India and IVI.15 Due to the variable distribution of schools of optometry across India, a stratified random sampling technique was employed. The cohort of schools and colleges was further stratified based on whether the duration of optometric education was a minimum of 2 years or above. Based on the formula for sample size calculations of finite population correction for proportions, 32 colleges were included in the study.
Due to up-gradation of diploma colleges to degree level and the closure of many diploma colleges in the country, the sample size between the degree and diploma colleges is uneven. Keeping the total sample size to 32, 20 degree (4-year) colleges and 12 diploma (2-year) colleges were included in the study.
Institutes offering fewer than 2 years of formal education in optometry and colleges offering undergraduate programs that are not recognized by the UGC or provide education through the distance learning mode were excluded from the study
Curricular analysis
The curriculum followed in each school and college of optometry in each zone was studied in detail and collated. The curricula were obtained from the institute heads along with their written consent for the purpose of the study. The information provided was checked against the information provided at the institute websites. The information from each institution included the duration of the optometry program, the subjects offered in each year, the credits/hours of study for each subject, practical hours allotted, the pattern of examination, clinical training provided, laboratory facilities and the number of faculty teaching basic sciences and core optometry subjects. The information obtained was further used to identify the gaps existing across diploma and degree colleges. The existing optometry curriculum at the diploma and undergraduate level was then compared with the WCO document on curricular components for an optometry program.18
This research study was approved by the Humanities and Social Sciences Research Ethics Committee of the University of KwaZulu-Natal (June 26, 2018, No: HSS/1635/017D).
Results
The study results showed that 12 diploma colleges (37%) and 20 degree colleges (63%) offered optometry at the undergraduate level. The majority of colleges that offered optometry at the undergraduate level were affiliated with state government universities (55%). The rest were either private universities (30%), deemed-to-be universities (10%) or autonomous institutes (5%). The affiliations of diploma colleges were variable in different states under study. Most of the colleges (six diploma colleges) were under the State Paramedical Council (50%). The nomenclature for the degree and diploma courses included in the study varied across the country as shown in Table 2.
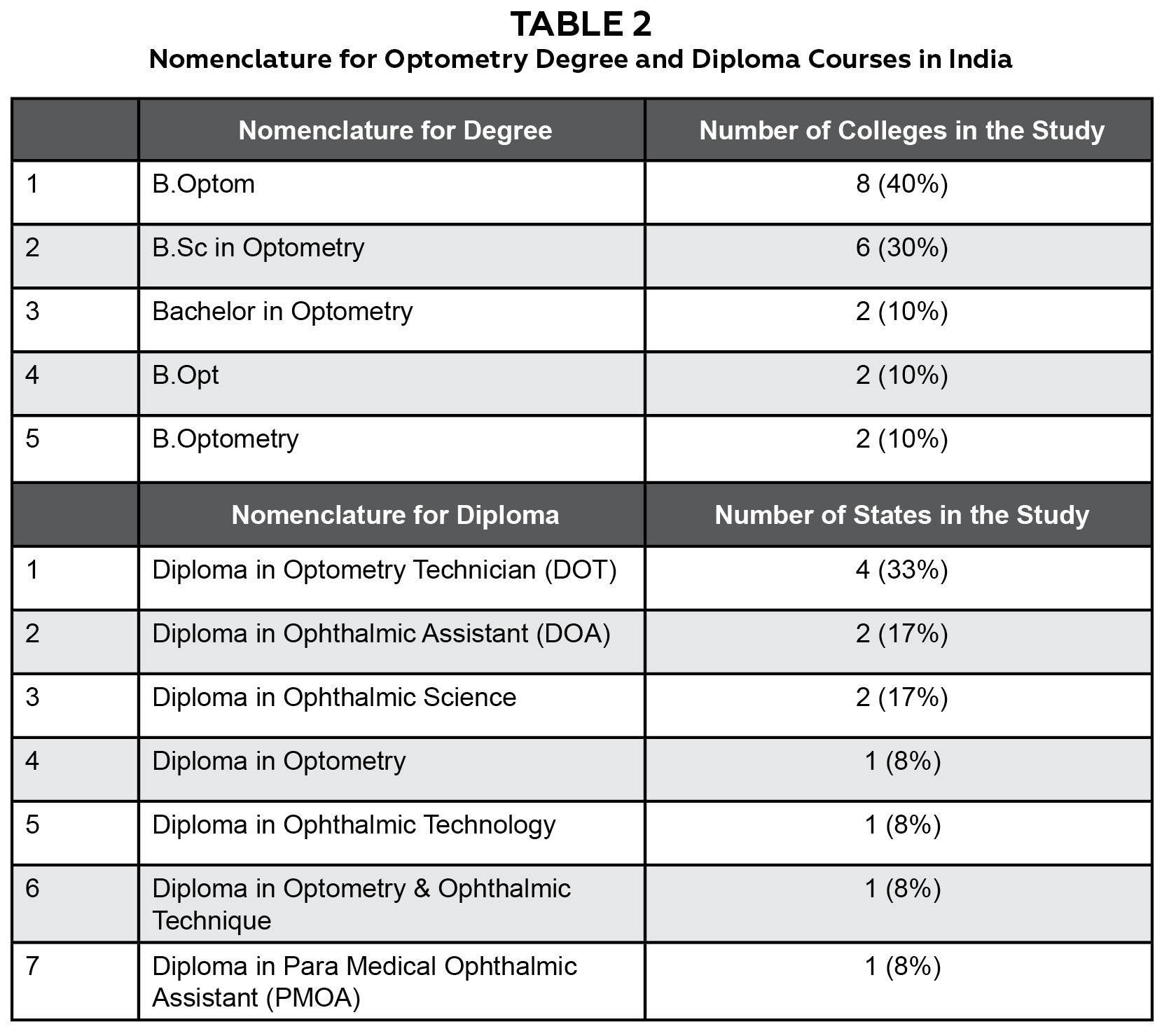
Table 2. Click to enlarge
Academic calendar and examination pattern
The academic calendar (final assessment) pattern was either semester (12 colleges) or annual (eight colleges) for degree colleges, but all the diploma colleges adhered to the annual examination pattern. A semester included 18 weeks, while the annual term included 36 weeks. The diploma and degree colleges in the study employed a traditional system (pen and paper examination along with practical and viva voce) of assessing and grading students during the program. This assessment and grading were done on the basis of theory and practical examinations in line with the dictates of the affiliating university or institute.
Student intake
The student intake in degree colleges was variable, ranging between 10 and 60, with an average of 29 ± 11 students. The intake for diploma institutes varied among the schools and colleges and also between government and non-government (private) institutes and ranged between 5 and 60 students per year.
Criteria for admission
The eligibility criteria for both diploma and degree students were the same, that is, 10 + 2 years of high school education within the science stream (physics, chemistry and math/biology). The minimum high school grade (in percentage) requirement (towards diploma/degree admissions) for school subjects was variable among diploma and degree colleges in the study, ranging from 40% to 60%. Selection of students into the diploma or degree program was based on either a written assessment followed by viva voce set by the individual institutes or affiliating university or based directly on high school marks.
Lecturing staff
The lecturing staff in the colleges offering a degree in optometry comprised medical faculty (non-ophthalmology), ophthalmologists, optometry teaching faculty and non-medical faculty. Postgraduates in optometry were employed as clinical instructors and teaching faculty in the degree (4-year) colleges. Most of the staff members lecturing at the diploma institutes were ophthalmologists and medical teaching faculty, and few optometrists were available to teach refraction and diagnostic procedures. The fourth year of the degree programs was solely dedicated to internship wherein students were involved in patient care in hospital and optical settings under supervision, while the 2-year diploma programs did not have a defined internship period in the curricula.
Curriculum for degree and diploma colleges
The study found that the curricula for diploma and degree colleges comprised subjects under basic or enabling sciences as well as core optometry subjects. Basic or enabling sciences were subjects that supported learning core optometry subjects. The diploma programs comprised a 2-year course and the curricula were ophthalmology-based, with emphasis on key clinical areas such as ophthalmic surgical instruments, outpatient procedures, patient care, minor surgical procedures, operation theater procedures, preoperative and postoperative care, eye banking, community ophthalmology and refraction. The diploma programs were oriented more toward ophthalmology, preparing students for practice under the supervision of ophthalmologists, whereas the undergraduate programs were structured to prepare students for independent practice within the scope of optometry.
The basic/enabling science subjects such as General Anatomy, Cell Biology and Biochemistry, Physiology and Microbiology were included in all the degree colleges (20) included in the study. None (0%) of the diploma colleges included Psychology, Mathematics and Applied Statistics and Research Methodology in their curriculum. While 35% of the degree colleges included Mathematics in their curriculum, diploma colleges did not offer the subject (0%) as shown in Figure 1.
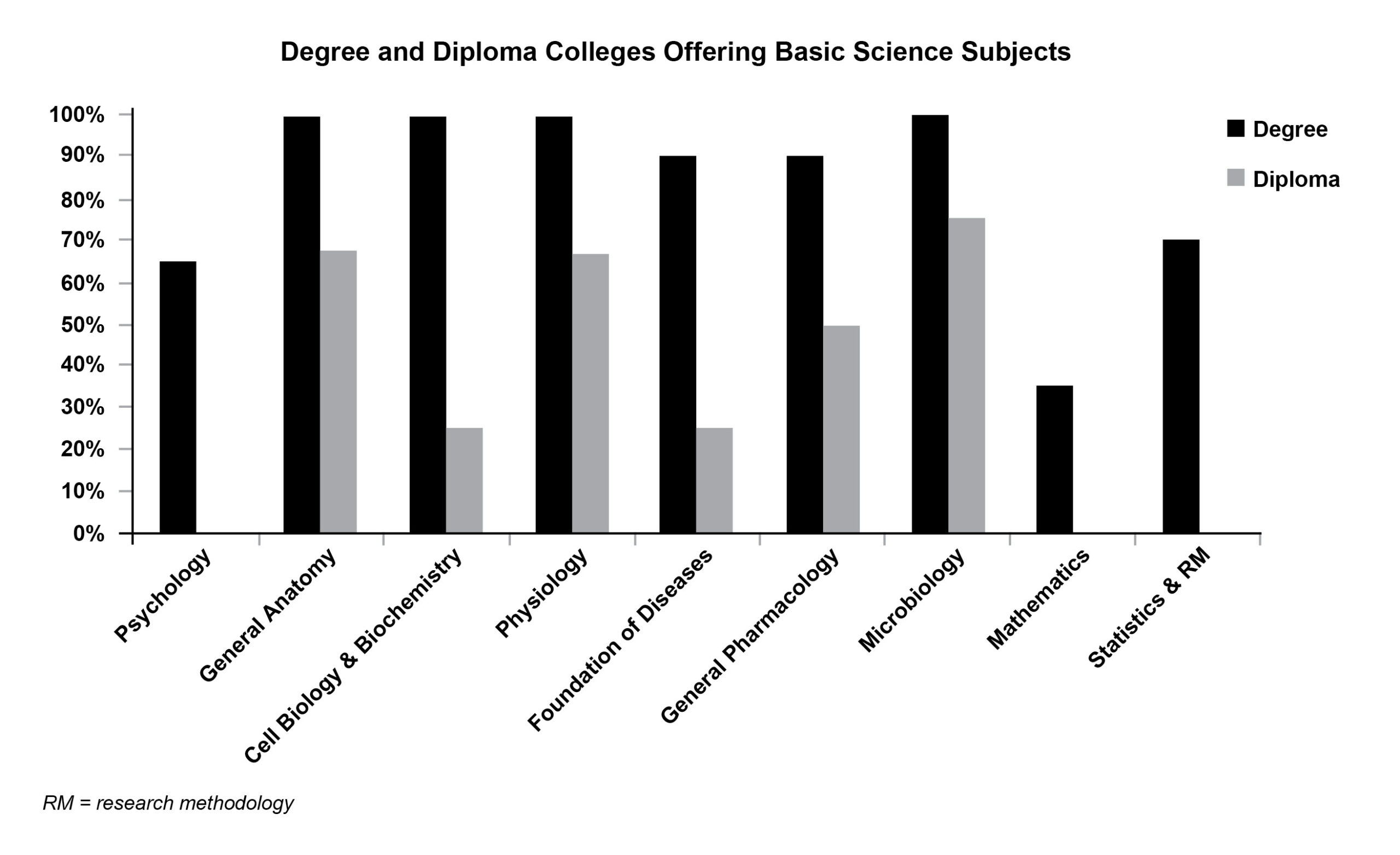
Figure 1. Click to enlarge
Ocular Anatomy and Ocular Physiology were the only two subjects offered by all the degree colleges (100%) and diploma colleges (100%). Also in the study, 50% of the degree colleges offered Practice Management as a subject, whereas diploma colleges did not offer this at all (0%). Optometry Specialties and New Technologies were also not offered by diploma colleges as shown in Figure 2.
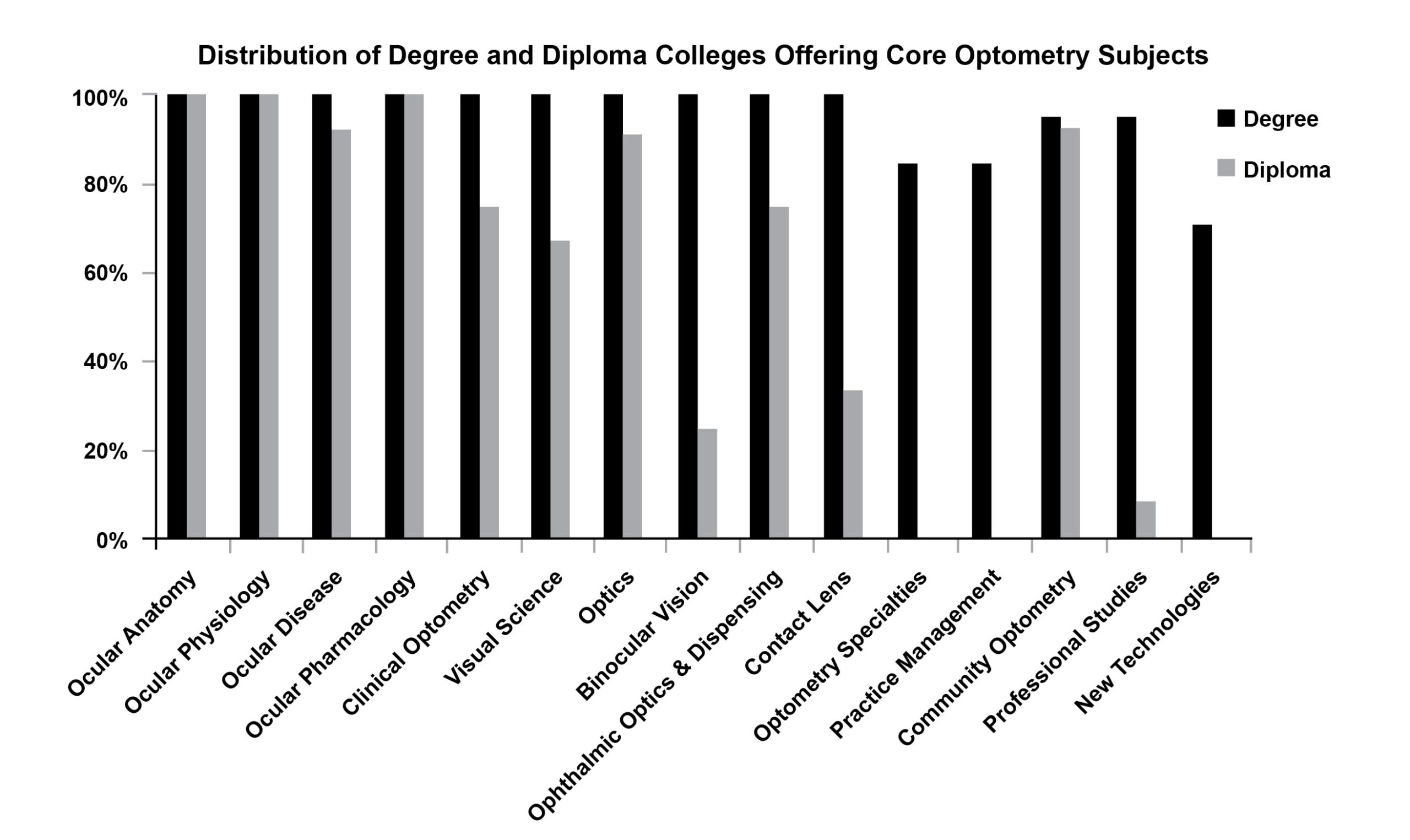
Figure 2. Click to enlarge
The subjects other than enabling/basic sciences and core optometry that were integrated into the mainstream curricula of the degree and diploma colleges involved in the study are listed in Table 3. The table indicates that degree colleges incorporated these subjects in the majority as compared with the diploma colleges. English and Communication Skills was incorporated into the majority (85%) of the degree colleges as was Computer Skills (75%). The diploma colleges involved in the study did not incorporate any subjects other than the basic and core optometry subjects. Only two diploma colleges (17%) offered English and Communication Skills and Computer Skills, and one diploma college (8%) offered Public Relations as a subject outside the basic and core optometry subjects.

Table 3. Click to enlarge
Comparison of diploma and degree curricula with WCO curricular elements
The second stage of the study involved comparing the diploma and degree curricula with the WCO curricular elements. Of the 20 degree colleges included in the study, 83% (n = 17) included all the enabling science subjects listed by the WCO compared with 34% (n = 4) of the diploma colleges. The majority, 93% (n = 19), of the degree colleges included all the core optometry subjects in their curricula compared with 57% (n = 7) of the diploma colleges (Figure 3).
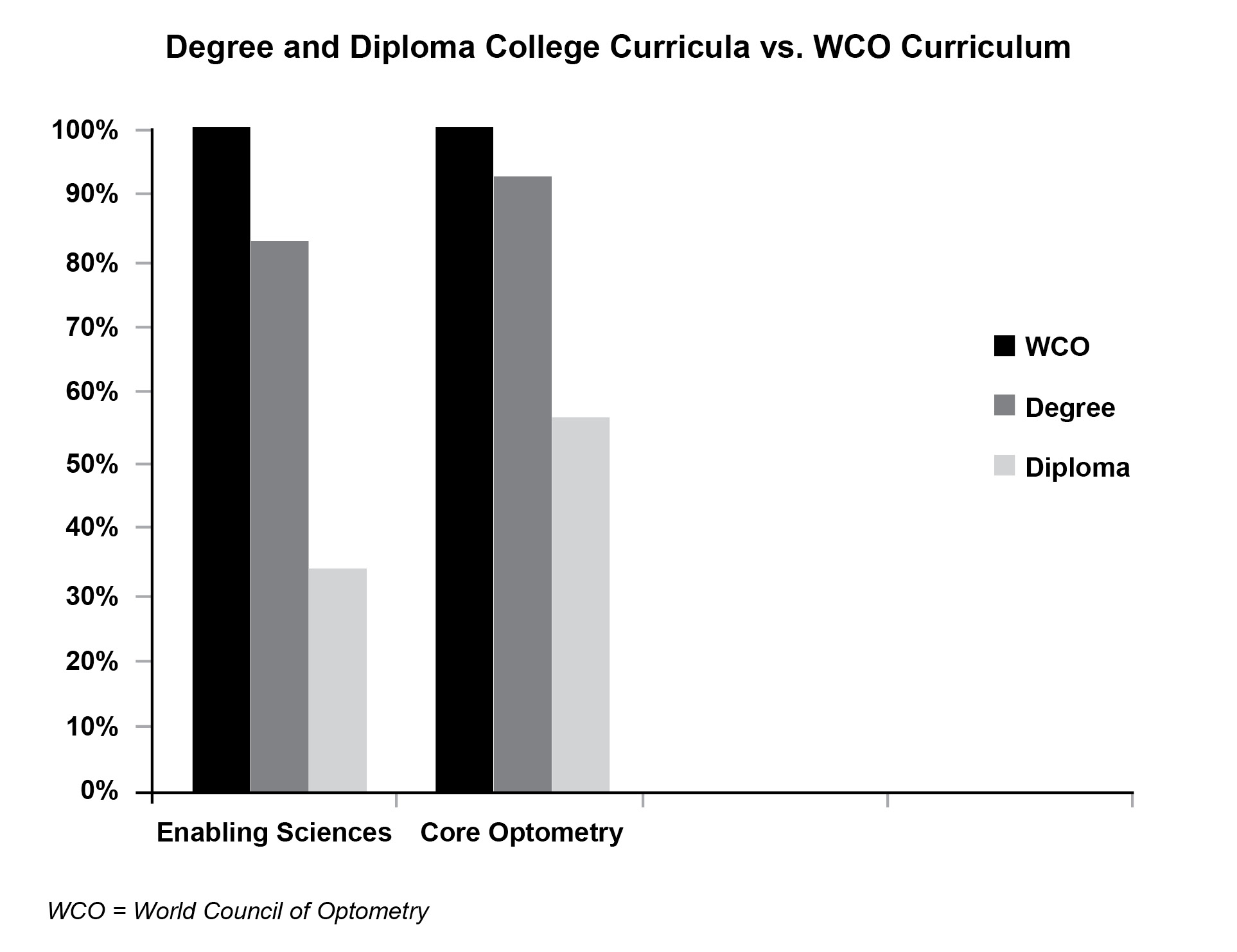
Figure 3. Click to enlarge
Syllabi were compared in terms of inclusion of enabling and core optometry subjects in order to assess the 10 elements of comprehensive eye care suggested by WCO. The analysis indicated that degree colleges included 76% of the subjects in enabling sciences and all subjects (100%) under core optometry to capacitate students with knowledge required to offer comprehensive eye examination. On the other hand, the diploma colleges offered 32% of the enabling science subjects and 82% of the core optometry subjects to enable students to offer comprehensive eye examinations (Table 4).
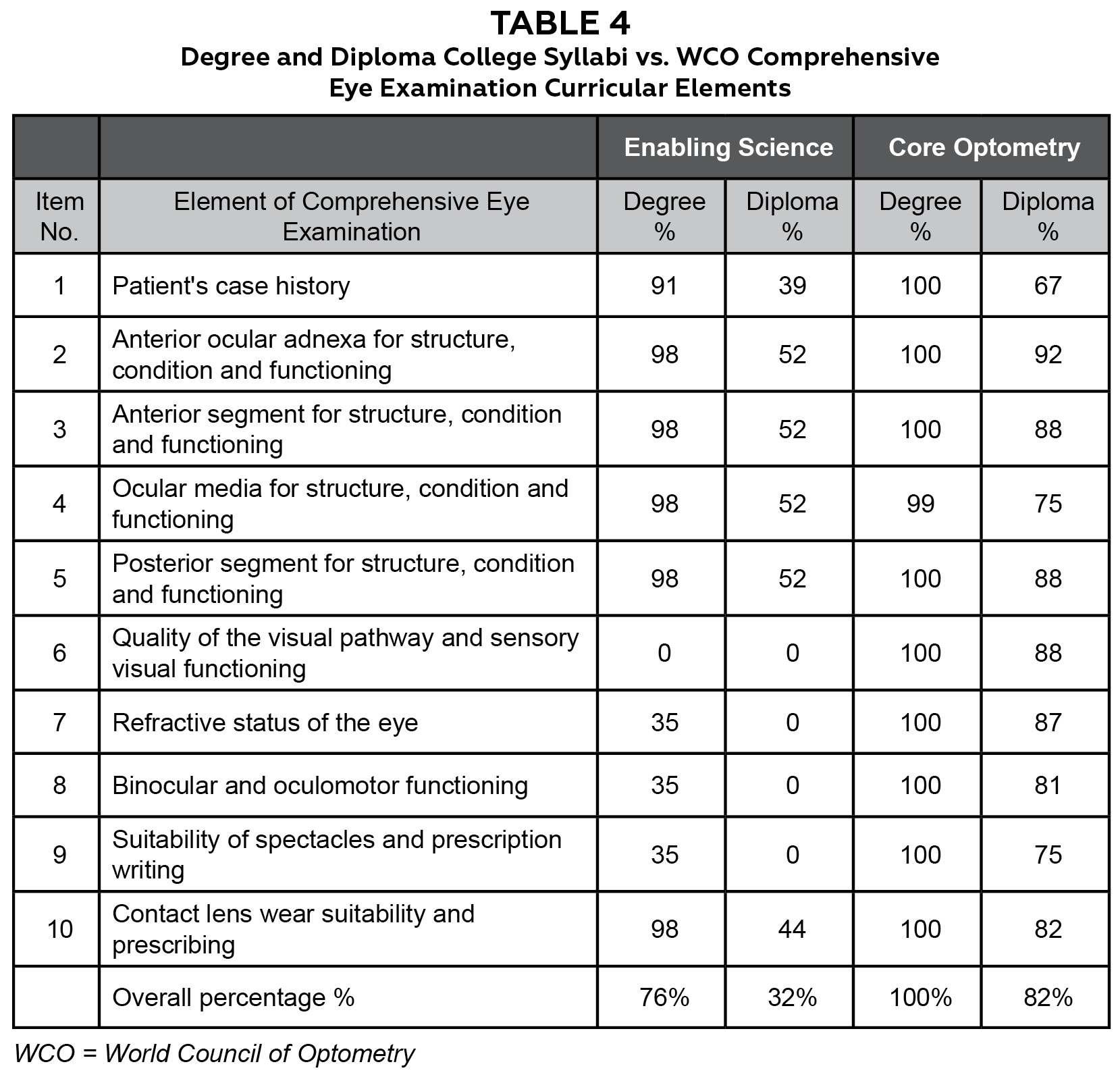
Table 4. Click to enlarge
Discussion
Diploma in optometry
The data reviewed for diploma colleges revealed that the duration of study required for a diploma was uniform (2 years) in all the states, but variations existed in terms of intake of students, curriculum, affiliation of diploma courses, nomenclature and lack of accreditation status involved in the training of MLOP or PMOAs as recognized by the NPCB&VI.15 This correlates with the observations made in the study “Thoughts on Establishing Mid-Level Ophthalmic Personnel for VISION2020.”15 MLOP practice in either a hospital or community-based setting performing tasks such as refraction and assisting surgeons in the operating theater and with pre- and post-surgical care.19 The subjects offered in the curriculum were ophthalmology-based and emphasized instrumentation, operation theater procedures, minor surgical procedures, preoperative and postoperative care as well as refraction. The enabling science subjects, which form the backbone of any optometry curriculum, were not included. The intended learning outcomes of the courses were not well-defined and the curriculum focused on preparing candidates for functions in primary or secondary eyecare centers and ophthalmological support services under supervision.10 Ophthalmologists were the primary teaching faculty in diploma programs. Research was not a part of the curriculum as it was for degree colleges. The scope of practice of diploma holders was not defined.
Globally, diploma students are exposed to didactic lectures, practical and clinical training and are expected to provide level-two services (visual function services) of the Global Competency-Based Model Scope of Practice in optometry developed by the WCO.20 In India, the diploma program prepares optometry practitioners to perform ophthalmological services under supervision and does not define their level of competence or scope of practice. Despite uniformity in diploma program duration, variations existed in nomenclature, curriculum and lack of accreditation status in India. In India, the lateral entry system allows a diploma holder to upgrade to a degree by seeking admission into the second year of the 4-year degree program as a full-time student. It is essential that diploma programs be aligned with the needs of the country through recognizing this segment of the workforce, ensuring uniformity in nomenclature and curriculum, and defining of scope of practice.
Degree in optometry
The data reviewed for degree colleges showed variations in terms of the nomenclature of the course, subjects offered in the curriculum, size of the intake of students and conduct of the examination. The findings of this study matched findings from a study conducted by Kunjeer et al. on the adequacy and relevance of the Indian optometry curricula to practicing optometrists.21 The study showed that the optometry curricula offered at the undergraduate level in India are relevant and adequate, although business and legal issues in optometry are inadequately covered.18 In the reviewed colleges, no major curriculum differences existed among the degree colleges as most of the subjects offered were based on the CMOC developed by ASCO-India. A defined scope of practice and entry and exit competencies are noted in India despite the fact that the curriculum implemented by degree colleges is comparable with the WCO curricular elements.
The subjects offered at the undergraduate level (apart from the enabling sciences and core optometry subjects, which were variable across the optometry schools) and integrated into mainstream university education were English and Communication Skills, Computer Skills, Hospital Administration, Accountancy, Regional Language, Foreign Language, Environmental Science, Indian Medicine and Telemedicine, Quality and Patient Safety, Value Education and Public Relations. The lecturing staff at the undergraduate level comprised basic science faculty, ophthalmologists and optometrists. Postgraduate qualifications in optometry were a prerequisite for appointment as academic or teaching staff at most universities offering a 4-year undergraduate degree in optometry. However, the absence of formal training in teaching and/or research among the faculty can limit ability and efficiency in terms of imparting knowledge and skills to the students in the optometry program. Traditional assessment methods were used in most colleges, which only assess theoretical knowledge rather than skills and competencies. The optometry profession requires clinical training and exposure. Although the Indian optometry curriculum includes hours of practical and clinical training, it was difficult to determine whether the colleges had the requisite infrastructure and teaching faculty to impart clinical training to students.
In all countries where the optometry profession is regulated and licensed, the curriculum is based on competency standard requirements with defined scope of practice and stringent entry and exit competencies that are cognizant of the health, safety and well-being of the public. Best practice suggests that a national regulatory body and framework could ensure harmonization and improved standards of education as well as eyecare delivery.
The study revealed that the diploma curriculum was insufficient in preparing practitioners to offer independent comprehensive optometric eye care, as defined by the WCO.
The differences in curricula of the degree and diploma syllabi necessitate defining scope of practice separately for diploma and degree holders in optometry in India. Skilled MLOP/technicians complement the services of ophthalmologists and can contribute to meeting the vision care needs of developing and developed countries.22 The need for MLOP to be part of the ophthalmic workforce in a developing and populated country like India cannot be ignored. Lack of standardization of programs, disparate entry and exit competencies, poorly defined career paths and unequal scope of practice for optometrists and MLOP are a major cause for concern in India and other countries where the profession is unregulated.19,22,23 The unethical and illegal practices of eye examinations and prescription of glasses by unqualified persons are major challenges in countries where the profession of optometry is unregulated and contribute to the public health issue of blindness.24 Hence, the question arises: What is the best approach to balancing access to “some eye care” with quality and health considerations in countries such as India.
Based on the results of the study, a possible way to improve standards of care is to recognize diploma and degree holders as separate ophthalmic cadres and design and implement accredited uniform competency-based frameworks for the two cadres as well as define scope of practice for each cadre in order to ensure quality education and service delivery in India.
The institutions offering optometry have adopted the WCO’s Global Competency-Based Model Scope of Practice in Optometry and are producing optometrists who offer services at Level Two – optometry technicians (visual function services), Level Three – optometrists (ocular diagnostic services) and Level Four – optometrists (ocular therapeutic services).9 In India, the curricula do not define the level for which graduates are prepared; therefore, the scope of practice of optometry needs to be defined, and education and training should be provided on the basis of this principle as in other countries. The optometry curriculum for the 4-year undergraduates in India does incorporate WCO curricular elements; however, lack of scope of optometry practice and an accreditation body creates optometrists with varying levels of education and training.
The results of this study indicated that not all colleges of optometry incorporate these elements in their curricula, suggesting the need for a uniform competency-based curriculum in the country. A socially responsive competency-based framework for ophthalmic technicians and optometrists should be developed in India in line with the one developed in Mozambique.25 A socially responsive competency-based framework enables students to understand the eyecare needs of the community and be involved in community service, which are needed in a developing and populous country such as India. The success of a competency-based curriculum depends on educators’ use of appropriate tools to assess competency standards in students; hence, standardized checklists and rating skills to be used by educators need to be developed along with the curricula.28
Limitations of the study
It was difficult to determine whether the subjects in the curricula were being taught to their fullest scope of imparting requisite knowledge and skills, which was a limitation of this study. Though the optometry institutions included in the study tried to be as representative as possible, the unequal distribution of colleges across the country was a limitation that led to differences in the representation of colleges in each zone.
Conclusion
This study identified significant gaps between the diploma (2-year) and degree (4-year) optometry syllabi. Variations were evident in nomenclature, student intake and student assessment as well as entry and exit competencies among Indian optometry diploma and degree colleges. The diploma syllabus does not cover basic/enabling sciences in detail. It is largely based on ophthalmology because diploma holders were originally meant to provide support to ophthalmology and services under the supervision of ophthalmologists. The diploma curriculum is not at par with curricular elements suggested by WCO and does not prepare practitioners to independently deliver comprehensive optometry services. The optometry degree syllabus is at par with the curricular elements suggested by the WCO, which prepares practitioners to deliver comprehensive optometry services independently. However, the lack of entry and exit competencies in both diploma and degree programs results in an ill-defined scope of practice. There is no accreditation body for either the diploma or degree programs in the country. The study stresses the need for the harmonization of diploma and degree programs underpinned by the designing and implementation of a uniform competency-based framework for diploma and degree programs separately with a defined scope of practice and entry and exit competency standards. This would allow optimal utilization of available human resources, both diploma and degree holders, and ensure that the eye health of the public is protected given the burden of vision impairment in India.
Recommendations
Based on the results of the study, it is recommended that diploma and degree holders be recognized as separate cadres offering eye care to the public. Their scope of practice should be defined and an accreditation body should be developed to ensure implementation of the same.
Acknowledgements
We wish to acknowledge the support of all the degree and diploma schools/colleges/institutes in the study for sharing their syllabi and consenting to be part of this study.
References
- Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012 May;96(5):614-8. doi: 10.1136/bjophthalmol-2011-300539
- Neena J, Rachel J, Praveen V, Murthy GV; Rapid Assessment of Avoidable Blindness India Study Group. Rapid assessment of avoidable blindness in India. PLoS One. 2008 Aug 6;3(8):e2867. doi: 10.1371/journal.pone.0002867
- Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008 Jan;86(1):63-70. doi: 10.2471/blt.07.041210
- NPCBVI. National Blindness & Visual Impairment Survey India 2015-2019 – A summary report [Internet]. National Programme for Control of Blindness and Visual Impairment. 2019 [cited 2020Aug11]. Available from: https://npcbvi.mohfw.gov.in/writeReadData/mainlinkFile/File341.pdf
- Eye care in India – a situation analysis. 2007 report prepared by Family Health and Development Research Service Foundation [Internet]. Boston, MA: Sightsavers International, India; [cited 2018 Apr 10]. Available from: https://www.sightsaversindia.in/wp-content/uploads/2019/03/16482_Eyecare-in-India-A-Situaltion-Analysis.pdf
- Thomas R, Paul P, Rao GN, Muliyil JP, Mathai A. Present status of eye care in India. Surv Ophthalmol. 2005 Jan-Feb;50(1):85-101. doi: 10.1016/j.survophthal.2004.10.008
- Palmer JJ, Chinanayi F, Gilbert A, et al. Trends and implications for achieving VISION 2020 human resources for eye health targets in 16 countries of sub-Saharan Africa by the year 2020. Hum Resour Health. 2014 Aug 15;12:45. doi: 10.1186/1478-4491-12-45
- Global initiative for the elimination of avoidable blindness: action plan 2006-2011 [Internet]. World Health Organization 2007; c2021 [cited 2018 Oct 3]. Available from: https://apps.who.int/iris/handle/10665/43754
- Resnikoff S, Lansingh VC, Washburn L, et al. Estimated number of ophthalmologists worldwide (International Council of Ophthalmology update): will we meet the needs? Br J Ophthalmol. 2020 Apr;104(4):588-592. doi: 10.1136/bjophthalmol-2019-314336
- De Souza N, Cui Y, Looi S, et al. The role of optometrists in India: an integral part of an eye health team. Indian J Ophthalmol. 2012 Sep-Oct;60(5):401-5. doi: 10.4103/0301-4738.100534
- Thite N, Jaggernath J, Chinanayi F, Bharadwaj S, Kunjeer G. Pattern of optometry practice and range of services in India. Optom Vis Sci. 2015 May;92(5):615-22. doi: 10.1097/OPX.0000000000000587
- Anon. Organization and Institution News, Plan to boost Indian Optometry endorsed. Optom Vis Sci. 2010;87(12)
- Kumar N. Role of optometrist in ophthalmic practice. Indian J Ophthalmol. 1976 Apr;24(1):41-2.
- Grisham DJ, Jose RT. Optometry in India: 1969. Optom Vis Sci. 1970 Nov;47(11):928-937
- Optometry Schools in India [Internet]. Tamil Nadu, India: India Vision Institute; c2015 [cited 2023 Aug 10]. Available from: https://www.indiavisioninstitute.org/resources-files/1004IVI%20-%20STATUS%20REPORT%20ON%20INDIAN%20OPTOMETRY%20SCHOOLS%202015.pdf
- Enoch JM. The Elite School; 25 Years Later! & Optometry and its future in India. Hindsight [Internet]. 2010;41:79-91. https://www.mendeley.com/reference-manager/reader/04f0861f-cb03-3ea0-8377-29203cb70c16/04e0936e-6354-af47-45e0-053f539ae08b
- University Grants Commission. UGC (act 1956) and Rules & Regulations Under the Act [Internet]. University Grants Commission. 1985 [cited 2016May3]. Available from: https://www.ugc.ac.in/oldpdf/ugc_act.pdf.
- Curricular Support Elements for an Optometry Programme [Internet]. World Council of Optometry. [cited 2022Aug.18]. https://worldcouncilofoptometry.info/wp-content/uploads/2020/08/curricular_support_element_final_web2.pdf
- Prasad NM. Thoughts on establishing mid-level ophthalmic personnel for VISION 2020 in India. Community Eye Health [Internet]. 2005 [cited 2019Dec.15];18:112. https://www.cehjournal.org/article/thoughts-on-establishing-mid-level-ophthalmic-personnel-for-vision-2020-in-india/
- A Global Competency- Based Model of Scope of Practice in Optometry [Internet]. World Council of Optometry. 2015 [cited 2022Aug.18]. https://worldcouncilofoptometry.info/wp-content/uploads/2017/03/wco_global_competency_model_2015.pdf
- Kunjeer G, Thite N, Gogate P, Jaggernath J. Adequacy and relevance of Indian optometry curricula to practicing optometrists. Clin Ophthalmol Res. 2016;4:127.
- Bogunjoko TJ, Hassan AO, Okonkwo O, Akanbi T, Ulaikere M, Akinye A, Bogunjoko H, Lawal-Sebioniga MY. Impact of middle level eye care personnel on the delivery of eye care services in South-western Nigeria. Int J Community Med Public Health. 2018;5:871.
- Awan H, Khan MD, Felch W, Spivey B, Taylor H, Resnikoff S, Gauthier T-M. Status of Ophthalmic Education and the Eye Health Workforce in South Asian Association for Regional Cooperation Countries. Asia Pac J Ophthalmol. 2014;3:74-82.
- Rai M. Challenges of Optometry in SAARC. Acta Scientific Ophthalmology [Internet]. 2019;2. https://actascientific.com/ASOP/pdf/ASOP-02-0026.pdf
- Shah K, Naidoo K, Loughman J. Development of socially responsive competency frameworks for ophthalmic technicians and optometrists in Mozambique. Clin Exp Optom. 2016;99:173-182.
- Moodley V, Loughman J, Naidoo K. Social Accountability: Introducing a new dimension in optometric education. S Afr J High Educ. 2016;30.

