
PEER REVIEWED
Normotensive Glaucoma Follow-Up with Incidental Finding of Choroidal Neovascular Membrane
Ryan Bulson, OD, MS, FAAO, and Ambar Faridi, MD
Abstract
Behind cataracts, glaucoma is the second leading cause of blindness worldwide. Patients with glaucoma are followed at regular intervals for testing to confirm stability of the disease; however, providers may need to divert from planned glaucoma testing when clinical findings suggest progression of comorbid ophthalmic conditions. This case report describes a patient presenting for a routine glaucoma follow-up appointment who was subsequently diagnosed with an acute choroidal neovascular membrane due to conversion from non-neovascular to neovascular age-related macular degeneration. The case highlights the management of normotensive glaucoma and both non-neovascular and neovascular macular degeneration.
Key Words: glaucoma, macular degeneration, optical coherence tomography, fluorescein angiography, visual field
Background
Normotensive glaucoma is a progressive optic neuropathy that follows clinical patterns of primary open-angle glaucoma in the absence of elevated intraocular pressure (IOP).1 Patients with normotensive glaucoma are typically followed at regular intervals several times per year for clinical examination of the optic nerve and for monitoring of IOP, automated visual fields and optical coherence tomography (OCT). The diagnosis and management of glaucoma are often complicated by ocular comorbidities, such as age-related macular degeneration (ARMD). While the exact pathogenesis in unclear, ARMD is characterized by abnormal deposition of acellular, polymorphous debris called drusen between the retinal pigment epithelium and Bruch’s membrane, a condition that represents the leading cause of irreversible blindness in people 65 years of age and older in the developed world.2 This case report describes a 70-year-old Caucasian female who presented for a visual field test and follow-up for normotensive open-angle glaucoma. Due to a new complaint of a central blurred spot in the right eye as well as a new central depression on visual field testing, the patient, who was also being followed for non-neovascular ARMD, was dilated and incidentally found to have a subretinal macular hemorrhage from an acute choroidal neovascular membrane (CNVM) related to neovascular macular degeneration. The case highlights the importance of a careful case history and the need for clinicians to divert from planned testing based on new information offered by the patient. This case is appropriate for optometry students in years two through four as well as optometry residents. It can be utilized in a seminar, laboratory, classroom or clinical setting.
Case Description

Table 1.
Click to enlarge
A 70-year-old Caucasian female presented to the eye clinic for a normotensive glaucoma follow-up appointment, including her annual threshold visual field. Her glaucoma was diagnosed in the right eye in 2012 based on moderate optic nerve cupping, inferior-temporal thinning of the retinal nerve fiber layer (RNFL) on OCT, an early superior nasal arcuate visual field defect, and strong family history (mother). Visual field and OCT findings of the left eye were unremarkable at the time of diagnosis; however, when treatment was discussed, the patient elected to initiate treatment of her left eye prophylactically. The patient’s glaucoma was well-controlled on latanoprost ophthalmic solution 0.005% instilled in both eyes before bedtime. Her pertinent glaucoma findings are summarized in Table 1. In addition to glaucoma, her ocular history was significant for intermediate non-neovascular ARMD, a hemorrhagic posterior vitreous detachment in the right eye diagnosed four months prior, non-visually-significant bilateral nuclear sclerotic cataracts, and mild dry eyes. Her medical history was significant for hypertension, asthma, hyperlipidemia, and previous cervical cancer. Her medications included metoporolol tartrate 50 mg BID, ipratropium bromide 20 mcg/albuterol sulfate 100 mcg inhaler QID, and gemfibrozil 600 mg BID. Additionally, she used AREDS2 formula multivitamins BID and was a current daily smoker. Significant allergies included piperacillin and clonidine.
The patient’s chief complaint was a blurred spot in her right eye for the past week. The spot was most noticeable towards the end of the day and seemed to improve with blink and the use of artificial tears. She reported no complaints with the left eye and observed no other changes to her overall vision. There was no metamorphopsia observed from either eye when using her home Amsler grid.
Incoming corrected distance visual acuity was OD: 20/30-2 and OS: 20/30+. Previous incoming corrected visual acuities were OD: 20/20- and OS: 20/25-. Pupils were equal, round and reactive to light without afferent pupillary defect. Extraocular motilities were full and concomitant OU. Cover test revealed orthophoria at distance and 6 prism diopters exophoria at near. A manifest refraction of +0.50-1.25×105 corrected the right eye to 20/25 and a manifest refraction of +0.50-1.25×105 corrected the left eye to 20/25. Anterior segment exam was significant for mild punctate epithelial erosions within the inferior one-third of each cornea, with a tear break-up time of 2-3 seconds OU. The 24-2 threshold visual field testing was reliable in both eyes and showed a large central relative defect in the right eye and two non-clustered paracentral relative defects inferiorly in the left eye. (Figures 1-2) OCT of the right optic nerve revealed inferior-temporal sector RNFL thinning with borderline quadrant RNFL thinning inferiorly while the left eye demonstrated no significant thinning of the RNFL. (Figure 3) Due to the patient’s chief complaint, slight reduction in best-corrected visual acuity and visual field findings, a dilated fundus exam was performed. This examination revealed bilateral grade 2 nuclear sclerotic cataracts, clear vitreous OU, optic nerves with cup to disc ratios of 0.70H/0.75V OD and 0.60H/0.70V OS, normal vasculature OU, and a flat and intact peripheral retina bilaterally. Examination of the right macula revealed course mottling with several small and intermediate drusen as well as a subretinal hemorrhage superior to the macula. (Figure 4) The left macula showed a mottled appearance with several small and intermediate drusen. (Figure 5) OCT of the macula was performed and showed confluent central drusen with a pigment epithelial detachment with overlying subretinal fluid OD, and confluent central drusen without subretinal fluid OS. (Figures 6-8)
 Figure 1. 24-2 Humphrey SITA Standard visual field test OD on 06/28/16 showing good test reliability with a large central relative defect. |
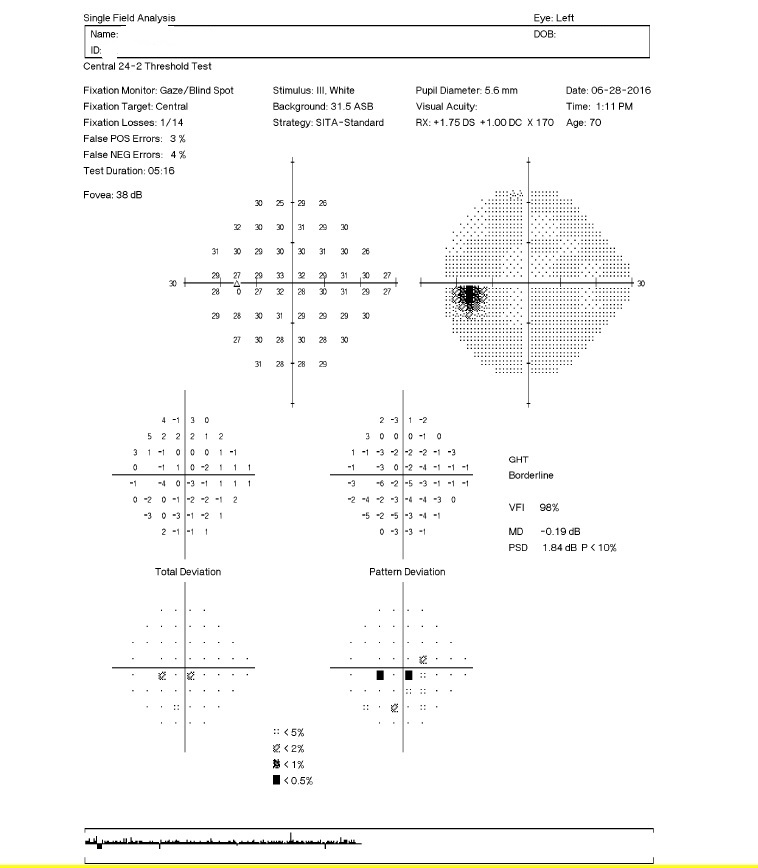 Figure 2. 24-2 Humphrey SITA Standard visual field test OS on 06/28/16 showing good test reliability with two non-clustered paracentral relative defects inferiorly. |
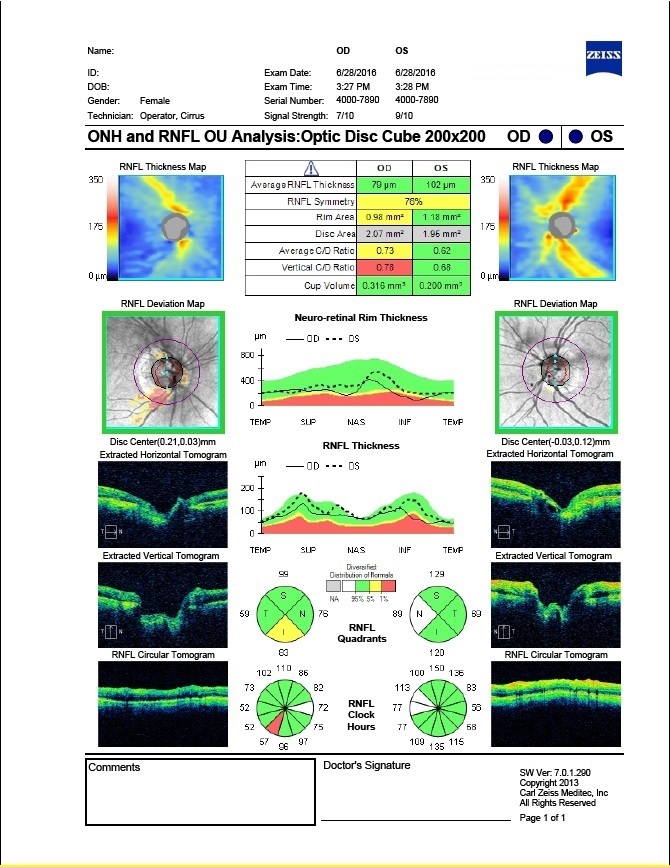 Figure 3. Optic disc OCT OU on 06/28/16 showing borderline RNFL layer thinning inferiorly OD and no significant thinning of the RNFL OS. |
 Figure 4. Fundus photograph OD on 06/28/16 showing a mottled appearance of the right macula with several small and intermediate drusen as well as a subretinal hemorrhage slightly superior to the macula. |
 Figure 5. Fundus photograph OS on 06/28/16 showing a mottled appearance of the left macula with several small and intermediate drusen. |
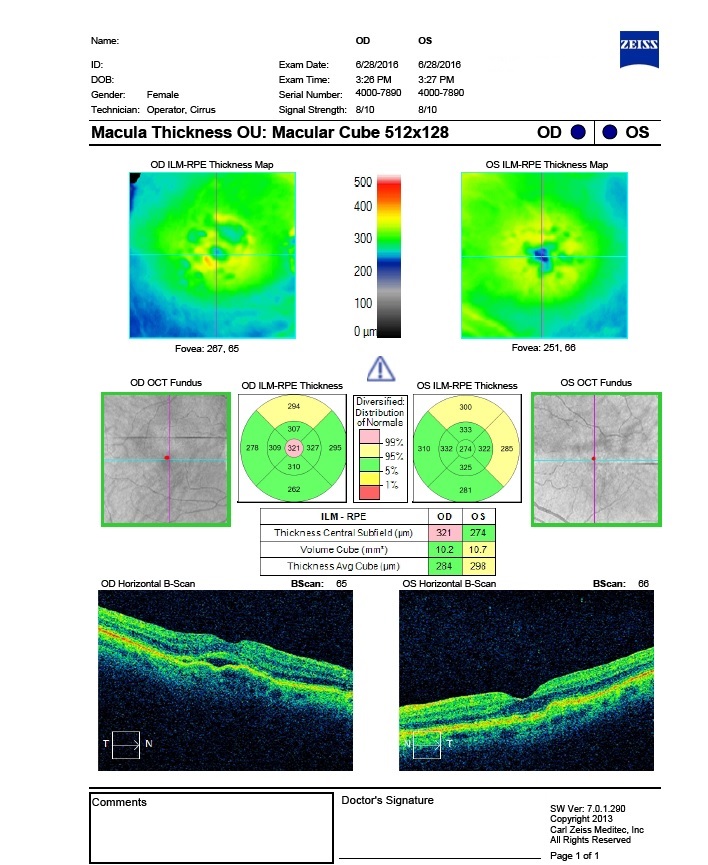 Figure 6. Macular Cube OCT OU on 06/28/16 showing increased central macular thickness of 321 µm OD and normal central macular thickness of 274 µm OS. |
 Figure 7. Five Line Raster Macular OCT OD on 06/28/16 showing confluent central drusen and pigment epithelial detachment with overlying subretinal fluid causing macular elevation. |
 Figure 8. Five Line Raster Macular OCT OS on 06/28/16 showing confluent central drusen with normal macular contour and thickness. |
A same-day consult with a retina specialist was requested, and fluorescein angiography (FA) was performed. (Figures 9-10) FA revealed a region of blockage superior to the fovea corresponding to the area of subretinal hemorrhage; however, within this region, specifically the portion superior-nasal to the fovea and corresponding to a pigment epithelial detachment, there was an area of early stippled hyperfluorescence that on the later frame had ill-defined leakage, i.e., occult leakage. Additionally, there was staining of numerous drusen present inferior to the fovea. Based on the FA study, the patient was diagnosed with an occult CNVM in her right eye related to exudative macular degeneration and subsequently treated with a 0.5-cc intravitreal injection of 1.25 mg intravitreal bevacizumab in the right eye. The patient was advised to continue AREDS formula vitamins and to monitor for vision changes at home with an Amlser Grid. Follow-up was scheduled with the retina specialist for four weeks later.
 Figure 9. Fluorescein angiography OD at 1:39 showing early-phase blockage superior to the fovea corresponding to the area of subretinal hemorrhage. Superior-nasal to the fovea there is an area of early stippled hyperfluorescence corresponding to the area of pigment epithelial detachment. Additionally, there is staining of numerous drusen present inferior to the fovea. |
 Figure 10. Fluorescein angiography OD at 7:25 showing a late-phase ill-defined area of leakage superior-nasal to the fovea. |
Education Guidelines
Key concepts
- Diagnosis and management of normotensive glaucoma
- Diagnosis and management of non-neovascular macular degeneration
- Diagnosis and management of neovascular macular degeneration
- Interpretation of OCT for glaucoma and macular degeneration
- Interpretation of fluorescein angiography
Learning objectives
- To understand and interpret pertinent testing for patients with glaucoma, including visual field and OCT
- To identify signs of neovascular macular degeneration on OCT
- To identify signs of neovascular macular degeneration on fluorescein angiography
- To understand how non-neovascular and neovascular macular degeneration are diagnosed
- To understand how non-neovascular and neovascular macular degeneration are managed
Discussion questions
- Knowledge and concepts required for critical review of the case:
- What are the diagnostic criteria for a patient with normotensive glaucoma?
- What are the risk factors for development and progression of normotensive glaucoma?
- What are the diagnostic criteria for a patient with non-neovascular macular degeneration?
- What are the diagnostic criteria for a patient with neovascular macular degeneration?
- Differential diagnosis:
- What are the differential diagnoses based on the patient’s chief complaint?
- What are the justifications for dilating a patient with a similar chief complaint?
- What other conditions could explain the patient’s visual field results?
- What other conditions could explain the patient’s optic nerve OCT results?
- What other conditions could explain the patient’s macular OCT results?
- How do OCT and visual field findings correlate?
- Disease management
- Describe the treatment options for glaucoma
- What are the pharmaceutical, non-surgical treatment options for glaucoma?
- Describe the different classes of pharmacological agents. For each agent, describe: drug class, dosage schedule, expected IOP reduction
- What are the surgical treatment options for glaucoma?
- When are AREDS multivitamins clinically indicated for macular degeneration?
- Describe the treatment options for neovascular macular degeneration
- Patient education
- What lifestyle modifications would be recommended for a patient with macular degeneration?
- How would glaucoma be explained to a patient to facilitate an understanding of the condition?
- How would both neovascular and non-neovascular macular degeneration be explained to a patient to facilitate an understanding of the conditions?
- For a patient acutely diagnosed with neovascular macular degeneration, how would one best explain to the patient what will happen at the exam with the retina specialist?
- What is the long-term visual prognosis for a patient diagnosed with glaucoma?
- What is the long-term visual prognosis for a patient diagnosed with non-neovascular macular degeneration? Neovascular macular degeneration?
- Critical thinking
- When should surgical treatment be recommend over pharmacological therapy for a patient with glaucoma?
- When should patients with glaucoma be referred to a glaucoma specialist?
- When should patients with macular degeneration be referred to a retina specialist?
Learning assessment
- Clinical skills such as high plus fundoscopy, binocular indirect ophthalmoscopy, acquisition of OCT images, automated visual field testing, and fundus photography can be tested in a laboratory or clinical proficiency exam
- Clinical thinking skills and knowledge base of the clinical signs of glaucoma and macular degeneration can be tested via review of stereoscopic optic nerve photographs, fundus photography, optic nerve/macular OCT scans, automated visual field interpretation and FA images. This would ideally be done in a small-group setting, such as a laboratory or seminar, with the faculty member or clinical attending serving as the mediator of the discussion and directing the discussion to cover salient points as appropriate. The material could also be reviewed in a larger group or classroom setting as a Grand Rounds case and assessed as part of a written exam
- Literature review on management of glaucoma and macular degeneration can be conducted and written up as a capstone or thesis project
Discussion
Glaucoma is a progressive optic neuropathy characterized by death of the RNFL ganglion cells.1 It represents the second leading cause of blindness worldwide behind cataracts.1 Pertinent testing for the diagnosis of glaucoma includes Goldmann applanation tonometry, corneal pachymetry, gonioscopy, stereoscopic ophthalmoscopy of the optic nerve head, RNFL analysis (most commonly via OCT) and threshold visual field testing.3 Evaluation of the macular ganglion cell complex (GCC) via spectral domain OCT has also recently emerged as a promising new tool for diagnosing and monitoring progression of glaucoma as the thickness of this region is reduced as glaucoma develops and progresses.4 However, as in the current case, concurrent macular disease may confound the results of this test, making interpretation of GCC loss more challenging.5
Normotensive glaucoma is defined as progressive optic neuropathy with subsequent visual field constriction and RNFL thinning in the presence of open angles on gonioscopy and normal IOP (<21mmHg).6 While normotensive glaucoma has historically been considered a distinct entity from primary open-angle glaucoma, where IOP is elevated, normotensive glaucoma may represent a continuum of the open-angle glaucomas whereby the mechanism changes from IOP-mediated to IOP-independent factors, such as abnormal vasoregulation, which produces transient ischemia. Increased frequency of disc hemorrhages as well as higher prevalence of Raynaud’s phenomenon, migraines and sleep apnea in patients with normotensive glaucoma support the role of vascular perfusion in the pathogenesis of normotensive glaucoma.6 Other risk factors for normotensive glaucoma include age, female gender and Asian heritage.3

Table 2.
Click to enlarge
Despite normal intraocular pressure, the standard treatment for normotensive glaucoma is similar to that of primary open-angle glaucoma; that is, reduction of intraocular pressure.1 Topical pharmaceutical agents, summarized in Table 2, represent the first-line treatment for normotensive glaucoma. Surgical interventions including laser trabeculoplasty, trabeculectomy and sclerotomy are considered in patients who are unresponsive to pharmaceutical treatment or that demonstrate progression despite sufficient IOP reduction.1 The Collaborative Normal Tension Glaucoma (CNTGS) study found a 30% or more reduction in IOP reduced progression of visual field loss over five years, thus, this remains the standard treatment goal for most patients with normotensive glaucoma.7 In the CNTGS, 57% of patients achieved a 30% IOP reduction with topical medication and/or laser trabeculoplasty, while the remaining 43% required filtering surgery.7 Thus, some patients with normotensive glaucoma will not achieve sufficient IOP reduction from pharmacological therapy alone and therefore require co-management with an ophthalmologist specializing in glaucoma.
The patient discussed in this article presented primarily for a visual field test, and was found to have a large central defect in the right eye that had not been previously noted. The left eye was found to have a smaller paracentral defect that was not noted on the previous visual field test. OCT findings of the optic nerve did not correspond to the visual field defects OD/OS. Due to these visual field results, as well as the patient’s chief complaint and slight reduction in best-corrected acuity, a dilated exam was performed to rule out progression of her macular degeneration. Although the patient did show signs of dry eyes, which might have explained these factors, the asymmetry of the patient’s complaint and visual field defect was not consistent with the relatively symmetrical mild dry eye findings.
Age-related macular degeneration is the leading cause of blindness and visual impairment in people 65 years and older in the United States.8-9 The condition is generally divided into two groups: non-neovascular or neovascular, with the former usually preceding the latter.10 Non-neovascular (also called non-exudative or “dry”) macular degeneration is characterized by the presence and accumulation of yellow lipid deposits called drusen below the retinal pigment epithelium of the retina.10 Accumulation of drusen damages the retinal pigment epithelium, resulting in large areas of geographic atrophy as well as expression of angiogenic cytokines such as vascular endothelial growth factor (VEGF).10 In neovascular (also called exudative or “wet”) macular degeneration, VEGF stimulates development of choroidal neovascularization (CNV) causing the characteristic clinical findings of subretinal hemorrhage, fluid exudation, lipid deposition, detachment of the retinal pigment epithelium from the choroid and, ultimately if left untreated, fibrotic scars.10 Neovascular macular degeneration is responsible for 80-90% of severe visual impairment and blindness, despite only accounting for 10-20% of macular degeneration cases.10
The gold standard for diagnosis of neovascular macular degeneration remains fluorescein angiography.11 FA is a minimally invasive test that involves intravenous administration of dye in conjunction with fundus photography to allow dynamic evaluation of ocular blood flow, including blood leakage and pooling.11 On FA, CNV is seen as hyperfluorescence that increases in intensity and size over time as the fluorescein leaks from the neovascular membranes.11 FA patterns of CNV are classified as either “classic,” which shows well-demarcated lesions with early hyperfluorescence and clear leakage in later frames, or “occult,” which is characterized by a fibrovascular pigment epithelial detachment or ill-defined leakage from an undetermined source.12 In cases where fluorescein is blocked by subretinal hemorrhage, indocyanine green angiography can be useful in identifying and characterizing choroidal neovascular lesions.11 This patient demonstrated an occult pattern on FA consistent with a fibrovascular pigment epithelial detachment.
In addition to FA, spectral-domain OCT has emerged in recent years as an essential adjunctive test for diagnosing and monitoring non-neovascular and neovascular macular degeneration.13 Detailed cross-sectional imaging of retinal anatomy allows non-invasive visualization of detachments of the pigment epithelium and subretinal fluid due to choroidal neovascularization.12 OCT in this patient identified a pigment epithelial detachment with adjacent subretinal fluid.
There is currently no definitive treatment for non-neovascular macular degeneration; however, the Age-Related Eye Disease Study (AREDS) demonstrated that high levels of antioxidants (500 mg vitamin C, 400 IU vitamin E, 15 mg beta carotene, 80 mg zinc, 2 mg copper) reduced progression to advanced AMD by 25% at five years for patients with moderate non-neovascular macular degeneration.8-9 The AREDS2 expanded on these findings and substituted lutein and zeaxanthin (main components of macular pigment) for beta-carotene. Part of the reasoning for this substitution was that beta-carotene might increase the risk for lung cancer in patients who had a history of smoking.14 Supplementation with omega-3 fatty acids [docosahexaenoic acid (DHA) and its precursor eicosapentaenoic acid (EPA)] did not appear to slow progression of the condition.14 As such, patients with intermediate non-neovascular or neovascular macular degeneration should be counseled on supplementation with the AREDS2 formula multivitamin.
In recent years, the treatment for neovascular macular degeneration represents one of the most significant advances in eye care. Current treatment involves intravitreal injection of Food and Drug Administration-approved anti-VEGF agents, such as ranibizumab, aflibercept, and pegaptanib.11 Bevacizumab, an anti-VEGF medication approved for the treatment of colon cancer, is also currently used off-label to treat neovascular macular degeneration.10 Several clinical trials (MARINA, ANCHOR, HARBOR, CATT, VIEW1, VIEW2) have demonstrated maintenance or improvement in visual acuity in patients with neovascular macular degeneration receiving regular (usually monthly) treatments of intravitreal anti-VEGF therapy.15-19 Human clinical trials are currently investigating platelet-derived growth factor (PDGF) antagonists as a promising alternative or combination therapy for treatment of choroidal neovascularization.20 PDGF is triggered by retinal ischemia and promotes the cascade responsible for neovascular angiogenesis and, as such, inhibiting this factor represents an encouraging new therapeutic possibility for the treatment of choroidal nevovascularization.20 With continued advances in therapies such as anti-VEGF and anti-PDGF, vision can be preserved and even improved with prompt diagnosis and treatment of neovascular macular degeneration.
Smoking represents the only known modifiable risk factor for development and progression of macular degeneration.12 The AREDS showed the risk for development of neovascular macular degeneration was doubled in patients who had a history of smoking compared to patients who had never smoked. Additionally, the risk of developing any macular degeneration for both males and females was doubled in active smokers, according The Physicians’ Health Study and Nurses’ Health Study.21-22 As such, smoking cessation should be strongly encouraged for all patients with macular degeneration.
Conclusion
This case highlights a patient who presented for a routine glaucoma follow-up visit, but was found to incidentally have a CNVM from neovascular macular degeneration. It reflects the importance of a careful case history to determine if recent visual changes could be related to progression of ocular pathology. Finally, it underscores the need to be flexible as a clinician to deviate from one’s planned exam sequence to address the patient’s symptoms.
Acknowledgment
The authors would like to thank Lorne Yudcovitch, OD, MS, FAAO, for his helpful comments during the revision process for this manuscript.
References
- Mallick J, Devi L, Malik PK, Mallick J. Update on normal tension glaucoma. J Ophthalmic Vis Res. 2016;11(2):204-8.
- Jager RD, Mieler WF, Miller JW. Age-related macular degeneration. N Engl J Med. 2008 Jun12;358(24):2606-17.
- Mi XS, Yuan TF, So KF. The current research status of normal tension glaucoma. Interv Aging. 2014;16(9):1563-71.
- Francoz M, Fenolland JR, Giraud JM, et al. Reproducibility of macular ganglion cell-inner plexiform layer thickness measurement with cirrus HD-OCT in normal, hypertensive and glaucomatous eyes. Br J Ophthalmol. 2014;98:322-8.
- Yenice E, Şengün A, Soyugelen Demirok G, Turaçlı E. Ganglion cell complex thickness in nonexudative age-related macular degeneration. Eye (Lond). 2015;29:1076-80.
- Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008;19(2):85-8.
- Anderson DR; Normal Tension Glaucoma Study. Collaborative normal tension glaucoma study. Curr Opin Ophthalmol. 2003;14(2):86-90.
- Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol. 2001;119(10):1417-36.
- Age-Related Eye Disease Study Research Group. Risk factors associated with age-related macular degeneration. A case-control study in the age-related eye disease study: Age-Related Eye Disease Study Report Number 3. Ophthalmology. 2000;107:2224-2232.
- Tsilimbaris MK, López-Gálvez MI, Gallego-Pinazo R, Margaron P, Lambrou GN. Epidemiological and clinical baseline characteristics as predictive biomarkers of response to anti-VEGF treatment in patients with neovascular AMD. J Ophthalmol. 2016;2016:4367631.
- Chalam KV, Sambhav K. Optical coherence tomography angiography in Retinal Diseases. J Ophthalmic Vis Res. 2016;11(1):84-92.
- Yonekawa Y, Miller JW, Kim IK. Age-related macular degeneration: advances in management and diagnosis. J Clin Med. 2015 Feb 12;4(2):343-59.
- Health Quality Ontario. Optical coherence tomography for age-related macular degeneration and diabetic macular edema: an evidence-based analysis. Ont Health Technol Assess Ser. 2009;9(13):1-22.
- Age-Related Eye Disease Study 2 Research Group. Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the Age-Related Eye Disease Study 2 (AREDS2) randomized clinical trial. JAMA. 2013 May 15;309(19):2005-15.
- Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419-1431.
- Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57-65.e5.
- Ho AC, Busbee BG, Regillo CD, et al. Twenty-four-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2014;121(11):2181-2192.
- Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group, Maguire MG, Martin DF, Ying GS, et al. Five-year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: The Comparison of Age-Related Macular Degeneration Treatments Trials. Ophthalmology. 2016;123(8):1751-61.
- Heier JS, Brown DM, Chong V, et al., VIEW 1 and VIEW 2 Study Groups. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119:2537-48.
- Sadiq MA, Hanout M, Sarwar S, et al. Platelet derived growth factor inhibitors: a potential therapeutic approach for ocular neovascularization. Saudi J Ophthalmol. 2015;29:287-91.
- Christen WG, Glynn RJ, Manson JE, Ajani UA, Buring JE. A prospective study of cigarette smoking and risk of age-related macular degeneration in men. JAMA. 1996;276:1147-1151.
- Seddon JM, Willett WC, Speizer FE, Hankinson SE. A prospective study of cigarette smoking and age-related macular degeneration in women. JAMA. 1996;276:1141-1146.
- Optometric Clinical Practice Guideline: Care of the Patient with Open Angle Glaucoma (revised 2010) [Internet]. St. Louis, MO: American Optometric Association; c2011. Available from: https://www.aoa.org/documents/optometrists/CPG-9.pdf

