
PEER REVIEWED
Developing a Consensus-Based Optometry Residency Military Unique Curriculum
Christopher S. Alferez, OD, FAAO, Anita Samuel, PhD, Holly Meyer, PhD, and Kevin M. Jackson, OD, MPH, FAAO
Abstract
Military optometry residencies currently do not adequately address the unique eyecare challenges faced by military optometrists. This study addresses the need for military-specific optometric education within residencies by identifying elements of an optometry Military Unique Curriculum (MUC). A modified nominal group technique was utilized involving Kern’s Six-Step Approach to Curriculum Development for Medical Education. The expert panel determined a curriculum goal, MUC topics, an ideal MUC learning environment and optimal MUC capacity. Implementing this curriculum within military optometry residency programs could improve vision readiness and care within the Military Health System.
Key Words: optometry residency curriculum, Military Unique Curriculum, curriculum development, nominal group technique
Background
The Defense Health Agency (DHA) supports medical readiness in two aspects: It promotes a ready medical force, which is the preparedness of military health personnel to care for the warfighter, and it promotes a medically ready force, which is the preparedness of the warfighter against health threats.1 Vision readiness is one of the key components of medical readiness.2 It is defined as the visual ability required of military personnel to perform their mission safely and efficiently.3 Military optometrists serve at the forefront of vision readiness as the primary eyecare providers for the nation’s service members. Like their civilian counterparts, they perform eye examinations, prescribe glasses and contact lenses, and diagnose and treat ocular conditions. However, due to their status as service members and the special population they serve, they perform duties that differentiate them from civilian optometrists when they address ocular and visual issues unique to the warfighter. Because military optometry is crucial for vision readiness, a curriculum tailored specifically for the armed forces is necessary. To ensure this, military optometrists need to be able to address military-specific issues. Examples of such issues include triaging/treating combat ocular trauma, managing visual complications of traumatic brain injury (TBI), examining patients in austere deployed environments, and performing military vision readiness physicals.
Currently, there are five optometry residency programs in U.S. military facilities. The Army has two Primary Care Optometry residencies and one Vision Rehabilitation (Brain Injury Rehabilitation) Optometry residency. The Navy has one Primary Care/Ocular Disease Optometry residency. Lastly, there is one Tri-Service Vision Rehabilitation residency program. Currently, there is no optometry residency specific to the Air Force. Given the vast resources available in their respective facilities, each of these residency programs is fully capable of providing military-specific optometric training. However, this military-specific training is either significantly underdeveloped or completely absent within these military optometry residency programs. Without such training, the programs risk residents being unprepared to face the challenges unique to military optometry. Consequently, military vision readiness will be at stake.
Military optometry residencies can implement a Military Unique Curriculum (MUC) to address this issue. The DHA defines MUC as “the integrated educational activities for trainees to learn and apply their specialty expertise to the scope of practice required for expeditionary medicine and unique issues of the MHS [Military Health System] patient population.”4 In fact, the DHA has mandated the implementation of MUCs within all military graduate medical education (GME) programs.4 The Uniformed Services University of the Health Sciences (USUHS) has championed the concept of MUCs.5 Further, during the 16th Annual Conference on Military Medicine at USUHS, a group of experts developed a model to identify and prioritize MUC content for GME programs within the military.5 De Lorenzo emphasized that MUC implementation is important because solely developing clinical skills and medical knowledge during training is not enough to prepare learners to face military-specific operational challenges.6 As a result, MUCs have been implemented in various medical programs throughout the military, including anesthesia, internal medicine, emergency medicine and infectious disease.7-11 Of these MUCs mentioned in the literature, a wide range of military-specific topics are described, including tactical combat casualty care, combat stress, military occupational health, and force health protection. Studies of MUC effectiveness demonstrated greater perceived readiness for post-residency military operational assignments and improved deployment medicine knowledge.8,9,11 These studies demonstrate practical benefits of implementing a MUC within military medical training programs.
Currently, all military optometry residencies do not have well-defined MUCs. It is also noteworthy that the Association of Schools and Colleges of Optometry currently does not define a residency category or emphasis area related to military practice.12 The Accreditation Council for Optometric Education (ACOE) states that all optometric residencies should define specific goals and outline curricular content.13 A MUC could be implemented within the goals and curricular content of an optometric residency. Thus, a needs assessment was conducted in this study to define the elements of a military-specific optometry curriculum that can serve as the first steps for military optometric residencies to fulfill the DHA mandate of MUC implementation.
This study aims to answer the question: What elements should be integrated into an optometry residency MUC to address the unique challenges that military optometrists encounter?
Methods
Methodological framework
To develop the MUC, a modified nominal group technique (NGT) was implemented. This technique effectively reaches consensus through collaboration and prioritizes information discussion.14 The NGT process generally involves five steps: (1) introduction, (2) silent generation of ideas, (3) sharing of ideas, (4) group discussion and (5) voting. The modified NGT process was modeled after the peer coaching NGT study by Bell et al. and the military refractive surgery curriculum NGT study by Evangelista et al.15,16 The NGT was selected to answer the research question because it enables equal representation of expert voices and has been successfully utilized for curriculum development.16-19
Kern’s Six-Step Approach to Curriculum Development for Medical Education provided the conceptual framework for this study.20 The six steps are: (1) problem identification and general needs assessment, (2) targeted needs assessment, (3) goals and objectives, (4) educational strategies, (5) implementation and (6) evaluation and feedback. Because this study was primarily a needs assessment, steps 1-3 were the focus of this study. Step 1 involves problem identification, where a healthcare need or problem is identified, and general needs assessment, which is an evaluation of the ideal approach vs. the current approach of the curriculum. Step 2 assesses the needs of the curriculum’s targeted learners and their learning environment. Step 3 defines the curriculum’s broader goals and the specific objectives that would achieve the goals.
This study was submitted to the institutional Human Research Protections Office, which determined that Institutional Review Board review was not required.
Study sample
To determine the elements of the optometry residency MUC, an expert panel was identified. The panel consisted of four military optometry residency program directors and the three optometry service branch leaders (the Army Optometry Consultant, the Air Force Optometry Consultant and the Navy Optometry Specialty Leader) for a total of seven panelists. These panelists were selected based on their extensive teaching and/or military optometric expertise. The majority of the panelists had military operational or deployment experience. Furthermore, the service branch leaders were included due to their seniority and broad, strategic overview of military optometry in their respective branches. Panelists consented to participate in the NGT through email response, but they could also opt out of the study at any time before or during the session. All seven invited panelists agreed to and participated in the NGT. Table 1 provides a summary of the panelist demographics.
Data collection and analysis
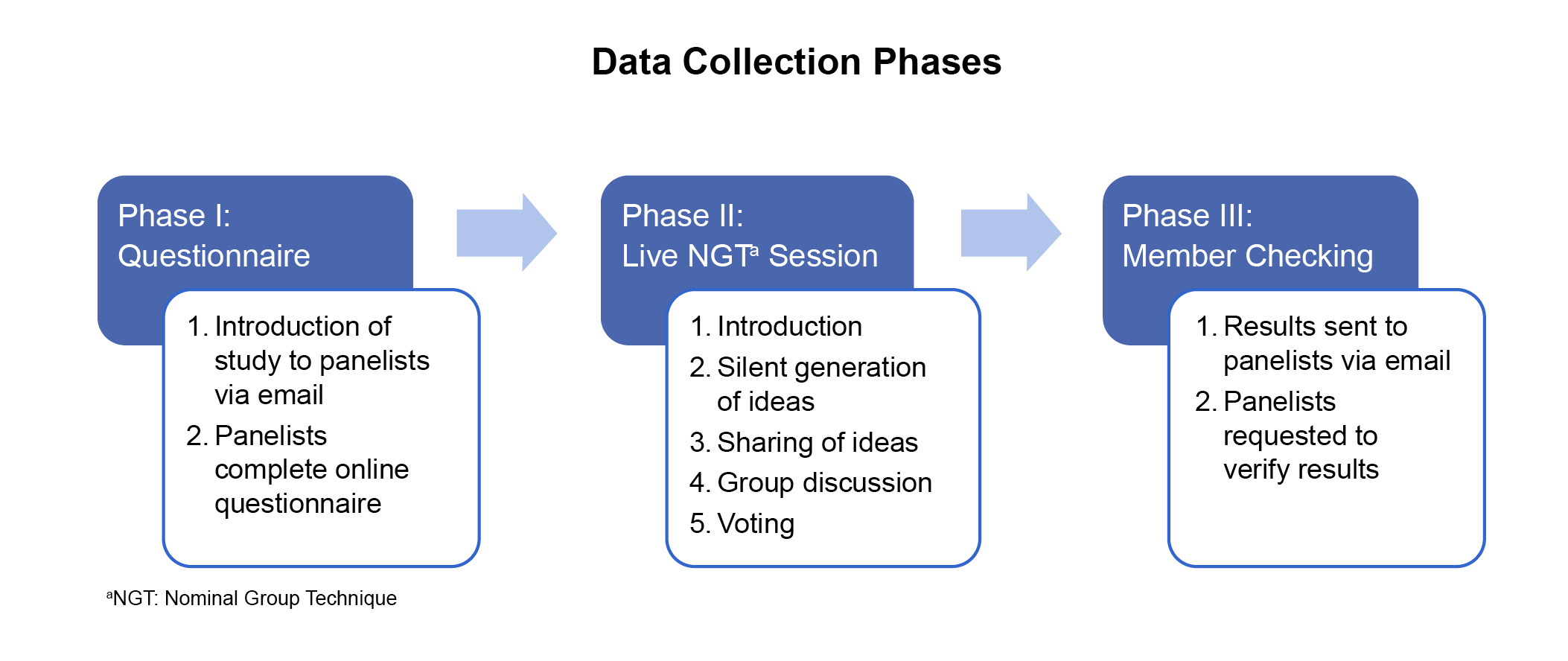
Figure 1. Click to enlarge
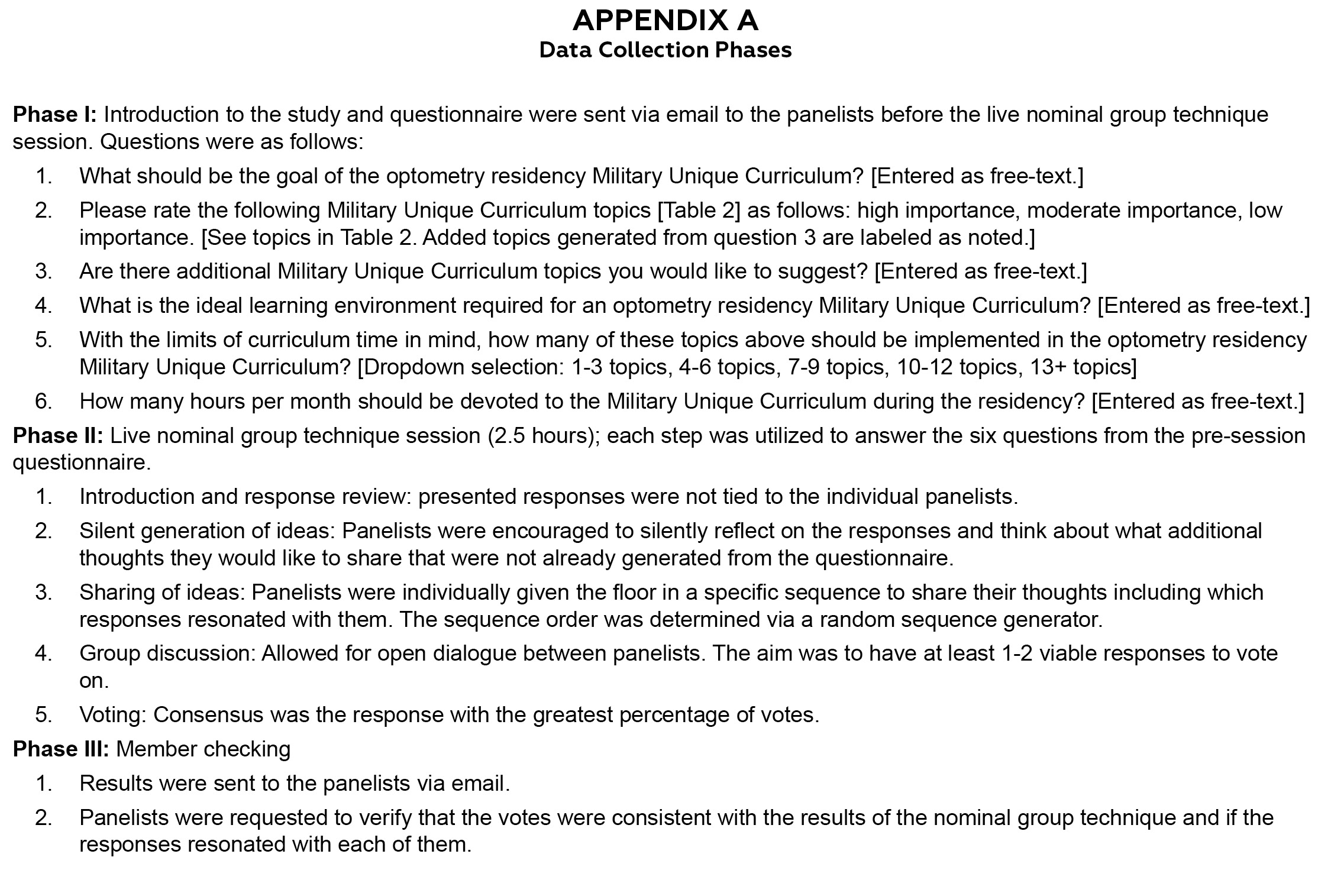
Data collection involved three phases (Figure 1 and Appendix A). The first phase was a six-question questionnaire emailed to the panelists. This questionnaire was guided by Kern’s Six-Step Approach to Curriculum Development for Medical Education.20 A list of 18 military optometry-related topics was derived from the USUHS Ocular Trauma Skills Laboratory (Jackson KM. Uniformed Services University of the Health Sciences Ocular Trauma Skills Laboratory, Military Optometry Education Assessment Presentation. May 2021) and panelists were invited to suggest additional topics (Table 2). The questionnaire sent to the panelists is included in Appendix A.
The second phase was the synchronous live NGT session conducted via online video conferencing and recorded for data analysis. The session consisted of five steps (Figure 1, Phase II). Panelists were provided an outline of the session and then given the de-identified panelist responses from the questionnaire in Phase I. Afterwards, the panelists silently generated ideas after reviewing the results. Next, the panelists individually held the floor and shared their ideas on the responses in a round-robin format. Responses were then discussed among the panelists. Lastly, the panelists anonymously voted on a consensus response for each question. Consensus was defined as the result with the most votes. This process was repeated for each of the six questions from the questionnaire.
 Table 1. Click to enlarge |
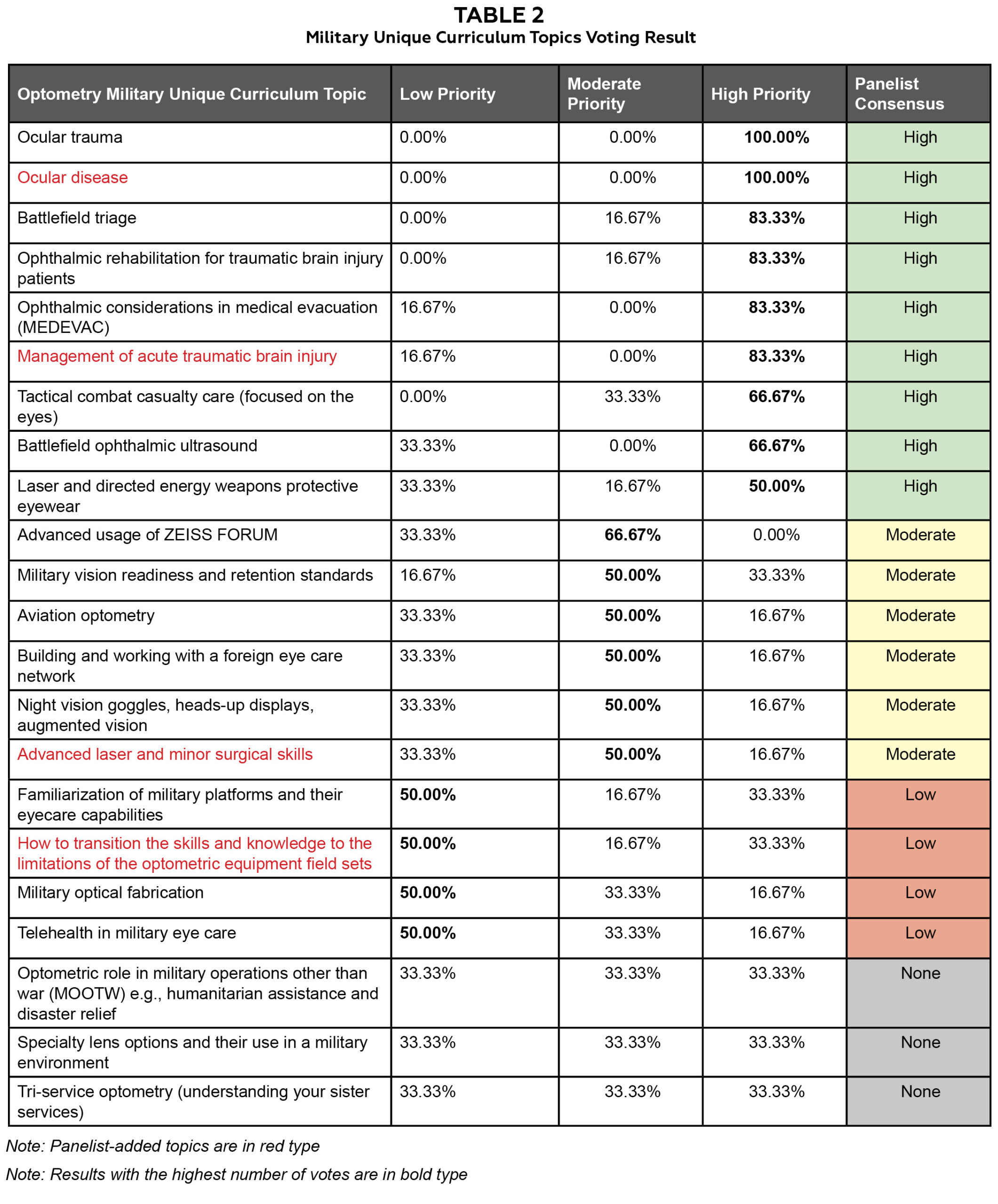 Table 2. Click to enlarge |
The third phase involved member checking the voting results, which enabled the panelists to validate the votes and ensure the responses resonated with them (Figure 1, Phase III). After member checking, the NGT was determined to be complete and ready for data analysis. Data analysis involved both qualitative and quantitative methods. The votes were quantified to identify consensus responses. CA, HM and AS conducted a thematic analysis of the transcribed recording. They independently coded the data and met to discuss their findings. Through an iterative process of qualitative coding, themes and subthemes were identified, which allowed further contextual insight.20
Results
The synchronous live NGT session results are organized below by themes: MUC goal, MUC topics, learning environment and capacity.
Goal of an optometry residency Military Unique Curriculum
The group discussion on the goal of an optometry residency MUC raised three themes: visual rehabilitation, ocular disease and the need to be prepared for operational environments (i.e., combat deployment). The panelists agreed that visual rehabilitation should be integrated into residency training because TBI is a frequent warfighter injury. Ocular disease was directly related to operational environments because optometrists need the knowledge to independently manage ocular diseases in remote and under-resourced locations typical of wartime deployments. After the discussion, the following consensus MUC goal was identified: The goal of an optometry residency MUC should be to train military optometrists in advanced practice and procedures related to TBI/vision rehabilitation, ocular disease, as well as military-centric issues to increase KSAs (knowledge, skills and abilities) for wartime deployments. Note that for the purposes of this study, the term “military-centric” is synonymous with “military-specific.”
Military Unique Curriculum topics
In addition to the 18 MUC topics provided in the questionnaire, the panelists identified four topics: ocular disease, management of acute TBI, advanced laser and minor surgical skills, and how to transition the skills and knowledge to the limitations of the optometric equipment field sets. During the synchronous NGT, these four options were added to the original list of topics; thus, the panelists voted on 22 topics (Table 2). Panelist consensus was based on the result with the highest number of votes (Table 2).
Nine topics were identified as high-priority. During the discussion, one of the panelists asserted that the Ocular Trauma Skills Laboratory at USUHS should be mandatory for residents. This comment was consistent with the panel’s unanimous vote of ocular trauma and ocular disease as high-priority topics. Other high-priority topics included battlefield triage and ophthalmic rehabilitation for TBI patients. Six topics, including military vision readiness and retention standards and aviation optometry, were considered moderately important. The importance of understanding aviation optometry’s dynamics, perceptions and misperceptions was mentioned during the discussion, but overall it was seen as a topic of moderate priority. Four topics were considered low priority, and three did not achieve consensus in the voting.
Learning environment
Panelists agreed that an optimal learning environment would provide opportunities for hands-on training with high volume and/or high complexity of patients. The panelists also emphasized the importance of exposure to austere or under-resourced environments to help prepare residents for deployment. Consequently, the panelists reached a consensus that an optometry residency MUC should “provide access to both field training and advanced clinical care for TBI (i.e., Centers of Excellence) and have high volume and/or high complexity of patients along with access to subspecialists.”
Capacity
Residency programs have a finite time to accomplish their goals. Recognizing this constraint, participants were asked how many military-specific topics should be implemented in a MUC. The panelists selected three ranges to vote on: 1-3, 4-6 and 8-10. Considering only military context-specific topics, the consensus was that 4-6 topics (50%, n=3) would be optimal (Table 3).
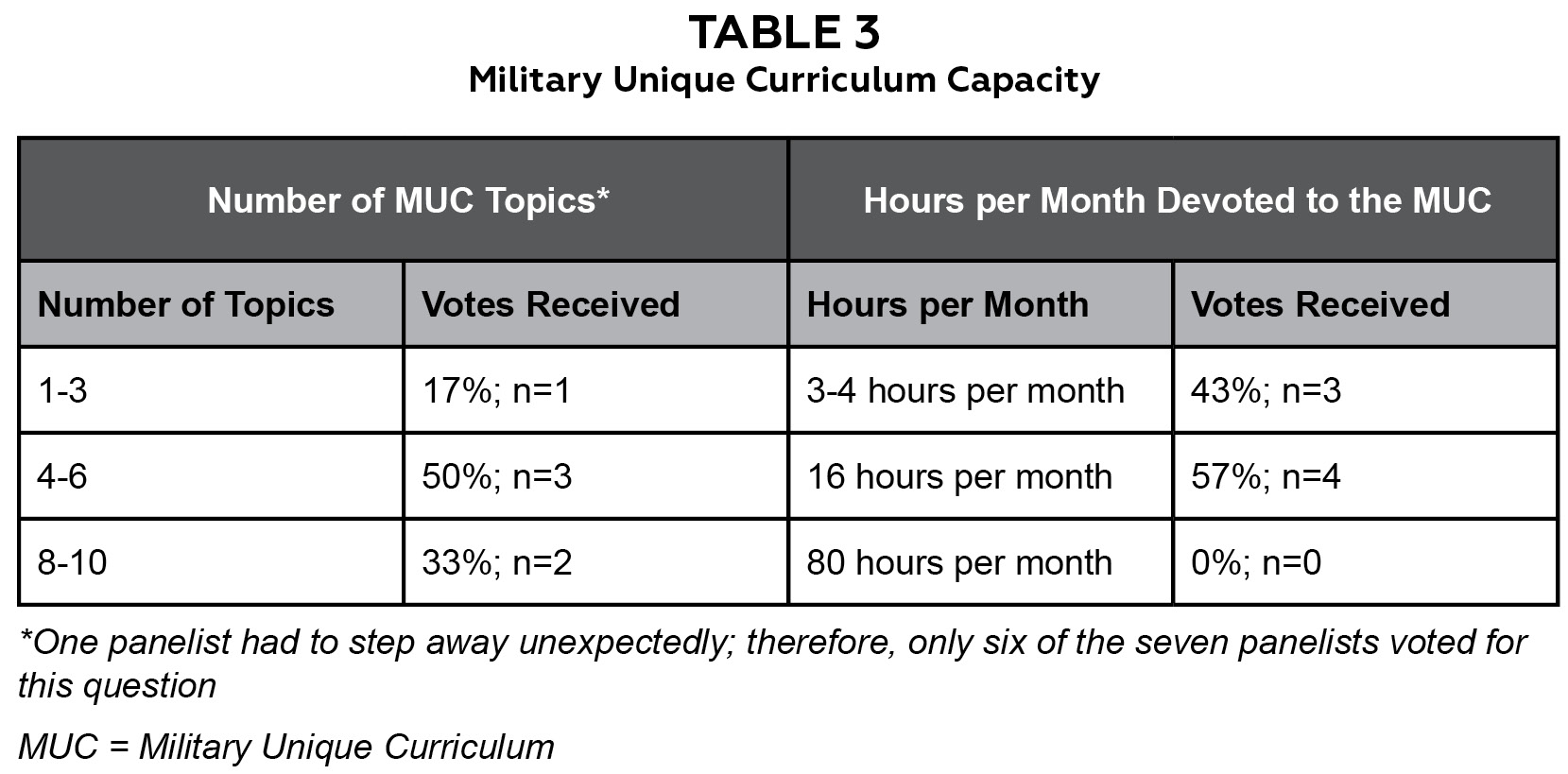
Table 3. Click to enlarge
The panelists also voted on the number of hours per month devoted to the MUC within an optometry military residency program. The panelists selected three voting choices for the number of hours per month: 3-4, 16 and 80. The panelists discussed that 16 hours is based on one-half day per week, and one of the panelists suggested 80 hours, arguing that half of the residents’ total of 160 working hours per month should be dedicated towards MUC topics. The consensus was that 16 hours a month (57%; n=4) should be devoted to the MUC (Table 3).
Discussion
Military healthcare providers are in a unique position relative to their civilian counterparts because they must be both proficient in their medical specialty and knowledgeable in military-specific issues. Currently, military optometry residencies do not sufficiently address military-specific issues within their curricula. Implementation of a MUC could serve as a means to address this gap. In this study, we utilized Kern’s Six-Step Approach to Curriculum Development for Medical Education to help identify elements of the MUC.20 The NGT was employed to address Kern’s steps 1-3: (1) problem identification and general needs assessment, (2) targeted needs assessment and (3) goals and objectives.
The panelists in this study agreed that the MUC goal should be to “train military optometrists in advanced practice and procedures related to TBI/vision rehabilitation, ocular disease, as well as military-centric issues to increase KSAs (knowledge, skills and abilities) for wartime deployments.” As with other MUCs, the panelists in this study focused on commonly encountered military-specific issues to maximize the effectiveness of the MUC. Nine topics were voted as high-priority, two of which were topics added by the panelists (ocular disease and management of acute TBI). The curricular limitations and time constraints of residency training as outlined by the ACOE residency standards were acknowledged in the suggestion for 4-6 military-specific topics covered over 16 hours.13 The panelists also reinforced the need within residency programs for contextual training and advanced competency, also emphasized by the ACOE.13
This study focused on the creation of a curriculum designed for military optometry residency programs. However, the framework and findings have implications for civilian optometric educators as well. Methodologically, this study further supported utilizing the NGT as an effective strategy for consensus decisions. Also, the NGT can be conducted fully online, enabling access to geographically dispersed subject experts. Delphi studies and expert interviews have been used to formulate curricula.22-25 However, these are resource intensive in time and money.26-27 Optometric educators therefore may find value in utilizing the NGT when designing or revising curricula.
This study also highlighted the effectiveness of using a curriculum development framework such as Kern’s six-step model. The model provides a structured approach to designing curricula and ensures that all elements of curriculum design are considered. The Kern model has been used extensively in medical education. This study demonstrated that Kern’s evidence-based curriculum development model can also be used in optometric education.
The limitations of this study included addressing only Kern’s steps 1-3, leaving Kern’s steps 4-6 (educational strategies, implementation, and evaluation and feedback) for future research. The notable time and resource commitments of Kern’s curriculum development model precluded inclusion of all steps. Future studies to develop this optometry residency MUC could consider including the other elements of Kern’s Six-Step Approach that were not included in this study, especially educational strategies and implementation. In addition to the consensus data from the NGT, epidemiological data from prior wars and conflicts would further augment the curriculum material. Lastly, the service branch leaders did not have resident teaching experience; however, their feedback was valuable, given their broader knowledge of military optometry at the strategic level.
Conclusion
Through the consensus of a military optometry expert panel, we developed a framework for a formalized Tri-Service optometry residency MUC. With this consensus curriculum, military optometry residency programs can prepare residents to become a ready medical force, from fixed-facility locations stateside to deployed locations worldwide. Consequently, the curriculum can promote a medically ready force by enhancing vision-saving eye care on the battlefield, improving visual rehabilitation of injured service members returning from combat, and ensuring vision readiness for deployable forces, fully leveraging the unique role of the military optometrist.
References
- 7 Ways DHA Ensures a Ready Medical Force [Internet]. Washington, DC: U.S. Department of Defense; 2020 Oct 2 [cited 2022 Aug 8]. Available from: https://www.defense.gov/News/Feature-Stories/story/Article/2370587/7-ways-dha-ensures-a-ready-medical-force/.
- Medical Services. Ophthalmic Services [Internet]. Washington, DC: Departments of the United States Army, Navy, Air Force. Army Regulation 40-63, SECNAVINST 6810.1, AFI 44-117; 2015 Apr 14 [cited 2022 Aug 8]. Available from: https://armypubs.army.mil/epubs/DR_pubs/DR_a/pdf/web/r40_63.pdf.
- Vision Conservation and Readiness [Internet]. Defense Centers for Public Health – Aberdeen; [updated 2019 Nov 6; cited 2023 Jan 11]. Available from: https://phc.amedd.army.mil/topics/workplacehealth/vcr/Pages/default.aspx.
- Defense Health Agency Procedural Instruction 1025.04: Graduate Medical Education [Internet]. Defense Health Agency Department of Defense; 2022 May 18 [cited 2022 Aug 8]. Available from: https://www.health.mil/-/media/Files/MHS/Policy-Files/Signed-DHAPI-102504-Graduate-Medical-Education.ashx.
- Cloonan C, Fauver HE Jr, Holloway HC, et al. Military unique curriculum: identifying and prioritizing content. Mil Med. 2003 Sep;168(9 Suppl):41-5.
- De Lorenzo RA. How shall we train? Mil Med. 2005 Oct;170(10):824-30. doi: 10.7205/milmed.170.10.824.
- Nagy CJ. The importance of a military-unique curriculum in active duty graduate medical education. Mil Med. 2012 Mar;177(3):243-4. doi: 10.7205/milmed-d-11-00280.
- Roop SA, Murray CK, Pugh AM, Phillips YY, Bolan CD. Operational medicine experience integrated into a military internal medicine residency curriculum. Mil Med. 2001 Jan;166(1):34-9.
- Engelbert LPR, Deaton TG, Walrath BD, Rudinsky SL. The joint emergency medicine exercise: a capstone training evolution of a military unique curriculum for emergency medicine residents. Mil Med. 2020 Jan 7;185(Suppl 1):544-548. doi: 10.1093/milmed/usz209.
- Markelz AE, Barsoumian A, Yun H. Formalization of a specialty-specific military unique curriculum: a joint United States Army and United States Air Force infectious disease fellowship program. Mil Med. 2019 Oct 1;184(9-10):509-514. doi: 10.1093/milmed/usz006.
- Murray CK, Reynolds JC, Boyer DA, et al. Development of a deployment course for graduating military internal medicine residents. Mil Med. 2006 Oct;171(10):933-6. doi: 10.7205/milmed.171.10.933.
- ASCO Residency Titles and Descriptions [Internet]. Rockville, MD: Association of Colleges and Schools of Optometry; [cited 2023 Jan 10]. Available from: https://optometriceducation.org/current-students/residency-programs/asco-residency-titles-and-descriptions/.
- Optometric Residency Definition and Standards Effective July 1, 2017 [Internet]. Accreditation Council for Optometric Education; [updated 2021 May; cited 2023 Jan 10]. Available from: https://theacoe.org/Affiliates/ACOE/Documents/ACOE/Residency_Standards_Adopted_by_ACOE_effective_07_%202017_updated_05_2021.docx.
- Harvey N, Holmes CA. Nominal group technique: an effective method for obtaining group consensus. Int J Nurs Pract. 2012 Apr;18(2):188-94. doi: 10.1111/j.1440-172X.2012.02017.
- Bell A, Meyer H and Maggio L. On the same page: building best practices of peer coaching for medical educators using nominal group technique [version 1]. MedEdPublish 2019, 8:95 [Internet]; [cited 2022 Aug 8]. Available from: https://doi.org/10.15694/mep.2019.000095.1.
- Evangelista CB, Larsen KL, Cervero RM, Samuel A. Corneal laser refractive surgery curriculum development in the military: using the nominal group technique. Mil Med. 2023 Jan 4;188(1-2):e145-e151. doi: 10.1093/milmed/usab262.
- Chamane N, Kuupiel D, Mashamba-Thompson TP. Stakeholders’ perspectives for the development of a point-of-care diagnostics curriculum in rural primary clinics in South Africa-nominal group technique. Diagnostics (Basel). 2020 Apr 1;10(4):195. doi: 10.3390/diagnostics10040195.
- O’Neil MJ, Jackson L. Nominal group technique: a process for initiating curriculum development in higher education. Studies in Higher Education. 1983;8(2):129-38. doi 10.1080/03075078312331378994.
- Parr E, Done M. Curriculum development and the nominal group technique: gaining the practitioners’ view. Journal of Education for Librarianship. 1979;19(3):223-32.
- Thomas PA, Kern DE, Hughes MT, Chen BY. Curriculum development for medical education: a six step approach. Baltimore: Johns Hopkins University Press; 2015.
- Patton MQ. Qualitative research & evaluation methods: Integrating theory and practice. 4th ed. Thousand Oaks: SAGE Publications, Inc; 2015.
- Viljoen CA, Millar RS, Manning K, Burch VC. Determining electrocardiography training priorities for medical students using a modified Delphi method. BMC Med Educ. 2020 Nov 16;20(1):431. doi: 10.1186/s12909-020-02354-4.
- Kizawa Y, Tsuneto S, Tamba K, et al. Development of a nationwide consensus syllabus of palliative medicine for undergraduate medical education in Japan: a modified Delphi method. Palliat Med. 2012 Jul;26(5):744-52. doi: 10.1177/0269216311410346.
- Varkey P, Karlapudi S, Rose S, Swensen S. A patient safety curriculum for graduate medical education: results from a needs assessment of educators and patient safety experts. Am J Med Qual. 2009 May-Jun;24(3):214-21. doi: 10.1177/1062860609332905.
- Johnson KE, Coleman K, Phillips KE, et al. Development of a facilitation curriculum to support primary care transformation: the “coach medical home” curriculum. Med Care. 2014 Nov;52(11 Suppl 4):S26-32. doi: 10.1097/MLR.0000000000000240.
- Powell C. The Delphi technique: myths and realities. J Adv Nurs. 2003 Feb;41(4):376-82. doi: 10.1046/j.1365-2648.2003.02537.x.
- Bolderston A. Conducting a research interview. J Med Imaging Radiat Sci. 2012 Mar;43(1):66-76. doi: 10.1016/j.jmir.2011.12.002.
- Sweet LR, Palazzi DL. Application of Kern’s six-step approach to curriculum development by global health residents. Educ Health (Abingdon). 2015 May-Aug;28(2):138-41. doi: 10.4103/1357-6283.170124.
- Scala JJ, Braun NJ, Shamardani K, Rashes ER, Wang W, Mediratta RP. Applying Kern’s six steps to the development of a community-engaged, just-in-time, interdisciplinary COVID-19 curriculum. J Med Educ Curric Dev. 2022 Apr 28;9:23821205221096370. doi: 10.1177/23821205221096370.
- Chen BY, Kern DE, Kearns RM, Thomas PA, Hughes MT, Tackett S. From modules to MOOCs: application of the six-step approach to online curriculum development for medical education. Acad Med. 2019 May;94(5):678-685. doi: 10.1097/ACM.0000000000002580.
- Said JT, Schwartz AW. Remote medical education: adapting Kern’s curriculum design to tele-teaching. Med Sci Educ. 2021 Jan 25;31(2):805-812. doi: 10.1007/s40670-020-01186-7.
Appendix A. Click to enlarge

