
PEER REVIEWED
Using Strabismus Simulation Prismatic Glasses to Teach Cover Testing in Optometric Clinical Education
Yutaka Maki, OD, MS, FCOVD, Narges Kasraie, OD, FAAO, Diplomate of ABO, Allison Cronin, OD, FAAO, Allan McCleary, OD, Srihari Narayanan, OD, PhD, FAAO, Sandra Fortenberry, OD, FAAO
Abstract
Background: To evaluate the effectiveness of strabismus simulation using prismatic glasses to teach the cover test in a preclinical optometry course.
Method: Forty-seven first year students were divided into two groups and taught cover test with and without the strabismus simulation prism glasses. Pre- and post-cover test assessments were given to evaluate each group’s learning gain.
Results: The control group’s average pre and post assessment grades were 55.80 and 72.46 (P=0.096), respectively while these of the experimental group were 59.03 and 89.58 (P<0.01), respectively.
Conclusion: The strabismus simulation prism glasses were found to be an effective tool in teaching cover test.
Keywords
Background
There are many elements of a comprehensive eye exam, each of which requires significant time, hard work and practice to learn. These elements, which include a thorough case history, initial entrance testing, refractive status determination, functional vision assessments, and ocular health evaluations, are taught at the University of the Incarnate Word Rosenberg School of Optometry over the course of four semesters in a series of pre-clinical courses and labs. The students in these “clinical optometry” courses spend most of their time learning the techniques from their attending doctors and, in turn, practicing the skills on their classmates. Before students can provide comprehensive eye care to patients in clinics, they must first demonstrate proficiency to the instructors in performing the techniques on each other. In the authors’ opinion, while many exam elements can be successfully learned through practice on any individual, certain skills, such as the cover test, are very difficult to master unless they are performed on many people with abnormal findings.
The cover test is an objective test13 designed to both identify and quantify the presence of an ocular misalignment, which is any “deviation of the line of sight from those directions necessary for bifoveal fixation.”13 An ocular misalignment is considered a phoria when both visual axes are aligned under binocular conditions and a tropia when both visual axes are not aligned under binocular conditions.14 A unilateral cover test (UCT), which includes observing the movement of the fixating eye when the other eye is first covered13, is designed to identify a strabismus (tropia or eye turn) and its component directions.13 An alternating cover test (ACT) includes alternating occlusion between the two eyes and holding occlusion in place for 2-3 seconds.13 The eye which was just uncovered is observed.13 The ACT is performed to determine both the direction and magnitude of a phoria or tropia.14 The ACT is not able to differentiate a phoria from a tropia.14
The simultaneous prism and cover test (SPCT) can also be utilized to measure the associated magnitude of the deviation of a strabismus.15 However, because many students have normal ocular postures, students often struggle to identify a larger phoria or strabismus. Further, because these students do not have the necessary experience with abnormal postures, measurement outcomes are likely to be impacted.1 Cover test findings are crucial in both the identification and management of phorias and strabismus. As phorias and strabismus can sometimes have a pathological origin, accuracy in performing cover test is crucial. Releasing a correct glasses prescription, referring for strabismus surgery, referring for vision therapy, or even ordering neuro-imaging hinge on a properly performed cover test.2
The educational experience and clinic readiness of the students can be enhanced if the students can experience ocular abnormalities through simulation early in their optometric education.3-7,9-12 There have been many attempts to create such clinical simulations using various techniques and technologies, and such simulations generally provide a greater understanding of ocular abnormalities and benefit students’ learning. Examples include simulations in color vision, visual impairment, strabismus and other conditions.3-7,9-12 While all these methods have been shown to be beneficial in aiding student learning, there is a cost associated with acquiring the equipment to achieve the necessary simulated conditions. The purpose of this prospective parallel study is to investigate the effect of custom-made prism glasses, designed to simulate strabismus, on the students’ ability to interpret the cover test without SPCT in a second semester first-year optometry lab.
Methods
Forty-seven optometry students (23 in the control group; 24 in the experimental group) who were registered in the second semester first-year clinical optometry course at the UIW Rosenberg School of Optometry participated in this prospective parallel study. This study was approved by the UIW Institutional Review Board. Informed Consent was obtained from all participants. The participants learned cover test skills in the previous first semester first-year clinical optometry course and passed the requirements of that course.
The participants were initially instructed to take an online cover test assessment which consisted of six multiple choice questions asking to evaluate and diagnose a series of different ocular alignments by watching animated cover test videos. The questions tested three lateral and three vertical deviations, and all questions were randomized. The animated cover test videos were created by the first author using PowerPoint and converted into an MP4 file. The software utilized to conduct the quiz was ExamSoft (Dallas, TX). The students were not given any feedback on their quiz performance. The students were then instructed to take a survey following the quiz regarding their subjective opinions on their understanding of cover test and interpretation of results (Table 1). Canvas (Salt Lake City, UT) learning management system (LMS) was utilized as the platform to conduct the online survey. After the prelab quiz and survey, a 15-minute lecture was given to review the basic concept of phorias and tropias.

Table 1: Survey Questions. Click to enlarge
After the mini-lecture, half of the students were then assigned the role of “patients” while the other half were assigned the role of “student doctors.” Each student doctor performed a cover test on every student from the “patient” group, and then the roles were switched. In this manner, every participant examined a minimum of 11 different patients, with a maximum of 12 different patients. A time duration of 3 minutes was allotted for each examination. Students were instructed to perform distance cover test and document the observed ocular alignment at every station. They had to determine if a phoria or a tropia was present, identify the deviating eye and interpret the direction of the deviation (ortho/eso/exo/hyper/hypo) through UCT and ACT. Students were not required to determine the magnitude of the deviation through SPCT. Three optometry professors and two third-year optometry student teaching assistants were utilized to offer consultation to ensure that the participants were performing cover test and interpreting results correctly. Both groups were instructed to seek help if they had questions.
After the cover test skills were performed, the laboratory concluded with another online cover test assessment using ExamSoft software. Although different questions were used in the post-lab quiz, the format was kept the same (six randomized multiple choice questions with three lateral and three vertical deviations). Feedback was not provided for their quiz performance. The participants were then instructed to complete a final survey using the Canvas LMS, to rate their subjective opinions on their understanding of cover test and interpretation of results. Questions were identical for pre- and post-surveys. Depending on their response, a score of 1 through 5 was given to reflect their subjective confidence level (Table 1).
Assignments to the experimental or control group were established by the students’ regularly scheduled laboratory day. The laboratories were administered on separate days and the students were instructed to report to their scheduled laboratory day without knowing if they would be a part of either the experimental or control group. The method we used in the experimental and control groups were identical except that each “patient” in the experimental group wore prismatic glasses to simulate vertical or horizontal strabismus, whereas no simulated strabismus glasses were used in the control group. The experimental group was instructed to wear contact lenses if they needed refractive correction so that they could wear prism glasses without issues.
The prism glasses were designed to simulate constant monocular horizontal or vertical strabismus. 6 to 10D prism was prescribed in each eye to induce diplopia. In addition, +4.00 to +5.00DS or Spherocylinder lens was prescribed in one of the eyes to degrade the visual acuity, simulating an amblyopic eye (See Table 2 for detail). A penlight was used as the fixating target. A patient wearing the strabismus simulation glasses was instructed to always choose to look at the clearer target of the two unless only one target was seen due to occlusion.

Table 2: Details of prismatic glasses. Click to enlarge
Results
As a class, 264 and 288 cover tests were performed in the control and experimental groups, respectively. In the control group, all examinations revealed phoric ocular posture. In the experimental group, the majority of patients manifested strabismus. Some patients’ ocular deviation changed from phoria to tropia over time most likely due to fatigue and prolonged occlusions. (Figure 1)

Figure 1: Cover test findings in Control and Experimental Groups Click to enlarge
The control group’s average pre- and post-cover test assessment grades were 55.80 and 72.46 (P=0.096), respectively, out of 100 points. The experimental group’s average pre- and post-assessment grades were 59.03 and 89.58 (P<0.01), respectively. Thus, the control and experimental groups improved their assessment grades by 29.87% and 51.76%, respectively (Figures 2A and 2B). The rate of improvement in the control and experimental groups were 16.67 and 30.56 points (P=0.15), respectively. There was no statistically significant difference in the average pre cover test assessment grades between the control and experimental groups (P = 0.74).
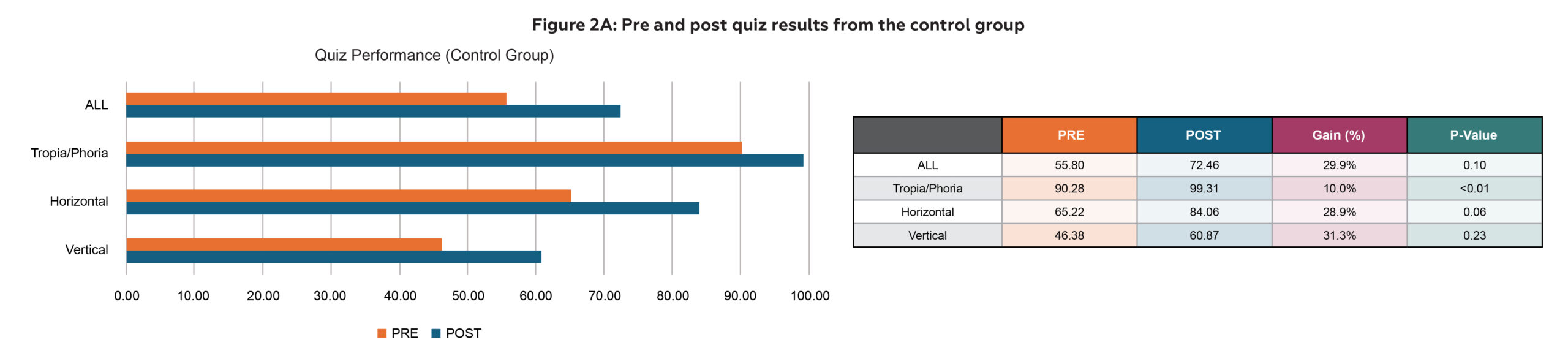
Figure 2A: Pre and post quiz results from the control group Click to enlarge
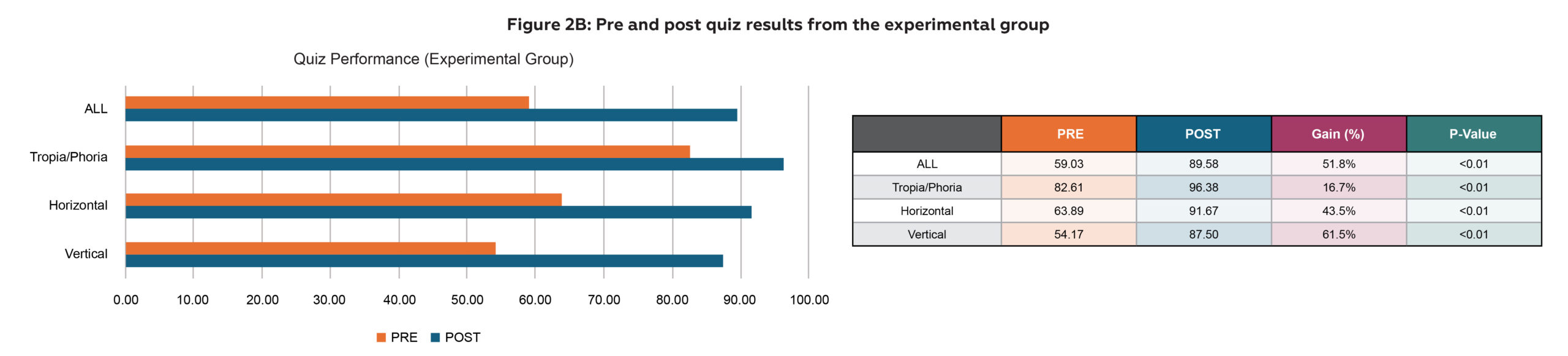
Figure 2B: Pre and post quiz results from the experimental group Click to enlarge
Their performance was further analyzed under three different learning objectives, which were also reflected in the lab survey: (1) ability to differentiate tropia vs. phoria, (2) ability to accurately evaluate horizontal deviations, (3) ability to accurately evaluate vertical deviations. For the first learning objective, each group improved their performance with statistical significance (P<0.01 each). For the second learning objective, the improvement seen in the control group was not statistically significant (P=0.06), while it was in the experimental group (P<0.01). For the third learning objective, the improvement seen in the control group was not statistically significant (P=0.23), while it was in the experimental group (P<0.01). Also, the greatest improvement was observed in their ability to accurately evaluate vertical deviations in the experimental group with a 61.5% gain (Figures 2A and 2B).
Some similar patterns were seen when survey results were analyzed. The control group’s overall pre- and post-survey results were 3.73 and 4.33 (P<0.01), respectively out of 5 points. The experimental group’s overall pre- and post-survey results were 3.69 and 4.67 (P<0.01), respectively. The control and experimental groups improved their survey results by 16.32% and 26.34%, respectively (Figures 3A and 3B). The rate of improvement in the control and experimental groups were 0.61 and 0.97 points (P=0.11), respectively. There was no statistically significant difference in the pre survey results between the control and the experimental groups (P = 0.86).
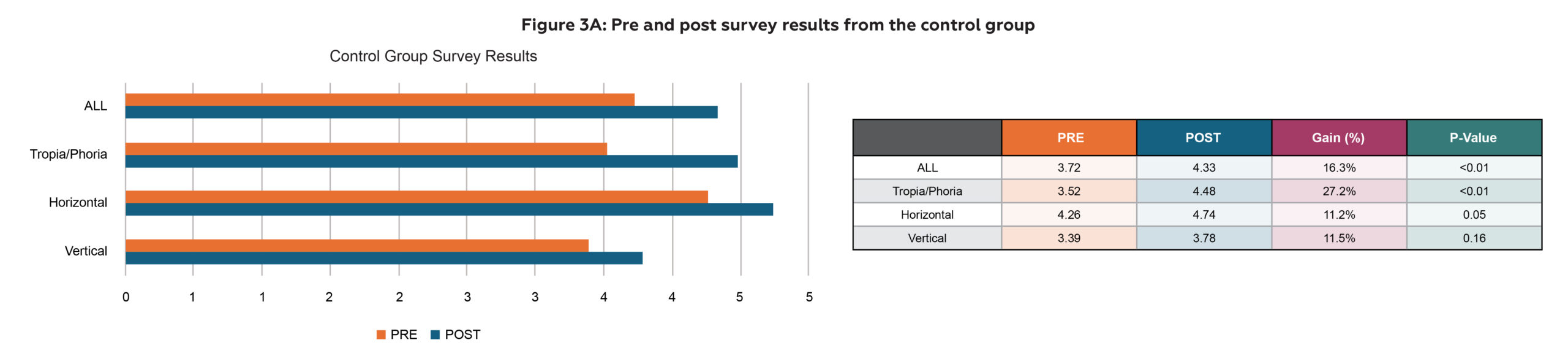
Figure 3A: Pre and post survey results from the control group Click to enlarge
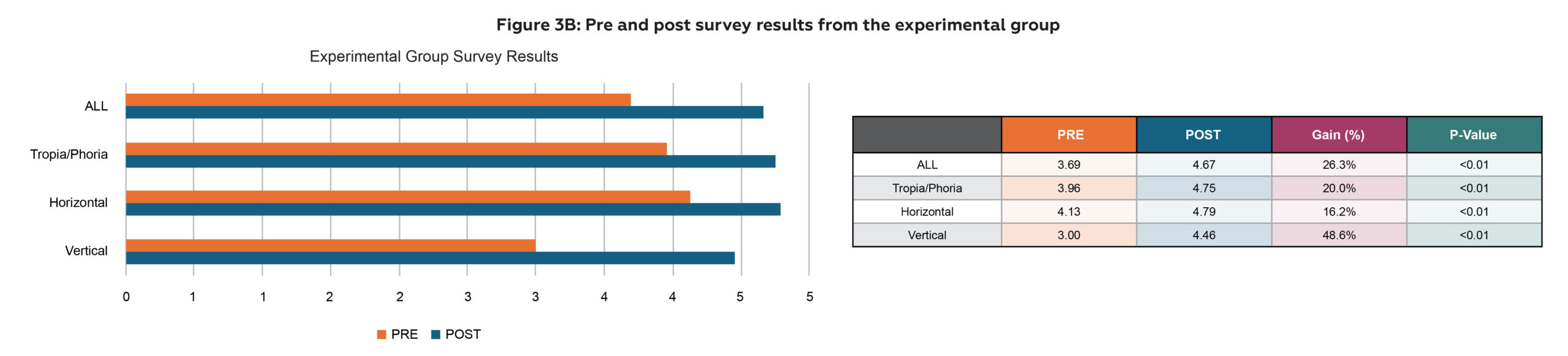
Figure 3B: Pre and post survey results from the experimental group Click to enlarge
Analysis of the survey results based on each question showed a similar pattern as seen in cover test assessment results; while there was no statistically significant positive change in their confidence level in evaluation of horizontal or vertical deviations in the control group (P=0.05 and P=0.16 respectively), there was statistically significant improvement in the experimental group (P<0.01 each).
Discussion
The traditional method of teaching cover test stands deficient at helping some students master this clinical skill prior to encountering strabismic patients in clinic which starts in the third year of the program. It remains true that under the current academic paradigm, students gain a rudimentary appreciation for diagnosing strabismus. However, when such practice is upon non-strabismic eyes predominantly, some students garner a limited opportunity to genuinely master cover test, or even gain the required confidence before seeing real strabismic patients.
In this study, the experimental group was exposed to various manifestations of strabismus through the simulation glasses and showed a greater gain in their interpretation and evaluation of cover test findings based on pre and post quizzes. While the control group also showed an improvement in their assessment performance, they were not exposed to a single patient with strabismus, and their improvement was smaller compared to the experimental group and not statistically significant. This non-statistically significant improvement may be explained by the fact that the subjects had already been previously exposed to traditional lab teaching and experiences. Thus, reviewing cover tests under the same conditions had no significant impact on them mastering the technique further under the same teaching conditions. Perhaps the gain we observed in the control group was the skills and knowledge that they had slowly forgotten since the previous semester.
Although the experimental group demonstrated a higher rate of improvement in cover test assessments and surveys, there was no statistically significant difference between the two groups. This can be explained since some students scored 100% on the pre assessment and/or survey, there was no measurable further improvement. This led to high variability in the rate of improvement especially in the experimental group (Figures 4A and 4B). This limitation may be addressed if this study is done earlier in the curriculum so that the rate of improvement is more measurable.

Figure 4A: Control group’s rate of improvement (ROI) measured in cover test assessments. Click to enlarge

Figure 4B: Experimental group’s rate of improvement (ROI) measured in cover test assessments. Click to enlarge
Based on our findings, using strabismic simulating glasses can enhance diagnostic training and improve students’ accuracy to diagnose strabismic eye abnormalities. The analysis of the participants’ pre- and post-cover test results revealed that the experimental groups’ cover test performance improved after one session of training with strabismic simulation glasses compared to the control group’s cover test performance. Students’ confidence levels were also found to be higher in the experimental group, where they worked with patients wearing the simulation glasses which provided them with an opportunity to observe and practice performing cover test on strabismic-looking eyes.
The greatest strength of the strabismus simulating glasses was teaching students the accurate evaluation of vertical deviations. There was a distinct gap in the achievement gain between the two groups when observing the mastery level of vertical deviation (31.3% vs 61.5%). Similar results were seen in their confidence level based on the surveys (11.5% vs 48.6%). These results indicate how students’ limited exposure to vertical deviation can adversely affect their clinical confidence and ability to diagnose this type of misalignment. However, the experimental group showed significant improvement in their clinical skills and confidence after using the simulation glasses. This shows the value of exposing students to abnormal clinical findings to facilitate their learning.
The authors noticed a greater level of engagement among the students in the experimental group, which was deemed to be a positive effect of simulation glasses. For most of the students, it was their first time seeing strabismic eyes. Also, many students found it fascinating to see the familiar eyes of their peers turning into strabismus. There were many exclamations of surprise and excitement during the lab. The authors also noticed that the experimental group took more opportunity to ask questions due to the complex nature of the cases. However, the students were not given extra assistance intentionally during the actual cover test procedure in each group.
In addition, the simulation glasses provided an opportunity for students to experience cover test from the perspective of a strabismus patient. One of the challenges instructors encounter when teaching cover test is how quickly students want to move the occluder. Sometimes they move it so fast that they do not give a patient sufficient time to fixate with the amblyopic eye when the dominant eye is occluded. Although this issue was witnessed by some students in our labs, it also allowed students to experience as a strabismus patient how difficult it can be to re-fixate on a blurry target when only a split second was given.
Our results show that the strabismus simulation glasses are a great additive teaching tool with respect to cover test instruction. This low-tech teaching device has been proven to serve as a supplemental apparatus to help improve clinical performance by optometry students.
Conclusion
In conclusion, based on the improved performance of the experimental group in this study, the strabismus simulation glasses were found to be an effective and valuable additional tool in teaching cover test to optometry students and should be utilized as a key component in cover test basic training.
References
Yutaka Maki, OD, MS, FCOVD, is an Associate Dean of Academic Affairs at the University of Texas Rio Grande Valley School of Optometry. His didactic responsibilities include teaching in optics, preclinical optometry, vision therapy and strabismus/amblyopia courses.
Narges Kasraie, OD, FAAO, Diplomate of ABO, is a professor at University of the Incarnate Word Rosenberg School of Optometry. She provides patient care as an attending optometrist at the Eye & Vision Care Clinic and engages in educational activities such as teaching lectures and directing laboratories in various optometric fields.
Allison Cronin, OD, FAAO, is a Clinical Assistant Professor at the University of the Incarnate Word’s Rosenberg School of Optometry and Chief of the Sports and Vision Enhancement Service at UIW Eye Institute. Her didactic responsibilities include teaching in preclinical optometry courses and sports vision.
Allan McCleary, OD, is a Clinical Assistant Professor at the University of the Incarnate Word’s Rosenberg School of Optometry and Coordinator for the UIWRSO Pediatrics and Vision Rehabilitation Residency Program. His didactic responsibilities include teaching courses in ophthalmic optics, neuroanatomy, clinical internship (school screenings), preclinical optometry, vision therapy and strabismus/amblyopia. He sees patients in the pediatrics clinic, sports vision clinic, vision therapy clinic, neuro-optometric rehabilitation clinic and the adult primary care clinic.
Srihari Narayanan OD, PhD, FAAO, is a Professor and Director of Cornea and Dry Eye Service at the University of the Incarnate Word Rosenberg School of Optometry. His responsibilities at UIWRSO include didactic teaching in clinical skills, anterior segment disease, problem-based learning courses and clinical precepting.
Sandra Fortenberry, OD, FAAO, is a Professor and Dean at the University of the Incarnate Word Rosenberg School of Optometry. Her primary role is now administrative; however, she still maintains didactic responsibilities in clinical optometry and clinical case management.

