
PEER REVIEWED
Presumed Traumatic Partial Fourth Nerve Palsy
Hilary Gaiser OD, MS, Stacy Lyons OD, FAAO
Superior oblique palsies (SOPs) are frequently encountered in primary care optometry and can be either congenital or acquired. Primary care optometrists should be comfortable in their ability to diagnose, treat and co-manage cases of SOP. This teaching case report features a unique case of traumatic SOP that was diagnosed in a primary care setting and managed with Fresnel prism. This teaching case report will give third- and fourth-year optometry interns an overview of commonly performed clinical tests used to diagnose SOP, signs and symptoms of SOP, causes of acquired SOP, and management options available to the primary care optometrist. Additionally, the case will provide students an opportunity to fit Fresnel prism on practice glasses and perform Park’s three-step and double Maddox rod on their peers or practice patients.
Key Words: fourth nerve palsy, traumatic fourth nerve palsy, acquired fourth nerve palsy, Fresnel prism, CN IV palsy, trochlear nerve palsy, superior oblique palsy, SOP
Background
While the most common causes of superior oblique (SOP) palsy are associated with congenital abnormalities, trauma is a leading cause of acquired SOP, accounting for approximately 40% of acquired cases.1,2,4 Due to the longer pathway the fourth cranial nerve (CN IV) travels to reach the superior oblique muscle in the orbit, CN IV is more susceptible to damage due to trauma.3 While dependent on the severity of the trauma, most cases of traumatic SOP resolve spontaneously, either partially or completely, over a period of one to six months.4,5 Symptoms of traumatic SOP can be variable but are typically associated with the complaint of constant, vertical, diplopia that worsens in downgaze and that is associated with a recent history of head or ocular trauma. Patients may also report torsional (rotational) disturbances and may show a compensatory head tilt and chin tuck.6 It is important for the primary care optometrist to differentiate between cases of acquired and congenital SOP and rule out other causes of acquired palsies, such as vasculopathies, infection and tumors.7 This teaching case report presents a unique case of traumatic SOP and is suitable for third- and fourth-year optometry interns.
Case Description
Visit One
A 35-year-old Spanish speaking male patient (Patient J) presented to a community health center clinic with the chief concern of a “bloody and painful” right eye (OD). Case history was completed using phone interpretation services for visit one and all subsequent visits. The patient reported that 4 days prior he was hit with an elbow OD and that since being hit in the eye he had been experiencing constant, moderate, blurry vision in both eyes (OU) that was noticeably worse OD.
Patient J reported (5/10) ocular pain and had not tried anything for relief. The patient presented to the clinic without glasses, although he had been given an updated glasses prescription six months ago at his annual comprehensive eye exam: OD: – 1.75 – 1.00 x 152 and left eye (OS): -1.75 – 0.50 x 120, with a visual acuity (VA) of 20/20 OU at that visit. The patient denied flashes, floaters and diplopia.
The patient was an established patient of the health center and his comprehensive exam six months ago was negative for findings consistent with ocular trauma. Previous ocular history was unremarkable aside from two other incidents of previous ocular trauma; one incident involving hitting an eye on the handlebars of a bicycle and one incident of getting “wires in both eyes”. Patient J reported that both incidents had occurred 7 and 6 years ago respectively and that he had not sought medical attention after both incidents. Patient J’s medical history was unremarkable; he was not taking any medications and denied drug and environmental allergies. Patient J did report social drinking and smoking but denied recreational drug use.
With the patient’s previous glasses Rx on file from 6 months ago, the patient’s entering visual acuities were OD: 20/50, OS: 20/40 and OU: 20/40. Pinhole (PH) visual acuities were OD: no improvement and OS: 20/60. Confrontation fields, pupils and extraocular motilities were normal. Biomicroscopy showed moderate periorbital swelling, mild bruising of the right inferior eyelid, and a diffuse nasal subconjunctival hemorrhage OD. All other anterior segment findings were normal other than mildly hyperemic bilateral nasal pterygia: 3 mm OD and 1 mm OS, which was not encroaching on the visual axis. Intraocular pressures via Goldmann Applanation Tonometry (GAT), were 14 mm Hg OD and 11 mm Hg OS. Dilated fundus examination (DFE) was positive for syneresis OU, and no holes/tears/detachments were noted bilaterally. Due to the decreased VA, compared to previous exams and unremarkable findings on DFE, macular OCT was performed. The results of the macular OCT were reliable and normal foveal contour was noted OU. The patient was diagnosed with an acute subconjunctival hemorrhage secondary to ocular trauma OD and was given a prescription for Systane Ultra 1 gtt OD QID x 14 days. The decreased visual acuity OD was attributed to the ocular trauma but of unclear etiology OS. Patient J was scheduled for a 2-week follow-up appointment for VA check and repeat refraction. Gonioscopy was to be considered at the 2-week follow-up appointment.
Visit Two
Patient J presented for his 2-week follow-up appointment with the report of decreased ocular pain and resolution of the subconjunctival hemorrhage OD. However, he reported persistent, constant bilateral blurry vision with his glasses at distance and near. Patient J also reported new symptoms of diplopia. The patient reported constant binocular diplopia at distance and near. Patient J did not recall when he first noted the diplopia but reported that it had happened sometime after his initial visit to the health center for ocular trauma. For relief the patient had been closing one eye. When asked about other visual distortions e.g., twisting, the patient denied any symptoms. Additionally, Patient J denied any changes to his medical history.
Entering visual acuity with habitual glasses was OD: 20/30, OS: 20/40 and OU: 20/30 and confrontation fields, pupils and extraocular motilities were unremarkable. Interestingly, the patient did not report diplopia on EOMs. Repeat subjective refraction was identical to the results of refraction 6 months prior with no improvement in visual acuity. A preliminary binocular vision assessment was performed at near, using the Modified Thorington (MT) and prism neutralized cover test using the patient’s habitual correction. MT showed a 1 prism diopter (pd) exo and 10 pd right hyper. Similar to the findings found on prism neutralized cover test in central gaze (orthophoria horizontally and 8 pd constant right hypertropia).
Subjectively, the vertical deviation improved the most with an 8 pd base down (BD) OD loose prism (remaining 2 pd right hypertropia on MT) and the addition of more loose prism did not improve the diplopia. Further binocular vision testing was not performed at visit two due to the time constraints of the patient; ideally prism neutralized cover test in all positions of gaze and Park’s three-step (Park’s) would also have been performed.
Biomicroscopy was unremarkable OU, aside from the bilateral pterygia, and the subconjunctival hemorrhage, periorbital swelling and bruising of the eye and eyelid had fully resolved. Intraocular pressures via GAT were 10 mm Hg OD and OS. Macular OCT was repeated due to the continued decreased best corrected visual acuity (BCVA) 20/30 OD and 20/40 OS. The results of the macular OCT were reliable with normal foveal contour noted OU. Gonioscopy was considered, but deferred due to a variety of factors, including stable IOP, no changes to the anterior chamber appearance on slit lamp and the complaint of new onset diplopia requiring more urgent testing. Additionally, damage to the structures of the angle resulting in angle recession does not produce elevated IOP soon after ocular trauma23.
Patient J was tentatively diagnosed with a presumed SOP secondary to trauma of the CN IV and/or the superior oblique tendon. A 7 pd BD Fresnel prism was attached to the right lens of the patient’s glasses and the patient reported improvement but not full resolution of his symptoms of diplopia. Unfortunately, an 8 pd Fresnel prism was not available in the office. The patient was educated on the findings and treatment, including the potential for blurry vision from the Fresnel. Patient J was scheduled for a follow-up appointment in 1 week for further binocular vision testing and a potential referral to neurology was discussed with the patient.
Visit Three
The patient presented to his third visit with the continued concern of diplopia and constant, bilateral, blurry vision. At this visit the patient was able to better describe that the diplopia was vertical, and he denied horizontal diplopia or torsional disturbances. Patient J reported that he was compliant with the use of Fresnel prism and reported improvement but not total resolution of his symptoms of diplopia. The patient denied any changes to his medical history.
The patient’s entering distance visual acuity with his prescription in a trial frame was OD: 20/40, OS: 20/60 and OU: 20/40, which represented a VA improvement of one line OD and a decrease in VA of two lines OS from the patient’s initial visit. Confrontation fields, pupils and extraocular motilities were normal, and prism neutralized cover test confirmed the presence of a constant and comitant 6 pd right hypertropia, representing an improvement of 4 pd from visit three. Comitancy is defined as an angle of deviation that does not change in either eye or in different fields of gaze24 and a deviation difference of 5 pd in all gaze directions has been suggested as a threshold criterion for acute onset esotropia25, however literature is lacking concerning the magnitude of deviation difference that can still be considered comitant in cases of SOP. However, Modified Thorington testing revealed a deviation of 12 pd in all positions of gaze. Park’s prism neutralized cover test in primary, left and right gaze and left and right head tilt, was performed and findings were consistent with a SOP OD. See Table 1 for summary of cover test findings and Park’s visit three. It should be noted that the deviation was comitant, which is not a typical presentation of SOP.
Double Maddox rod testing was considered, but not performed as the patient did not report frank torsional disturbances. Had torsional disturbances been reported and Maddox rod performed, an excyclorotation response would have been consistent with a SOP, while a response of incyclorotation would be consistent with a skew deviation21.
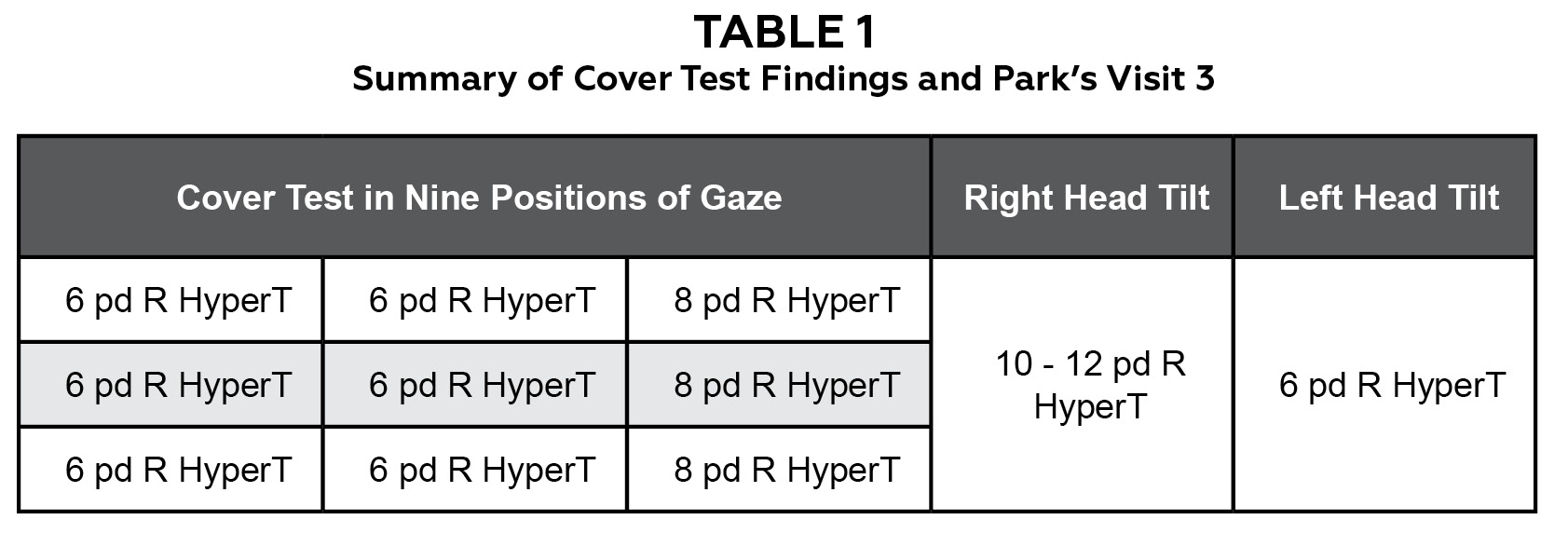
Table 1. Summary of Cover Test Findings and Park’s Visit 3. Click to enlarge
Biomicroscopy was positive for mild meibomian gland dysfunction, bilateral pterygia and reduced tear break-up time OU. The presumed diagnosis of traumatic SOP of visit two was further confirmed at visit three by Park’s. The decreased BCVA OD and OS was attributed to mild dry eye secondary to meibomian gland dysfunction OU, although the reduction of BCVA OD and OS was not considered to be consistent with the level of dry eye noted during biomicroscopy. The patient was referred to neurology for imaging and to confirm the diagnosis of SOP. Unfortunately, the earliest neurology appointment was not available for two months due to COVID-related access issues. Patient J was instructed to continue using the Fresnel prism, unchanged at this visit, and to begin aggressive lubrication with preservative free artificial tears (PFAT) QID OU and to return in 1 week for diplopia and dry eye follow-up.
Visit Four
Patient J presented to his fourth visit with reports of marked improvement in visual acuity OU with the use of PFAT QID OU. However, the patient’s symptoms of diplopia were unchanged from the previous visit. Additionally, there were no changes to his medical history. Patient J reported a new concern about the pterygia OU, which he thought had grown since getting hit in the eye.
The patient’s entering visual acuity, with his habitual prescription in a trial frame, was OD: 20/40 OD, OS: 20/30 and OU: 20/30; this represented a stable VA from the previous visit OD and an improvement in three lines VA OS. Confrontation fields, pupils and extraocular motilities were normal. Findings of Park’s and prism neutralized cover test are summarized below in Table 2. Modified Thorington testing revealed a comitant deviation of >12 pd in all positions of gaze.

Table 2. Summary of Cover Test Findings and Park’s Visit 4. Click to enlarge
Biomicroscopy findings indicated no growth of the patient’s bilateral pterygia from the patient’s initial visit and improvement in the tear film layer and meibomian gland dysfunction were noted OU. Gonioscopy, which had been deferred at previous visits, was performed to rule out potential angle recession due to trauma. The angle was open to ciliary body band (CBB) OU and no angle recession was noted.
Patient J was diagnosed with a stable traumatic SOP OD and decreased BCVA associated with mild dry eye OU. The patient was educated to continue using the Fresnel prism OD, unchanged from visit two, and to continue the use of PFAT QID OU. The patient was scheduled to return in 2 weeks for diplopia and dry eye follow-up.
Visit Five
On his fifth appointment, now 6 weeks after the initial ocular trauma, Patient J reported marked improvement in his symptoms of both blurry vision and diplopia. Patient J denied blurry vision at distance and near OD and OS and reported only trace, binocular, vertical diplopia with his glasses with Fresnel attached. Entering visual acuity, with the patient’s habitual prescription in a trial frame was OD: 20/30, OS: 20/20 and OU: 20/20, an improvement of one line VA OD and two lines VA OS from the previous visit. Confrontation fields, pupils and extraocular motilities were unremarkable. Prism neutralized cover test revealed a 3 pd R hypertropia in all positions of gaze, and MT revealed a 2 pd R hyper in all positions of gaze. This represented an improvement of 3 pd and 10 pd respectively. The Fresnel prism attached to the patient’s glasses was reduced from 7 pd to 3 pd BD OD and Patient J reported single vision with a slight blurring OD. The patient was diagnosed with a resolving, traumatic SOP and dry eye controlled with PFAT and was educated to continue using PFAT QID OU and the new Fresnel prism. The patient was scheduled to return in 2 weeks for dry eye and diplopia follow-up.
Visit Six
Unfortunately, Patient J missed his subsequent 2 week follow-up appointment and presented to the health center nearly two months after his fifth visit for his follow-up appointment. While initially scheduled for a neurology appointment 2 weeks prior to his sixth appointment, the patient stated he “forgot his appointment” and did not go. The patient reported full improvement in symptoms, other than mild blur created by the Fresnel prism still attached to the right lens of his glasses.
Visual acuity, with his prescription in a trial frame, was OD: 20/20, OS: 20/25 and OU: 20/20 and confrontation fields, pupils and extraocular motilities were unremarkable. Prism neutralized cover test was ortho in all positions of gaze. The patient was diagnosed with a resolved traumatic SOP and the 3 pd Fresnel prism was removed from the patient’s glasses. The patient was educated extensively on eye safety and was told to resume comprehensive eye exams as regularly scheduled.
Education Guidelines
This case is appropriate for third- and fourth-year optometry interns under the guidance of a facilitator. This can include but is not limited to clinical grand rounds, workshops, seminars and the traditional classroom. Students can be given the case details and discussion questions, either as individuals or in groups, and tasked with answering the questions with peer reviewed literature, either during the sessions or with answers brought to the session. During the session the facilitator should review the key concepts, discussion questions and assist students with fitting Fresnel prism to practice glasses and performing the Park’s and double Maddox rod tests on each other. Assessment of learning can be performed through grading of the discussion questions and participation in answering open ended questions, fitting of the Fresnel prism and performing Park’s and double Maddox rod tests.
Learning objectives
- Trauma is a common etiology of acquired SOP
- Optometrists play a key role in the diagnosis and management of acquired SOP
- Fresnel prisms can be utilized to manage transient diplopia until resolution of the acquired SOP occurs
- Patient education and frequent follow-up is a critical component of SOP management
- Optometric clinical tests, including prism neutralized cover test in all positions of gaze, double Maddox rod and Park’s are commonly used to diagnose SOP
Key concepts
At the conclusion of this case report, readers should be able to:
- Differentiate between congenital and acquired cases of SOP
- Articulate the various etiologies underlying SOP
- Perform relevant testing to diagnose and manage SOP
- Demonstrate proficiency in fitting Fresnel prisms to a pair of practice glasses
- Demonstrate proficiency in performing and interpreting findings of Park’s and prism measured cover test in all positions of gaze
- Understand when collaboration with other providers is warranted and when cases can be managed or co-managed by a primary care optometrist
- Understand how and when to perform the double Maddox rod test
Learning Assessment
Students should work in small groups with access to Fresnel prisms, practice glasses, double Maddox rod, prism bars and occluders. After reviewing the case and discussion questions, either individually or in groups, students should work to answer the discussion questions using peer-reviewed literature. Under the guidance of a facilitator, students should then practice the Park’s technique and double Maddox Rod on each other or a practice patient. Students can also work through the findings outlined in the case description of SOP. The facilitator also has the option for students to practice performing prism measured cover test in all positions of gaze, if it is deemed that students would benefit from extra practice of this technique. After completing the above assignments, students should practice fitting a Fresnel prism to practice glasses. The facilitator should review the students answers to the discussion questions, observe and give feedback on the Park’s and double Maddox rod procedures and assist students with questions pertaining to fitting of Fresnel prism.
Students should be shown examples of Fresnel prism in a variety of sizes, recommendations are to show a small, medium and large range of Fresnel. This can vary depending on the Fresnel prisms available to the facilitator. Review the orientation of the prisms and how to properly select the correction orientation. Other hypothetical situations e.g., horizontal deviations, can also be assigned to students for them to determine the correct orientation of Fresnel. Students can then trace, cut and place the Fresnel prism to their own glasses, glasses of classmates or practice glasses.
Discussion questions
- What examination techniques are utilized to diagnose SOP?
- What specific findings are used to differentiate cases of SOP from other cranial nerve palsies?
- What is the importance of subjective and objective findings for complaints of diplopia?
- How might the management of the patient have changed had decreased BCVA of unknown etiology not been present?
- How might the management of the patient have changed had symptoms consistent with cyclodeviation been present?
- What is the repeatability of estimated cover test vs. prism measured cover test and discuss the importance of prism measured cover test when multiple follow-up visits are needed.
- How did the presentation of Patient J differ from more typical cases of traumatic SOP?
Discussion
Trauma is a common cause of acquired SOP.1,2 Depending on the study, the prevalence of acquired SOP is estimated to be approximately 40% traumatic, 30% idiopathic, 20% due to vascular infarct and 10% due to tumor or aneurysm.4 When the etiology is of traumatic origin, it is usually the result of closed head trauma. Occasionally direct trauma to the superior oblique tendon can also result in unilateral SOP as in the case of Patient J.8 Since a high number of traumatic SOP cases fail to show abnormal findings on imaging,3,8 determination of the exact etiology can be difficult. However, most cases of traumatic SOP resolve spontaneously over a period of weeks to 6 months. If diplopia persists longer than 6 months, surgery may be required to realign the eyes.4,5
Understanding the CN IV Nerve and the Superior Oblique Muscle
The nucleus of CN IV is located in the dorsal midbrain, ventrolateral to the cerebral aqueduct. The nerve fascicle of the nucleus courses posteroinferiorly around the aqueduct to decussate (cross) in the anterior medullary vellum just caudal (towards the tail) of the inferior colliculus. CN IV then emerges from the dorsal surface of the lower midbrain below the inferior colliculus and near the tentorium. CN IV then passes between the superior cerebellar and posterior cerebral arteries to leave the posterior fossa and enters the cavernous sinus, along the lateral aspect of the clivus below the petroclinoid ligament.7 Note CN IV is the only nerve to decussate before reaching its target extraocular muscle and has the longest pathway of all the cranial nerves.9
After entering the subarachnoid space, CN IV then travels around the brainstem and enters the cavernous sinus. While in the cavernous sinus, CNIV is located along the lateral wall and lies below the oculomotor and above the ophthalmic division of the trigeminal nerve with which it shares a connective tissue sheath. After leaving the cavernous sinus CN IV enters the superior orbital fissure to innervate the superior oblique muscle. This is a lengthy pathway for the thin CN IV and injury can occur anywhere from midbrain to orbit, including direct trauma to the superior oblique tendon.9, 7,10,11
The primary action of the superior oblique muscle is intorsion, the secondary action depression, and the tertiary action is abduction.7 Contrecoup forces encountered during a traumatic event can compress the CN IV against the rigid tentorium, which is adjacent to the nerve for a significant portion of its course9,11.
Localization of Superior Oblique Palsies
A lesion of the CN IV nucleus may result in paresis of the contralateral superior oblique muscle. Non-traumatic causes of unilateral or bilateral SOP may include but are not limited to, nuclear aplasia, mesencephalic stroke, tumor, arteriovenous malformation and demyelinating diseases. Mesencephalic lesions most typically present with additional damage to neighboring structures, causing additional findings, which may assist in the determination of etiology e.g, disturbances in consciousness, gait ataxia, hemiparesis, oculomotor disturbances and visual field defects.22 Unilateral SOP may also present with an ipsilateral Horner’s Syndrome (contralateral CN IV nucleus lesion) if the lesion occurs before decussation in the anterior medullary velum and adjacent sympathetic fibers. Ischemic neuropathy from diabetes or other vascular causes can occur anywhere along CN IV. A summary of ocular signs and the affected structures can be found in Table 3. Please note this table is ocularly focused, other signs such as hemiparesis, may also be noted but the scope is outside this teaching case report.7 Inflammatory causes such as meningitis, cavernous sinus mucormycosis and cysterical cysts of the aqueduct may also be implicated in SOP.19
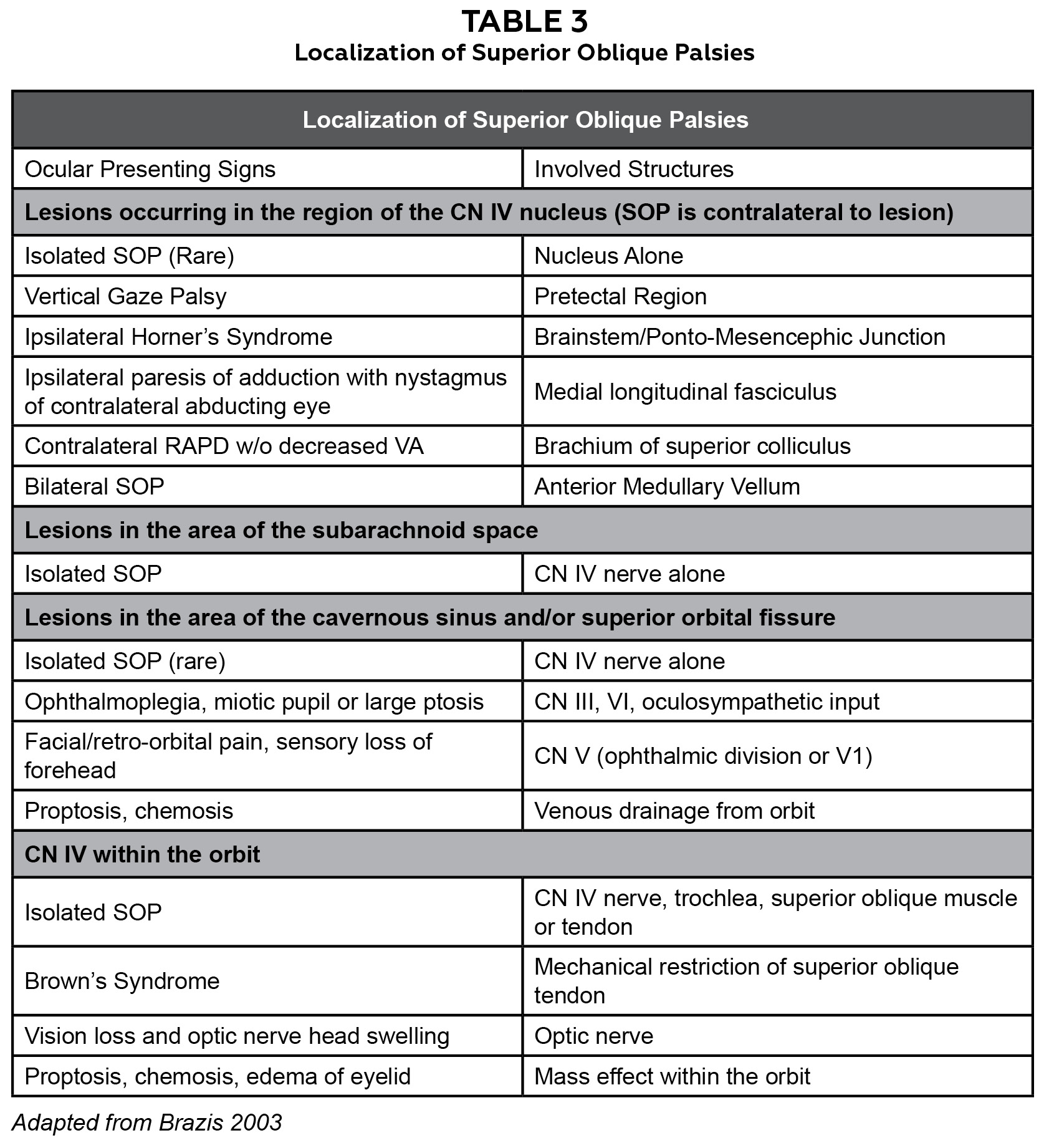
Table 3. Localization of Superior Oblique Palsies. Click to enlarge
Congenital vs Acquired Superior Oblique Palsy
Determination of acquired vs. congenital SOP, can be aided by a thorough case history. Typically acquired cases of SOP present with symptoms of diplopia while in congenital cases the complaint of diplopia is commonly absent.8 A compensatory head tilt away from the affected side occurs in approximately 70% of patients with congenital and acquired SOP and patient photos may be helpful in distinguishing a new compensatory head tilt from a longstanding head tilt. This compensatory head tilt allows the patient to fuse the double images into a single image. Some patients, approximately 3%, develop a paradoxical head tilt towards the side of the lesion. This may aid in suppression due to the wider separation of the images.10,12 In the case of Patient J, no compensatory head tilt was noted throughout the duration of the SOP. Additionally subjective complaints of torsional disturbances, while absent in this case, are more commonly found in acquired vs. congenital cases of SOP.16 Greater fusional amplitudes are also usually found in patients with congenital SOP than in patients with acquired palsies.20
Diagnosis of Traumatic Superior Oblique Palsy
Unilateral traumatic SOP typically presents with a noncomitant hypertropia that worsens in nasal gaze of the involved eye and when the head is tilted towards the affected side.12 Patient J was atypical in that the vertical deviation was noted to be comitant. However, since the deviation followed a pattern consistent with an SOP on Park’s, he was diagnosed with a presumed traumatic SOP and/or damage to the superior oblique tendon.
The Park’s test is a common clinical test performed in patients presenting with vertical diplopia to determine the affected muscle. The test is estimated to have a sensitivity of 70-75% in diagnosing unilateral SOP.13,14 Prism-measured alternate cover test is currently the gold standard for objective determination of the magnitude, laterality, direction and frequency of vertical deviations associated with SOP. The Modified Thorington test could also be selected to measure the subjective deviation of the patient due to the test having the highest interobserver repeatability of tests of ocular deviation.15
As the primary action of the superior oblique muscle is intorsion, subjective torsional disturbances of the visual field are often reported and are more common in cases of acquired SOP.16 The double Maddox rod test, two cylinders, one in each eye, oriented to produce two horizontal lines, can be used to assess subjective torsional disturbances while fundus photography or indirect ophthalmoscopy are objective techniques for determining torsional disturbances. As neither frank subjective torsional disturbances were not reported by Patient J nor a noncomitant deviation found, torsional testing was not performed.16
Patients with minor damage to CN IV and related structures, typically present with the complaint of constant blurry vision despite having normal visual acuities. This is likely due to the subjective observation of mild vertical diplopia. Patients with more severe damage to CN IV may report diplopia and torsional disturbances of the visual fields. Pain is atypical in both cases.18 Complicating the case of Patient J was the lingering decrease in BCVA OU, including the eye without trauma, over several follow-up visits. Although the measured decrease in BCVA was larger than what is typically observed in patients with dry eye, BCVA did have marked improvement with the aggressive use of preservative-free artificial tears and a diagnosis of dry eye was determined to be the likely cause of the bilateral decreased BCVA. Correlation of visual acuity and other determinants of visual function e.g., contrast sensitivity with severity of dry eye, can be variable and are not always predictable.17
Management of Superior Oblique Palsies
Spontaneous resolution of acquired SOP occurs in approximately 82.6% of cases with 52.2% of patients experiencing complete recovery.19 While it is recommended that trauma related SOP undergo an MRI or CT scan of the head to dismiss the possibility of traumatic hemorrhage,10 our patient had resolved fully before his scheduled appointment with neurology. Additionally, Patient J did not report a history of head trauma but rather blunt force trauma OD only and did not present with any other neurological findings.
Since spontaneous resolution of SOP occurs in the majority of cases, it is recommended to delay prescribing permanent prism for 3-6 months. Fresnel prism, a form of temporary prism, is a good option for patients as they allow for the power of the prism to be changed frequently while helping the patient to attain single vision. The drawback of Fresnel prism is that it degrades the visual acuity, contrast and cosmesis due to the grooves of the prism.
Fresnel prism can be used for larger deviations (up to 30 pd). In both cases of temporary and permanent prism, the power needed to correct vertical diplopia can vary between congenital and acquired cases. In a study by Tamhankar et. al., patients with congenital SOP were given on average prismatic correction equal to 73% of the deviation measured in primary gaze, while those with acquired palsy were given prism almost equal to their deviation. This is most likely due to greater fusional amplitudes found in congenital SOP patients. Greater fusional amplitudes can also lead to higher success rates with prism correction in patients with congenital SOP, 92.8% (95% CI: 84%–97%) versus 86% (95% CI: 60%–96%) in patients with acquired SOP.20 Alternative treatments consist of patching and surgery. A surgical consult is typically recommended if diplopia persists longer than 6 months and typically requires resection of the inferior oblique muscle.5
Conclusion
Patient J presented with a unique case of traumatic SOP in several aspects of presentation including, delayed onset of diplopia, comitancy in all positions of gaze, lack of torsional disturbance complaints, and lack of chin tuck or head tilt. This may be due to bruising of the superior oblique tendon rather than frank trauma to CN IV, however cases of acquired SOP can also have a wide range of presentations and the patient’s findings formed a pattern that were consistent with SOP. Unfortunately, the results of imaging were not available as Patient J missed his appointment with neurology. Literature on isolated superior oblique tendon bruising as a cause of traumatic SOP is currently lacking so this case report presents a unique perspective on acquired SOP.6
Summary
SOPs (congenital or acquired) are frequently encountered in optometric practice and primary care optometrists should be comfortable in their ability to diagnose, treat and co-manage cases of SOP. Ocular trauma is a common cause of SOP implicated in 40% of acquired cases of SOP. Occasionally direct trauma to the superior oblique tendon can also result in unilateral SOP. Since a high number of traumatic SOP cases fail to show abnormal findings on imaging,3,8 determination of exact etiology can be complicated. However, most cases of traumatic SOP resolve spontaneously over a period of weeks to 6 months. If diplopia persists longer than 6 months, surgery may be required to realign the eyes.
References
-
- Von Noorden G, Murray E, Wong S. Superior Oblique Paralysis: A Review of 270 Cases. Arch Ophthalmol. 1986;104(12):1771-1776. doi:10.1001/archopht.1986.01050240045037
- Dosunmu EO, Hatt SR, Leske DA, Hodge DO, Holmes JM. Incidence and Etiology of Presumed Fourth Cranial Nerve Palsy: A Population-based Study. Am J Ophthalmol. 2018;185:110-114. doi:10.1016/j.ajo.2017.10.019
- Tago M, Hisata Y, Hirata R, Sakaguchi M, Katsuki NE, Yamashita SI. Traumatic bilateral fourth nerve palsy: Double vision induced by downward gaze after head injury [published correction appears in J Gen Fam Med. 2020 Nov 25;21(6):296]. J Gen Fam Med. 2020;21(4):155-156. Published 2020 Mar 11. doi:10.1002/jgf2.310
- Stiller-Ostrowski JL. Fourth cranial nerve palsy in a collegiate lacrosse player: a case report. J Athl Train. 2010;45(4):407-410. doi:10.4085/1062-6050-45.4.407
- Mitchell PR, Parks MM. Surgery of bilateral superior oblique palsy. Ophthalmology. 1982;89(5):484-488. doi:10.1016/s0161-6420(82)34765-x
- Ayse Gul Kocak ALTINTAS. Trochlear Nerve Palsy: A Review of Etiology, Incidence, Diagnostic Methods, and Treatment Alternatives. Arch Neurol & Neurosci. 7(4): 2020. ANN.MS.ID.000666. doi:10.33552/ANN.2020.07.000666
- Brazis Paul W. Trochlear Nerve (Cranial Nerve IV), Editor(s): Michael J. Aminoff, Robert B. Daroff, Encyclopedia of the Neurological Sciences, Academic Press, 2003, Pages 570-572.
- Yang HK, Kim JH, Hwang JM. Congenital superior oblique palsy and trochlear nerve absence: a clinical and radiological study. Ophthalmology. 2012;119(1):170–177. doi:10.1016/j.optha.2011.06.038
- Martin J. Neuroanatomy Text and Atlas. United States. McGraw-Hill; 2020.
- Brazis PW. Isolated palsies of cranial nerves III, IV, and VI. Semin Neurol. 2009;29(1):14–28. doi:10.1055/s-0028-1124019
- Moore KL, Dalley AF. Clinically Oriented Anatomy. Philadelphia, PA: Lippincott Williams & Wilkins; 1999.
- Brazis PW. Palsies of the trochlear nerve: diagnosis and localization. Recent concepts. Mayo Clin Proc. 1993;68(5):501–509. doi:10.1016/s0025-6196(12)60201-8
- Manchandia AM, Demer JL. Sensitivity of the three-step test in diagnosis of superior oblique palsy. J AAPOS. 2014;18(6):567-571. doi:10.1016/j.jaapos.2014.08.007
- Lee JE, Yang HK, Kim JH, Hwang JM. Diagnostic Utility of the Three-Step Test According to the Presence of the Trochlear Nerve in Superior Oblique Palsy. J Clin Neurol. 2018;14(1):66-72. doi:10.3988/jcn.2018.14.1.66
- Cebrian JL, Antona B, Barrio A, Gonzalez E, Gutierrez A, Sanchez I. Repeatability of the Modified Thorington Card Used to Measure Far Heterophoria. Optometry and Vision Science. 2014; 91 (7): 786-792. doi:10.1097/OPX.0000000000000297
- Khanam S, Sood G. Trochlear Nerve Palsy. [Updated 2022 Mar 8]. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. Available from: https://www.statpearls.com/point-of-care/30629
- Keane JR. Fourth nerve palsy: historical review and study of 215 inpatients. Neurology. 1993;43(12):2439-2443.
- Szczotka-Flynn LB, Maguire MG, Ying GS, Lin MC, Bunya VY, Dana R, Asbell PA, & Dry Eye Assessment and Management (DREAM) Study Research Group (2019). Impact of Dry Eye on Visual Acuity and Contrast Sensitivity: Dry Eye Assessment and Management Study. Optom Vis Sci, 96(6), 387–396. doi:10.1097/OPX.0000000000001387
- Park UC, Kim SJ, Hwang JM, Yu YS. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye (Lond). 2008;22(5):691-696. doi:10.1038/sj.eye.6702720
- Tamhankar MA, Ying G, Volpe NJ. Success of Prisms in the Management of Diplopia Due to Fourth Nerve Palsy. J Neuroophthalmol. 2011; 31 (3): 206-209. doi:10.1097/WNO.0b013e318211daa9
- Wong AM. Understanding skew deviation and a new clinical test to differentiate it from trochlear nerve palsy. J AAPOS. 2010 Feb;14(1):61-7 doi:10.1016/j.jaapos.2009.11.019. PMID: 20227626; PMCID: PMC5154745.
- Kumral E, Bayulkem G, Akyol A, Yunten N, Sirin H, Sagduyu A. Mesencephalic and associated posterior circulation infarcts. Stroke. 2002;33(9):2224-2231. doi:10.1161/01.str.0000027438.93029.87
- Salmon JF, Mermoud A, Ivey A, Swanevelder SA, Hoffman M. The detection of post-traumatic angle recession by gonioscopy in a population-based glaucoma survey. Ophthalmol. 1994 Nov. doi:10.1016/s0161-6420(94)31091-8
- Caloroso E and Rouse M. Clinical Management of Strabismus. Butterworth – Heinemann. 1993.
- Zhou Y, Ling L, Wang X, Jiang C, Wen W, Zhau, C. Augmented – Dose Unilateral Recession – Resection Procedure in Acute Acquired Comitant Esotropia. Opthalmol. 2022 Dec 23. doi:10.1016/j.optha.2022.12.019

