
PEER REVIEWED
Bridging the Divide: Strategies to Improve Equitable Access to Quality Eyecare Services Globally Through Collaborative Optometric Education
Parres Wright, OD, FAAO, Diane van Staden, PhD, MPA, BOptom
Abstract
There is an urgent public health mandate facing the profession of optometry. The 2030 In Sight call to action demands that vision be recognized as fundamental economic, social and developmental issue, and as part of this, proposes leveraging educational settings in the strategy to end avoidable sight loss. Despite advancements in optometric education and services globally, inequities in access to quality eye care persist both within and between countries. Variable training standards and scopes of practice across the world also contribute to disparities in access to quality care; further exacerbated by inequitable access to advanced technologies that promote early diagnosis and treatment and mostly affects institutions in low- and middle-income countries. Collaborative education models between countries presents a possible solution to addressing these variable resource and training standards, as well as promoting shared learning. This paper argues that exploring collaborative teaching and learning opportunities between institutions in contextually differently regions of the world could help support global goals in respect of achieving equitable access to high-quality eye care and reducing the unnecessary causes of vision impairment or loss.
Keywords
Background
Globally, uncorrected refractive error, which is primarily the responsibility of the optometry profession, is a significant unmet health need and a major cause of avoidable vision impairment.1 Despite an increase in optometric education and services in both the developed and the developing world over the past decade, avoidable vision impairment remains a public health challenge.1 There has been long-standing inequitable distribution of the burden of unaddressed eyecare needs, with low- and middle-income countries (LMICs) typically having higher rates of blindness and vision impairment.2 Among the main challenges limiting the coverage and quality of eyecare services, particularly in developing countries, are the availability of trained human resources and access to appropriate equipment and technologies.3
Optometrists are considered primary eyecare providers responsible for diagnosing, managing and treating diseases and disorders of the eye and visual system. However, scope of practice variations from country to country or state to state, result in disparities in the level of care optometrists can provide4 both within and between countries. Even more concerning is that in some countries in the developing world, there are no established optometry schools, meaning that there isn’t a steady supply of qualified optometry personnel entering the health workforce to address these unmet eyecare needs, even where optometrists are available, essential ophthalmic equipment and consumables to manage ocular conditions are frequently unavailable or not in good working condition particularly in the public health sector of some low- and middle-income settings.5
While the last decade has seen the establishment of new optometry training programs in low- and middle-income countries,6 training standards may not be immediately regulated due to delays or bureaucracies in establishing new regulatory authorities for the profession of optometry.7 In this paper, the authors argue that there is a collective obligation facing the optometric community; specifically optometrists and optometry training institutions, to address the needs and challenges facing the profession in terms of addressing the unmet eye health needs of populations.
Opportunity exists for training institutions in better-resourced settings to collaboratively support this broader developmental agenda in partnership with institutions in developing countries as well as other supports. Collective accountability will promote shared learning as well as elevate the role of all optometric institutions beyond their primary training mandate, to that of an active participant in the global fight against avoidable vision impairment and social responsibility to reduce the disparities in access to quality optometric care.
Discussion
Disparities in Optometric Education and Scope of Practice
Optometric training varies in terms of curriculum content, duration and certification requirements both within and between countries around the world. In the United States (US), the optometric scope of practice varies between states as well and has advanced to the point where, in some states optometrists can now perform certain surgical and laser procedures. However, in most parts of the developing world where unmet eyecare needs are high, the scope of practice for optometrists is limited to diagnostic level or in some cases, just refraction. This, coupled with the additional challenge of a limited number of ophthalmologists to provide secondary and tertiary care, compounds the challenge of unmet needs; limiting opportunities for early diagnosis and treatment which reduces the risk of avoidable vision impairment. Similarly, eyecare centers and training institutions in developed countries are generally better equipped and often have access to state-of-the-art technologies, unlike the reality for most institutions in low- and middle-income countries. These contextual disparities may inadvertently be contributing to widening the gap in terms of access to quality optometric care for people everywhere – regardless of nationality and socio-economic status.
The World Council of Optometry (WCO) describes optometry as “a healthcare profession that is autonomous, educated and regulated (licensed/registered), and optometrists are the primary healthcare practitioners of the eye and visual system who provide comprehensive eye and vision care, which includes refraction and dispensing, detection/diagnosis and management of disease in the eye, and the rehabilitation of conditions of the visual system”.8 In 2024 the WCO revised its previous Competency Framework for Optometry which categorized optometry into four levels of service starting at Category 1, Optical Technology, up to Category 4, Ocular Therapeutics, with Visual Function and Diagnostic services representing Categories 2 and 3 respectively.9,10,11 The WCO now presents five competency domains reflecting the expected minimum competencies of optometric education programs globally, so optometrists can make a greater contribution towards meeting future demands of eye care. One of these domains includes public health.16
The former WCO categories were used to assess the global optometric workforce in the Global Mapping of Optometry Workforce study. The survey compiled responses from 123 of 152 countries with only 66 of 123 countries meeting the recommended 1:50,000 optometrists-population ratio.11 According to the study, there was a positive relationship between the prevalence of significant vision impairment and optometrist-population ratios. Unsurprisingly, countries with low Gross Domestic Product (GDP) had higher optometrist-patient ratios and greater deficits of optometrists.
Though there are varying levels of practice and scope of practice between countries, globally, one optometrist serves an average of 20,479 people.11 However, in Central Sub-Saharan Africa, a single optometrist serves 1,198,141, while in Western Europe the ratio is 1:3,877. This highlights the imbalance disadvantaged developing countries face in terms of addressing unmet eyecare needs, improving access and providing quality care. Of the 21 Global Burden of Disease (GBD) regions (Figure 1), three did not have any institution within its countries to train optometrists.11 Regions most affected were Central Asia, Central Sub-Saharan Africa and Oceania.11 Approximately half of the countries surveyed regulate optometry as a profession. Furthermore, optometry was a recognized profession in all high-income regions, with 34% of countries imposing mandatory continuing professional education to maintain clinical competency and enforce up-to-date practices.10
Since public health now has a stronger global focus in optometry,16 this should be reflected in the curricula and training models of optometry programs everywhere, if 2030 global targets are to be met.
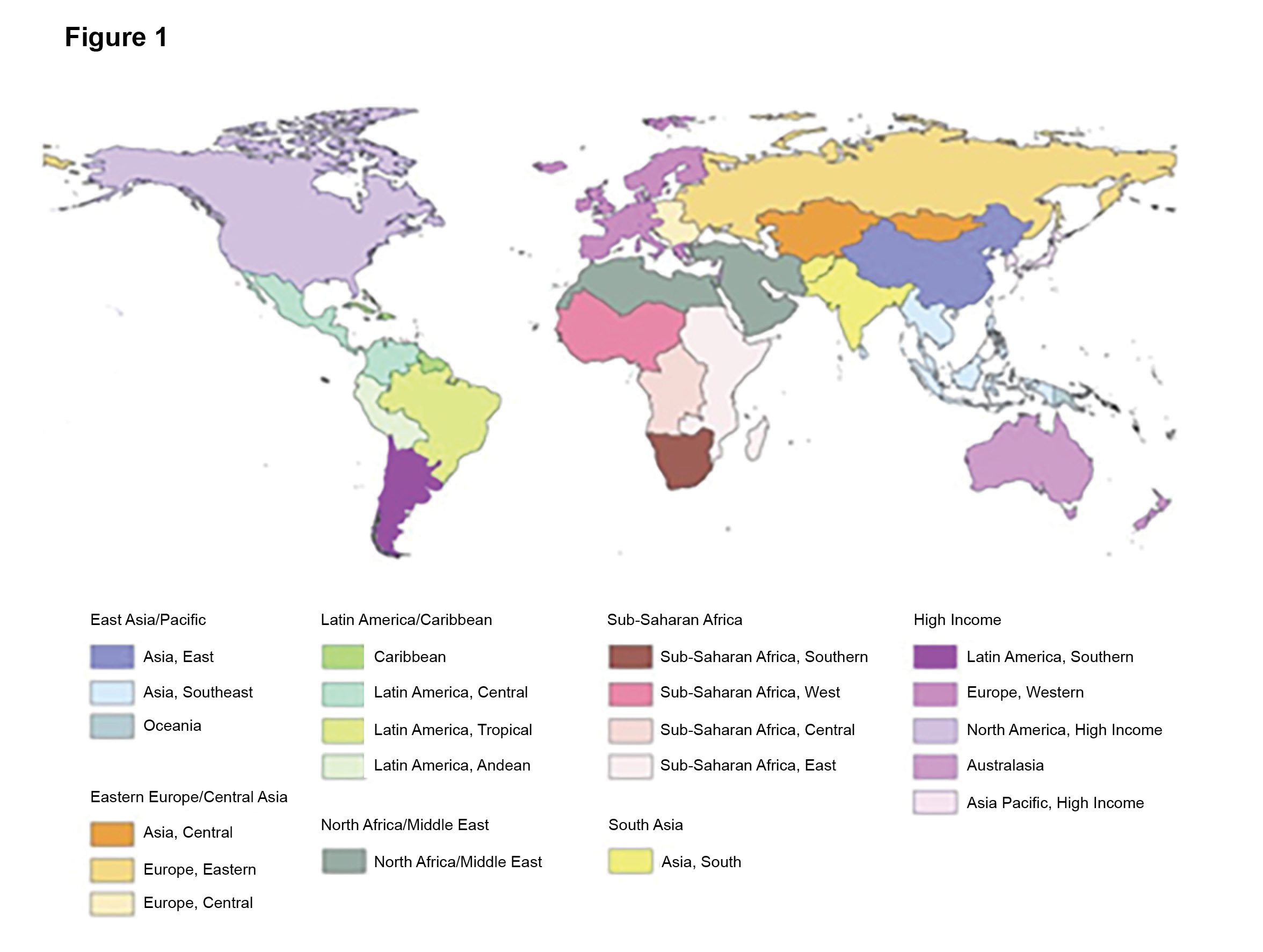
Figure 1:Figure 1 Map of the 21 GBD regions.Source: https://www.researchgate.net/figure/Map-of-the-21-GBD-regions-GBD-Global-Burden-of-Disease-Risk-Factors-and-Injuries_fig1_233955589. Click to enlarge
The rise in demand for eyecare services
Population aging, along with a greater awareness of rehabilitation options for people with severe vision impairment, is resulting in a rise in the demand for vision care services in general, and low vision services in particular. All members of the “Baby Boomer” generation, which includes those born in 1946-1964 will reach age 65 years and older by 2029, bringing the US population over 75 to 12%.13 This growth in the aging population in the US mirrors the ever-growing, aging populations globally. By 2030, one in six people in the world will be aged 60 years or over and will total approximately 1.4 billion people.14 Putting this in perspective, the over 60 population of the world will double by 2050 and those over age 80 is expected to triple between 2020 and 2050, reaching 426 million.14 This trend started in high-income countries, like Japan, whose over 60 population has already reached 30%.14 Currently, low- and middle-income countries are experiencing the greatest change regarding population aging.14
With the aging of populations, the numbers of those with vision loss are expected to increase. In 2019 it was reported that a minimum of 2.2 billion individuals worldwide have some form of visual impairment.5,15 It is projected that by 2050, 6.95 million people in the US will have vision impairment and 2.09 million people will have blindness.13 In addition to aging leading to increased numbers of those with vision loss, studies have also shown that visual impairment is also expected to rise among working-aged adults worldwide. “In 2019, the highest number of visual impairment associated disability-adjusted life years (DALYs) among working-age individuals was documented in South Asia, whereas the lowest was documented in Oceania.”15 Vision impairment negatively impacts employment opportunities and as such, the increasing trend of vision loss in working-aged adults is poised to be a global public health concern.15 Optometrists worldwide must therefore be properly, trained, educated and equipped to address these growing needs preventing and treating vision loss and blindness.
Opportunities for shared learning through teleoptometric education
Given the disparities between how optometrists are training globally, and the potential impacts of this on widening the gap in terms of equitable access to quality care, finding innovative ways to bridge training and development gaps between the different regions of the world, may prove mutually beneficial for training institutions.
Studies have highlighted the lack of access to equipment and technologies as a barrier to delivering quality eye care in LMICs.12 The reality is that, given the economic and structural problems facing developing nations, resource acquisition for eye care must compete with other more pressing health system demands and may therefore not be a priority. For many of these countries, there is no short-term fix to address resourcing gaps.
Within this digital age, our world is essentially borderless; meaning that the lack of skilled human resources, as well as access to routine equipment or diagnostic technologies affecting certain countries need not be a limitation in terms of providing quality primary eyecare services in any setting. Innovative strategies such as remote, real-time consultations and the use of diagnostic software applications which are increasingly being utilized to serve remote communities, can also be employed to support training in various parts of the world where resourcing is a challenge.
Remote optometry is emerging as a viable tool to address unmet resource and skills needs by using telemedicine, making access to more specialized services accessible for people in outlying areas, even in developing countries. Teleoptometry, and by extension teleoptometric education, allows for increased access to care in remote areas worldwide and increased timeliness of care. It also supports the training needs of optometry students in developing countries to help them be better prepared for the future of eye care and rapidly advancing technologies. However, this need not be a one-sided benefit as underresourced institutions may also have rich lessons to share on creative approaches to instruction when standard resources are not available, particularly when students are engaging in service learning outside of the academic center. These innovative models of teaching and learning as well as unique clinical cases can be a shared learning opportunity.
The post-COVID world removed geographical barriers to shared learning and resistance to virtual and remote clinical care and training models. Where institutions in the developed world may lack specific expertise available at institutions in the developing world, various lectures or clinical training can also be facilitated virtually. Much like learning online has become more commonplace even within the health professions, institutional collaboration and shared learning using digital technologies at higher education level is a very real possibility and should rightly be explored particularly in the context of growing needs and limited resources. Opportunity exists to bridge the access divide in the areas of training and diagnostic services in underresourced countries, while also creating diversified teaching opportunities and rich experiential learning opportunities, including international exchanges, for students in high income countries.
Where health partnerships exist, support from established partners for improved regulations and quality standards can help strengthen institutions still in a developmental stage, though both partners stand to benefit from shared knowledge, clinical cases, etc.
Graduates who make a difference
To build a workforce of optometrists trained to keep up with the burgeoning demand for eye care requires focusing on recruitment of diverse candidates and constructing robust, innovative training programs and curricula. To address some of the global challenges in providing high-quality eye care, insufficient numbers of optometrists, and discrepancies in levels of training the WHO developed the Eye Care Competency Framework (ECCF).9 This framework utilized a wide range of eyecare professionals from both high- and low-income countries. The aim was “to facilitate eyecare workforce planning and development by providing a comprehensive set of competencies and activities that encompass the diverse roles represented by eyecare workers.”9 This competency framework is a tool to ”strengthen the alignment of the workforce with the population’s needs.”9 The value of such a framework would be greatest when designed to be applied to any context, particularly to low- and middle-income countries, where tools for workforce development are limited.9 Learnings from both contexts would be invaluable in shaping the future of training and scope of practices in various regions of the world; with such guidance critical in educating and constructing the next generation of eyecare professionals.
Rise in new optometry schools
The world is favorably responding to global calls for increased access to eyecare services, with many new optometry schools in the US and Africa being opened to address the availability of skilled personnel to meet the growing eye health needs. Just 15 years ago, only one in four countries in Sub-Saharan Africa had optometry training programs. Since then, new optometry schools have opened across the African continent. With the development of new optometry programs across the US, the opportunity to do teaching and learning differently should be explored, and to include not only a global public health and developmental mandate within the ethos of training programs, but to further explore partnerships and collaboration opportunities which strengthen training via hybrid in-person and remote learning within a global optometry perspective, regardless of country of training.
Conclusion
The disparities in terms of optometric care standards across the world have been well documented. The authors believe that there is an opportunity for the optometry community globally, specifically optometry training institutions, to collaborate on improving access to better quality care through innovative training models and the use of technology. Technology has expanded the realm of what is possible via teleoptometry. Where resource gaps exist, the proposed use of a teleoptometry model to strengthen a collaborative public health approach to training could potentially lead to a more highly trained, better-equipped optometric workforce for all students through shared virtual learning.
By rethinking what we teach, and how we teach in terms of addressing the needs and challenges facing the profession, we can potentially create rich opportunities for mutual learning, share contextual lessons in advancing the access and quality of care, and ultimately move closer to the ideal of a single global standard for optometry education and scope of practice. Finally, the development, use and sharing of creative options to collectively address the profession’s public health mandate improves equity in access to care globally, as well as egalitarianism to high-quality eye care.
References
- Blindness and vision impairment [Internet]. Geneva, Switzerland: World Health Organization; c2023 [cited 2024 Jan 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment
- Forrest SL, Mercado CL, Engmann CM, et al. Does the current global health agenda lack vision? Glob Health Sci Pract. 2023 Feb 28;11(1):e2200091. DOI: 1-.9745/GHSP-D-22-00091
- Graham R. Facing the crisis in human resources for eye health in sub-Saharan Africa. Community Eye Health. 2017;30( 100):85–7.
- Ezinne NE, Kwarteng MA, Tagoh S, Ekemiri KK, Ogbonna G. Scope of optometry practice in Trinidad and Tobago: a cross-sectional study. Health Sci Rep. 2023 Oct 31;6(11):e1667. DOI: 10.1002/hsr2.1667
- World report on vision [Internet]. Geneva, Switzerland: World Health Organization; c2019 [cited 2024 Jan 22]. Available from: https://www.who.int/publications/i/item/9789241516570.
- Abu SL. History and current status of optometric education in Africa. Hindsight: J Optom Hist. 2020 Sep 28;51(4):84–92. DOI: 10.14434/hindsight.v51i4.31557
- Moodley VR. Towards a culture of quality assurance in optometric education in sub-Saharan Africa. Afr Vision Eye Health. 2019 Mar 6;78(1). DOI: 10.4102/aveh.v78i1.462
- WCO’s concept of optometry [Internet]. St. Louis, MO: World Council of Optometry; [cited 2023 Oct 7]. Available from: https://worldcouncilofoptometry.info/concept-of-optometry/.
- Yu M, Keel S, Mariotti S, Mills JA, Müller A. Development of the WHO eye care competency framework. Hum Resour Health. 2023 Jun 19;21(1):46. DOI: 10.1186/s12960-023-00834-4
- Kiely PM. A global competency-based model of scope of practice in optometry [Internet]. South Melbourne, Australia: Optometry Australia; [cited 2024 Jan 22]. Available from: https://worldcouncilofoptometry.info/wp-content/uploads/2017/03/wco_global_competency_model_2015.pdf
- Naidoo KS, Govender-Poonsamy P, Morjaria P, Block S, Chan VF, Yong AC, Bilotto L. Global mapping of optometry workforce. Afr Vision Eye Health. 2023;82(1):a850. DOI:10.4102/AVEH.V82I1.850.
- Sengo DB, Salamo ZMA, dos Santos II d’Alva B, et al. Assessment of the distribution of human and material resources for eye health in the public sector in Nampula, Mozambique. Hum Resour Health. 2023 Mar 31;21(1):27. DOI: 10.1186/s12960-023-00812-w
- Varma R, Vajaranant TS, Burkemper B, et al. Visual impairment and blindness in adults in the United States: demographic and geographic variations from 2015-2050. JAMA Ophthalmol. 2016 Jul 1;134(7):802–9. DOI: 10.1001/jamaopthalmol.2016.1284
- Steverson M. Ageing and health [Internet]. Geneva, Switzerland: World Health Organization 2022; [cited 2023 Oct 6]. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- Chen J, Yang C, Zheng W, et al. Global, regional, and national epidemiology of visual impairment in working-age individuals, 1990–2019. JAMA Ophthalmol. 2024 Jan 1;142(1):25–32. DOI:10.1001/jamaophthalmol.2023.5617
-
16. WCO Competency Framework for Optometry [Internet]. Saint Louis, MO: World Council of Optometry; c2024 [cited 2024 Nov 30]. Available from: https://worldcouncilofoptometry.info/wp-content/uploads/2024/02/WCO_Competency-Framework-for-Optometry.pdf

