
Evaluation of Interprofessional Education and Collaboration in Optometry
Lisa W. Christian, OD, FCOVD, FAAO, Sarah MacIver, OD, FAAO, Marg Alfieri, RD, FDC
Abstract
To evaluate the impact of interprofessional education (IPE) in final-year optometry learners, a questionnaire was given to assess their knowledge, attitude and skill around interprofessional collaboration (IPC) before they completed a placement with an interprofessional health clinic. Results showed that a majority of learners believed there is an increasing need for IPE and IPC in optometry and felt the development of multidisciplinary ideas and the enhancement of patient-centered care are the main benefits. Both the learners and clinic members indicated that they gained a personal satisfaction working together and were interested in future collaborations. Further investigation is required to enhance the understanding of how optometry improves patient care outcomes in an interprofessional setting.
Key Words: interprofessional education, interprofessional collaboration, family health team, primary health care, optometry learners
Background
Interprofessional collaboration (IPC) encourages integration of healthcare services and has shown positive impact on professional practice, quality of care and health outcomes.1,2,3 IPC between optometry and ophthalmology is well-established; however, collaboration between optometry and other health professions is not standard practice.4,5 With both the aging population and the chronic disease population increasing, the risk of vision loss also increases. The most common causes of vision loss are diabetic retinopathy, macular degeneration, glaucoma and cataracts. These causes are often co-morbid with common chronic diseases such as diabetes, hypertension and cardiovascular disease.6,7,8 An integrated model of primary care optometry in IPC teams with health professions such as family medicine, nursing, pharmacy and social work, may reduce health threats to older individuals and augment chronic disease management.6, 9, 10
D’Amour and colleagues have described interprofessional teams as groups of professionals that work collaboratively to enhance patient-centered care.11 This organization of different health professionals aims to better meet population needs and provide improved service integration and coordination. In order to effectively develop collaborative skills, health professionals need to work outside the scope of their own professional identity and learn about the expertise and values of other health disciplines.11,12 While many health professions have adopted the IPC model, Canadian optometry has not readily engaged in this type of practice.13
The literature suggests IPC is fostered by improved interprofessional education (IPE).14 To date, IPE has been established as a mandatory component in health professional programs such as medicine, nursing, social work, pharmacy and dietitian/nutrition but is not so in the optometry curriculum.14 It is thought that if learners are trainedto be competent as a member of an interprofessional team, more collaborative practice opportunities will arise, increasing the opportunities for learning and teaching.14,15 The hope is that introducing IPE to optometry learners will yield the same results.
To explore the potential of IPC in Canadian optometry, the University of Waterloo School of Optometry and Vision Science along with the Centre for Family Medicine (CFFM) in Kitchener, Ontario, Canada, developed an IPE teaching methodology to educate healthcare providers and optometry learners on the potential role optometry can play within interprofessional health care. The purpose of this study was to evaluate interprofessional collaboration and education in optometry learners and explore the benefit to patient care when optometry is integrated into a family health team (FHT) focused on diabetes managed care.
Methods
Ninety fourth-year optometry learners were offered a voluntary one day in total placement with the CFFM FHT’s Diabetes Clinic between January 2011 and June 2012. Only 50 placements were available and participation was determined on a first-come, first-served basis. The Diabetes Clinic included physicians, physician assistants, dietitians, pharmacists, nurses and learners from each represented health profession. Optometry’s role was to educate patients with diabetes on the importance of annual eye examinations, to review the date of their last eye examination, and to provide input on patient management where appropriate. Prior to the on-site placement, all learners attended a two-hour IPC lecture that focused on optometry’s role within an IPC diabetes team and highlighted multidisciplinary knowledge exchange between optometry, pharmacy, nutrition and family medicine. Immediately following the lecture, an opinion questionnaire was given to the students to complete.
The questionnaire was derived from established studies on IPC,11,12,14,15 and questions were adjusted to be specific to final-year optometry learners. The focus of the questionnaire was on three areas: 1) the optometry learners’ understanding of IPC (knowledge), 2) the perceived need for collaboration between optometry and other health professionals (attitude), and 3) the competency and ability of optometrists to practice in interprofessional teams (skills).16,17 The questions were self-reflective, and the respondents were asked to rate how they agreed with each statement on a seven-level Likert response scale (Appendix A). Likert responses with values of 1 (strongly disagree) to 3 were recorded as negative responses; responses with values of 5 to 7 (strongly agree) were recorded as positive responses; and responses of 4 were recorded as neutral.
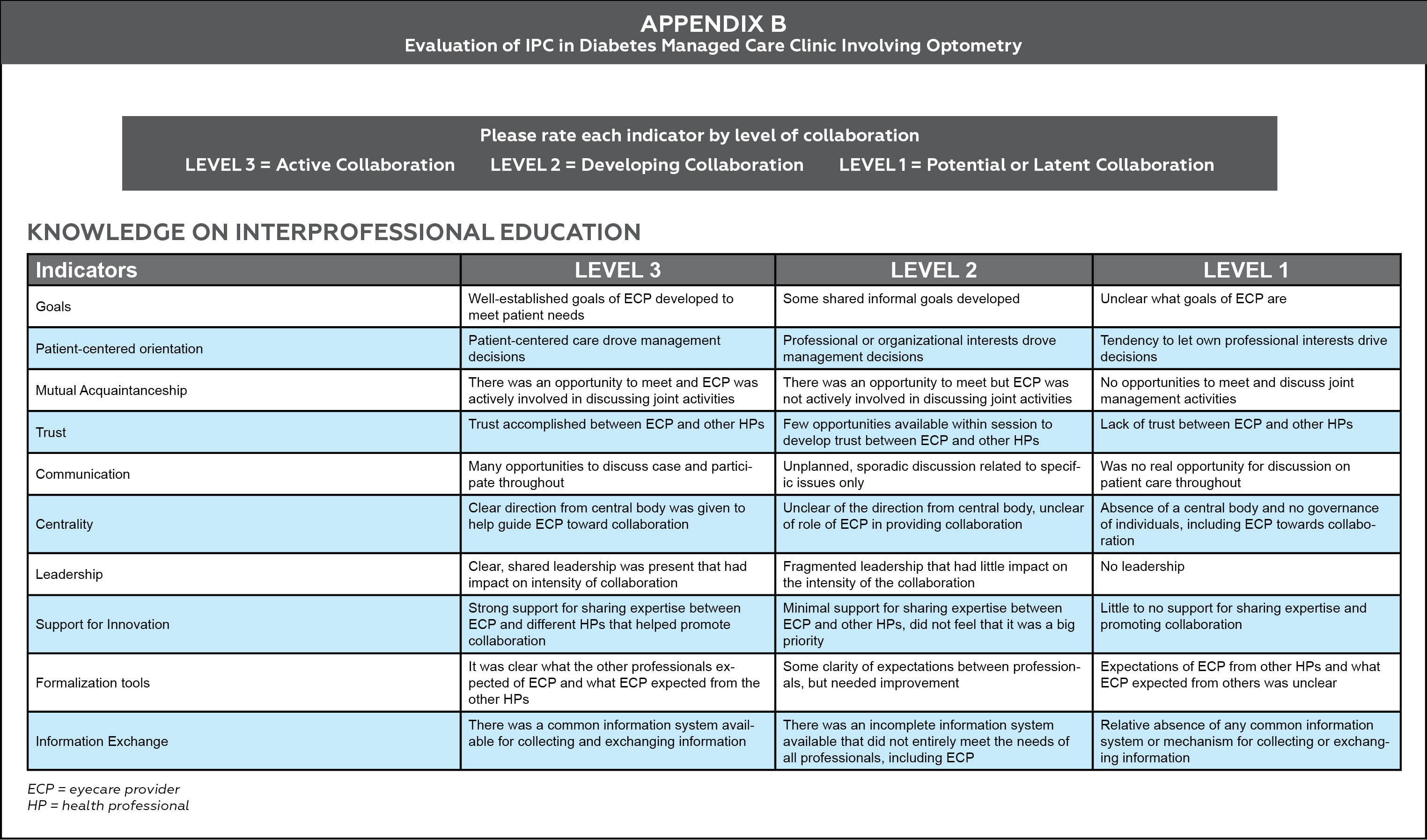
Following the IPC Diabetes Clinic, a post-IPC online survey (Appendix B) was offered to the 50 optometry learners as well as the 15 health professionals and interprofessional learners to evaluate the intensity of collaboration between optometry and the interprofessional team in the Diabetes Clinic. The survey was adapted from D’Amour’s12 “A model and typology of collaboration between professional healthcare organizations.”
Ethics approval for this study was received from the University of Waterloo Research Ethics Board. The participants were given a cover letter outlining the study, and informed consent was assumed if the participants chose to fill out the questionnaire.
Results
A total of 81 fourth-year optometry learners filled out the opinion questionnaire based on the knowledge, attitude and skill of an IPC approach to patient care. This was done prior to participating in the IPC Diabetes Clinic. Twelve optometry learners and seven members of the IPC (Diabetes) FHT completed the same post-IPC survey to assess the intensity of the collaboration between the two groups.
Prior to IPC exposure: knowledge
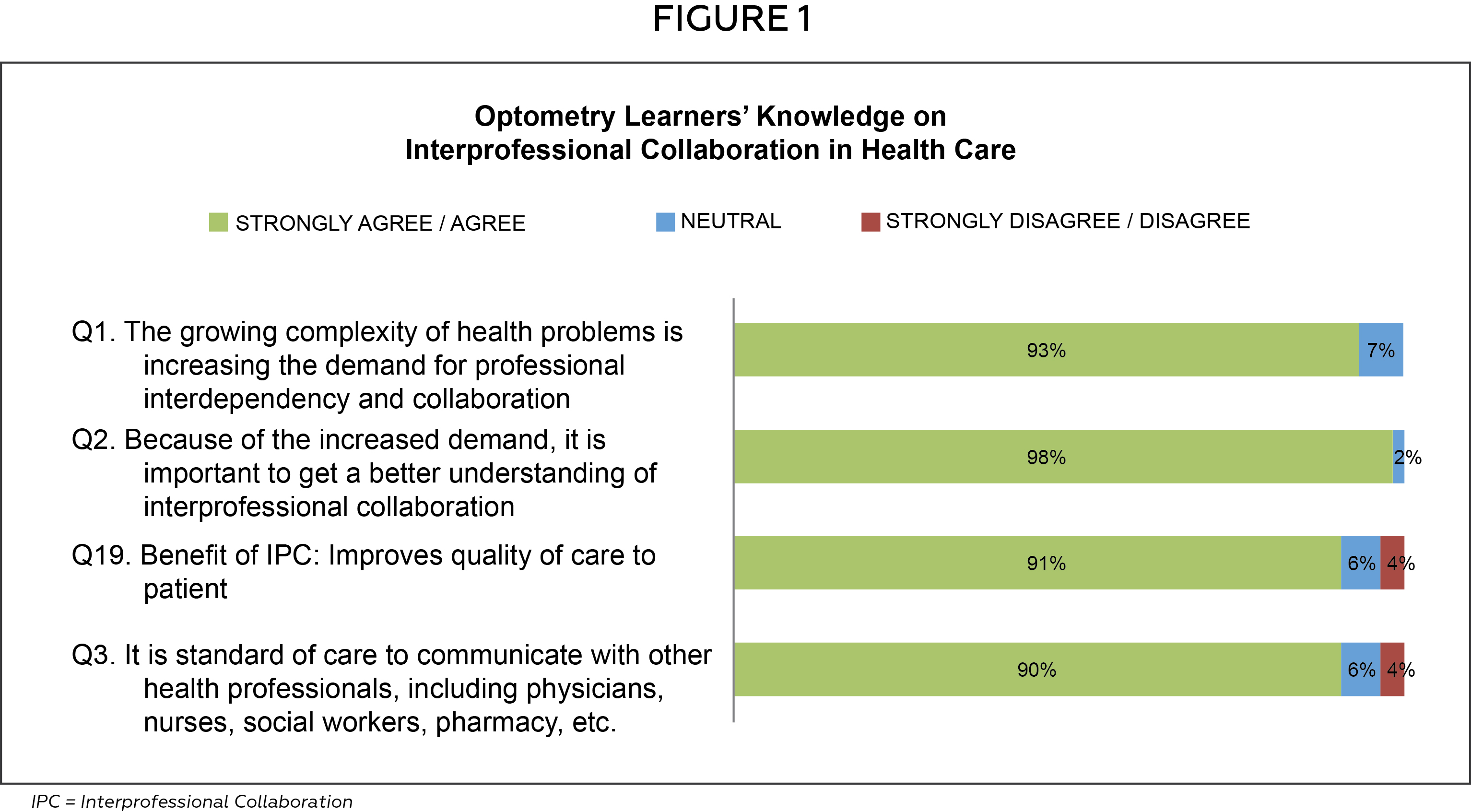
To evaluate optometry learners’ knowledge of IPC we divided this section into IPC in health care (Figure 1) and self-assessment of how to utilize IPC in clinical practice (Figure 2).
Click image to enlarge
Figure 1 illustrates the optometry learners’ primary understanding of IPC in health care. When asked, the majority of learners felt there was an existing patient need for health professionals to practice IPC (93%; Q1), and a better understanding of IPC was needed (98%; Q2). Learners also agreed collaborative practice was an important component in improving the quality of patient care (91%; Q19) and that IPC was the standard for patient care (90%; Q3).
Figure 2 depicts the learners’ understanding of the utilization of IPC in clinical practice. The majority (>90%) of optometry learners believed the greatest benefit of IPC was enhanced patient care (93%; Q16) and the collaborative development of ideas and management plans by a team of healthcare professionals (94%; Q15). However, only half of the learners were clear about which patients (52%; Q26) and which patient care situations (46%; Q28) would benefit from an IPC team, and only slightly more than a third felt they understood the process of coordinating IPC in clinical practice (37%; Q31).

Click image to enlarge
Prior to IPC exposure: attitude
Responses involving the learners’ attitudes toward their readiness and toward optometry’s role were variable (Figure 3). Although the majority of learners felt their optometric education promoted an intercollaborative approach to patient care (65%; Q63), they also felt they needed additional training in IPC to feel more comfortable with it (79%; Q42). In addition, while learners expressed the patient benefit of an IPC team (Figure 1: 91%; Q19), most felt more comfortable working within optometry than collaborating with other health professionals (64%; Q45). However, they indicated that further expertise outside the optometry arena would increase their level of comfort (85%; Q52).

Click image to enlarge
Slightly more than half of the learners felt other health professionals are highly motivated to work with optometrists (56%; Q55) but fewer than a quarter felt that other health professionals understand the role optometry has in patient care (20%; Q40 and 22%; 41). A large majority of the learners felt that an optometrist’s input on a patient’s well-being would be valuable to other health professionals (90%; Q35) and identified an interest in learning more about professional collaborations (77%; Q34).
Prior to IPC exposure: skills

Click image to enlarge
Optometry learners were asked to evaluate how they currently practice IPC within their clinical education (Figure 4). Only a third of the learners admitted to consulting regularly with other health practitioners (35%; Q66); however, most did feel an expectation to consider the entire patient history (physical, psychological, social) when making patient care decisions (93%; Q67). The majority of optometry learners felt optometrists listened to and considered the opinions/views of other health professionals (78%; Q75) and felt the patient was included in management decisions (83%; Q70) and that this was a high priority (95%; Q71) for patient care.
Post-IPC exposure

Click image to enlarge
A comparison of post-IPC exposure results between optometry learners and the IPC diabetes FHT can be seen in Figures 5 and 6 respectively. While the number of post-IPC responses was low, the FHT responses appeared to consider the intensity of collaboration with optometry more active than the optometry learners. Similarly, optometry learners did not always feel included within the IPC team (Figure 5; mutual acquaintanceship), while the FHT felt that all members contributed equally (Figure 6; mutual acquaintanceship). Survey results also revealed a positive shift in attitude from the optometry learners about communicating and engaging in interprofessional care with other members of the healthcare team. Overall, the majority of the optometry learners felt that the intensity of collaboration in the identified areas of IPC was developing, while the FHT members felt that the intensity of collaboration in those areas was already active between optometry and the team.
Discussion
Interprofessional collaboration is the process of individual health professionals working together to positively impact patient-centered care.12,15 In recent years, the literature has reported on the benefits of IPC as it continues to become increasingly prominent in primary health care.13 Interprofessional education in a clinical setting has also been shown to offer valuable learning opportunities and establish a greater understanding of IPC within each profession.14,18 IPE is necessary to help prepare learners from various professions to develop the competencies needed to work together and understand the individual skill set each profession carries. To date, there has been no literature on IPE within Canadian optometry, which remains one of the only health professions in Canada that does not (formally) include a component of IPE in the curriculum.

Click image to enlarge
The literature documenting the benefit of IPC between optometry and ophthalmology is well-established.4,5 While this collaborative relationship is important for optimum eye care, optometry also has an important and expanding role in interprofessional collaboration with other primary care providers, such as family medicine, pharmacy, nursing, social work and nutrition, to improve interdisciplinary collaboration and patient-centered care in practice.1,14,17 To successfully establish this model of health care, it has been suggested that IPC should be included in each profession’s curriculum.18
Before developing a model for IPE within the optometry curriculum, we wanted to evaluate final-year optometry learners’ knowledge, skills and attitudes toward optometry’s current role in IPC. To do so, we assessed the learners’ understanding of IPC via a questionnaire.16, 17 Overall, our findings were very positive toward the benefit of optometry in IPC. Optometry learners indicated they were interested in gaining knowledge about IPC and felt IPC was an important component in providing optimal patient care. However, the survey also identified barriers to implementing IPC, which were similar to those reported by other health professions.16,19 One of the identified barriers was the lack of understanding regarding the role that optometry would have in an IPC clinical setting. In addition, the survey found that learners had a level of discomfort in working and communicating with other healthcare practitioners. Results indicated a need to improve IPE in the optometry curriculum in order to foster a better understanding of optometry’s role in IPC and improve the comfort level of working with other healthcare practitioners. IPE ideally occurs within collaborative practice settings where learnerscan be exposed to practical educational experiences. The creation of more IPC opportunities is therefore required between optometry and other health professionals.14
Prior to this study, optometry had not been part of the diabetes management team, and no role had been established for optometrists at the time of participation. There was no set expectation on the optometry learner about the level of involvement because the purpose was to investigate the role of the learner within an IPC team.
A post-IPC survey was distributed evaluating the intensity of the collaboration between optometry and the other health professionals. Although the participation in this part of the investigation was low, our findings showed that the optometry learners’ felt there was either a developing or active level of collaboration in all areas surveyed. The evaluation of the experience showed that IPC with optometry could exist from the perspectives of the optometry learners and the FHT members. While the FHT members felt a high intensity of collaboration with optometry (Figure 6; information exchange), the optometry learners felt that the intensity was still developing (Figure 5; information exchange). This area of discrepancy should be further explored among the participants surveyed. Overall, the post-IPC survey results suggested a value for optometry being present in a FHT setting and that there is an ongoing need for optometry to part of a FHT to better develop and strengthen collaboration.
Where to Go from Here: Culture Shift
A primary care IPC team with optometry integration may be a valuable model for risk reduction of vision loss in high-risk individuals. We would like to further develop and evaluate this model. As part of this, we want to strengthen the IPE component in the optometry curriculum at the University of Waterloo. The literature supports that increased collaborative opportunities lead to increased understanding of optimal optometry integration.6,9,10 Other health professions need exposure to the scope of practice of optometry, as this will create a demand for optometry to be embedded within healthcare settings, e.g., primary care. We have continued to incorporate optometry into other IPC primary care clinics at CFFM, such as the mobility clinic for persons with severe physical challenges, the C5-75 clinic for patients older than 75 with frailty, and the Healthy Futures clinic, a clinic to ensure 3-year-olds are healthy. By providing optometry learners clinical training in these clinics, we are helping them build practice skills for use in similar environments after graduation. The integration fosters trust and acknowledgment of skills among all professions, including optometry.14
The published literature supports collaborative efforts in health care and the positive impact they have on improving patient satisfaction, coordinated access to resources and reduction of costs associated with redundant medical examinations and clinical errors.1,21 We believe that optometry working in a collaborative team effort will have the same positive effects by improving access to care for patients at high-risk for vision loss and reducing associated costs to the healthcare system by limiting unnecessary referrals to tertiary care providers (i.e., ophthalmology). By doing so, we hope to create a model where we can demonstrate that benefits exist from both the optometry and primary healthcare perspective. Further research is therefore needed to investigate how to improve the level of comfort between optometry learners and other health professionals.
Limitations
Although this was a demonstration project and the goal was to evaluate if the interprofessional collaboration of optometry in a family health team is beneficial in the optometry curriculum, there were a few limitations to the study. First, while this study was based on validated studies, a validated questionnaire was not used. Second, the small number of respondents to the post-IPC survey from among both the optometry learners and the FHT limited the conclusions that could be drawn. For future studies, a validated questionnaire should be used and repeated after participation in the collaborative clinic to determine whether there was an improvement in knowledge, skill and/or attitude.
Conclusion
There is a need for optometry to become embedded into interprofessional primary care, if the goal of optimal patient care is to be achieved. Optometry has seen recent gains in its scope of practice, allowing the profession to utilize all of its skills. The profession is best equipped in the primary healthcare system to manage primary vision care needs that go beyond prescribing glasses and involve the prevention and management of many eye conditions. IPC has been gaining recognition as a preferred model for primary healthcare delivery; however, Canadian optometry has not yet explored the potential role in this model. This qualitative investigation helps to recognize that there is a role for optometry in IPC acknowledged both by the optometry profession and the members of an IPC team. This study also demonstrates the need for optometry to include IPE in its curriculum to help cultivate the development of optometry-integrated IPC. We hope to further develop the preliminary models explored in this study to help better understand how interprofessional interventions in optometry affect patient care and outcomes.
Acknowledgements
The authors would like to express sincere thanks to Dr. Joseph Lee, Chair and Lead Physician, The Centre for Family Medicine FHT, and the CFFM Diabetes Clinic for their support and participation in this study.
The research for this paper was supported by an American Optometric Foundation Vistakon Innovation in Education Grant.
References
1. Zwarenstein M, Goldman J, Reeves S. Interprofessional collaboration: effects of practice-based interventions on professional practice and healthcare outcomes. Cochrane Database of Systematic Reviews. 2009;3.
2. Ontario Ministry of Health and Long Term Care. Ontario’s Action Plan for Health Care; c2012 [cited 2014 Jun 19]. Available from: https://www.health.gov.on.ca/en/ms/ecfa/healthy_change/docs/rep_healthychange.pdf.
3. Goldman J, Meuser J, Rogers J, et al. Interprofessional collaboration in family health teams: an Ontario-based study. Can Fam Physician. 2010;56(10):368-74.
4. Budning A. Model of interprofessional collaboration in the care of patients with glaucoma and those suspected of having glaucoma. Can J Ophthalmol. 2011;46(6):460-1.
5. Nicolela M, Buys Y, Birt C, et al. Model of interprofessional collaboration in the care of glaucoma patients and glaucoma suspects. Canadian Glaucoma Society Committee of Interprofessional Collaboration in Glaucoma Care. Can J Ophthalmol. 2011;46(6 Suppl):S1-21.
6. Fong A, Lee G. Reducing vision loss in chronic eye disease. Aust Fam Physician. 2009;38(10):774-9.
7. Chiang P, Zheng Y, Wong T, et al. Vision impairment and major causes of vision loss impacts on vision-specific functioning independent of socioeconomic factors. Ophthalmol. 2013;120(2):415-22.
8. Lord S. Visual risk factors for falls in older people. Age Ageing. 2006;35 (Suppl) 2:42-5.
9. Taylor HR, Pezzullo ML, Keefe JE. The economic impact and cost of visual impairment in Australia. Br. J. Ophthalmol. Mar 2006;90(3):272-275.
10. Taylor HR. Eye care for the community. Clin Experiment Ophthalmol. 2002;30(3):151-4.
11. Amour D, Ferrada-Videla M, San-Martin Rodriguez L, et al. The conceptual basis for interprofessional collaboration: core concepts and theoretical frameworks. J Interprof Care. 2005;19 (Suppl) 1:116-31.
12. D’Amour D, Goulet L, Labadie JF, et al. A model and typology of collaboration between professionals in healthcare organizations. BMC Health Serv Res. 2008;8:188.
13. A guide to chronic disease management and prevention. Ontario Ministry of Health and Long Term Care Family Health Teams; 2005. [cited 2014 Jun 25]. Available from: https://www.health.gov.on.ca/en/pro/programs/fht/docs/fht_chronic_disease.pdf.
14. D’Amour D, Oandasan I. Interprofessionality as the field of interprofessional practice and interprofessional education: an emerging concept. J Interprof Care. 2005;19 (Suppl) 1:8-20.
15. Da Motta LB, Pacheco LC. Integrated medical and health multiprofessional residency programs: the experience in building an interprofessional curriculum for health professionals in Brazil. Educ Health. 2014;27(1):83-8.
16. Coleman MT, Roberts K, Wulff D, et al. Interprofessional ambulatory primary care practice-based educational program. J Interprof Care. 2008;22(1): 69-84.
17. Sicotte C, D’Amour D, Moreault MP. Interdisciplinary collaboration within Quebec community health care centres. Soc Sci Med. 2002;55(6):991-1003.
18. Joseph S, Diack L, Garton F, Haxton J. Interprofessional education in practice. Clin Teach. 2012;9(1):27-31.
19. Tremblay D, Roberge D, Cazale L, et al. Evaluation of the impact of interdisciplinarity in cancer care. BMC Health Serv Res. 2011;11:144.
20. Congdon N, O’Colmain B, Kalver C, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol. 2004;122(4):477-85.
21. Barrett J, Curran V, Glynn L, Godwin M. CHSRF synthesis. Interprofessional collaboration and quality primary healthcare. Ottawa, ON: Canadian Health Services Research Foundation; 2007. [cited 2014 Jun 25]. Available from: https://www.cfhi-fcass.ca/Migrated/PDF/SynthesisReport_E_FINAL.pdf.
Click image to enlarge

Click image to enlarge

