
PEER REVIEWED
Management of A-Pattern Exotropia
Kristen L. Kerber, OD, MS, FAAO
Abstract
A-pattern exotropia presents a unique challenge to the eyecare practitioner due to increased incidence of symptoms compared with V-pattern exotropia, as down gaze is more frequently used on a daily basis. This has been further exaggerated during the age of electronics when the amount of near work has increased and the COVID-19 pandemic has led to even more virtual activities. It is imperative to incorporate adjunct testing to fully evaluate this condition. This teaching case report discusses treatment for A-pattern exotropia including different types of prism, such as yoked or base-in, and ergonomic interventions such as using a slant board.
Key Words: exotropia, strabismus, A-pattern, prism, comitancy
Background
Strabismus is a common disorder that can be challenging for practitioners. It is especially important that it is identified early in life if it is amblyogenic. Population-based studies estimate the prevalence of strabismus in the general population to be 2.5-4.6%.1 It is further estimated that 12-50% of cases of horizontal strabismus will demonstrate a pattern or vertical incomitance.2,3 Although pathology must always be considered in non-comitant deviations, pattern strabismus is common and can be non-pathologic in origin. The two most common non-pathological conditions with pattern strabismus are infantile esotropia and intermittent exotropia, which are associated with inferior oblique overactions. Although less common, superior oblique overaction (SOOA) may also manifest as pattern strabismus. Careful case history and full sensory and motor evaluation with a dilated comprehensive eye exam are imperative for ruling out disease and recommending the best management. This teaching case report is significant in that it examines two cases of A-pattern exotropia, one presenting with an abnormal head posture (AHP). It is intended for third- and fourth-year optometry students and all clinical eyecare providers.
Case 1 Description
A 2-year-9-month-old female presented with her grandmother for her first complete eye exam with concerns regarding squinting up close and far away. The grandmother also noted she occasionally noticed an intermittent eye turn out in the child, OS > OD, daily. She was unsure of the timing of onset, but noted that it only occurred for short periods of time, then went away. Upon further questioning, the grandmother reported that the child sometimes had a chin-down posture but no eye closure. The patient’s birth history was unremarkable, but she had a history of febrile seizures as an infant, which required hospitalization twice. She was taking diazepam (Diastat) prescribed by her neurologist and Claritin. There were no known drug allergies. She had a history of speech delay, but her grandmother noted it had rapidly improved and nearly resolved since starting day care a few months prior. Also according to the grandmother, the patient’s mother had a history of exotropia and glasses wear.
Observation of the child from the waiting room to the exam room revealed a chin-down posture, but no overt strabismus. Distance visual acuity with LEA matching was 20/50 OU. Unfortunately, the patient couldn’t be engaged to test monocularly due to objection to occlusion OS > OD. Near visual acuity was central, steady, maintained with a toy OD/OS. Confrontation fields were grossly normal to distraction OD/OS, and pupils were equal, round and reactive to light with no afferent pupillary defect. Ocular motilities were significant for 2+ SOOA OD/OS in an A-pattern. No restrictions or underactions were noted in ductions. Distance cover test showed ~14-16△ X(T) with a slight OS fixation preference, Mayo scale 1.4 Near cover test showed ~18-20△ X(T) with no fixation preference, Mayo scale 1. Covering an eye for longer than 3 seconds resolved the patient’s AHP. The patient was not able to be engaged in a cover test conducted in multiple positions of gaze. Near point of convergence (NPC) was 7/10 cm, OS out, with apparent effort. Color vision and stereopsis tests were not possible due to patient understanding. Non-cycloplegic (“dry”) retinoscopy was OD: +0.50-1.25×010, OS: +0.25-1.25×180.
Slit lamp examination was unremarkable, revealing only racial melanosis OU. Digital pressures were soft and equal to palpation, and the patient was dilated with 2 gtts of 1% cyclopentolate OU. Cycloplegic retinoscopy was OD: +0.75-1.25×010, OS: +0.50-1.25×180. The patient’s dilated posterior ocular health exam was unremarkable. The grandmother was educated on the findings and asked to keep a journal at home to monitor the frequency, laterality and duration of the eye turn. A follow-up appointment was scheduled for 6 weeks to monitor control and re-attempt multiple positions of gaze cover test and monocular optotype acuity. A copy of LEA symbols was sent home for practice.
The patient was lost to follow-up for a few months but returned to the clinic at age 3. Her grandmother and preschool teacher noted consistent squinting at distance and near with an intermittent eye turn outward that occurred almost equally between the two eyes, though slightly more frequently OS. The chin-down posture was still noted at times and there was no eye closure. The grandmother noted a stable OD fixation preference at home but, interestingly, the first exam had demonstrated an OS fixation preference. No changes since the previous eye exam were reported for medical history, medications or family history.
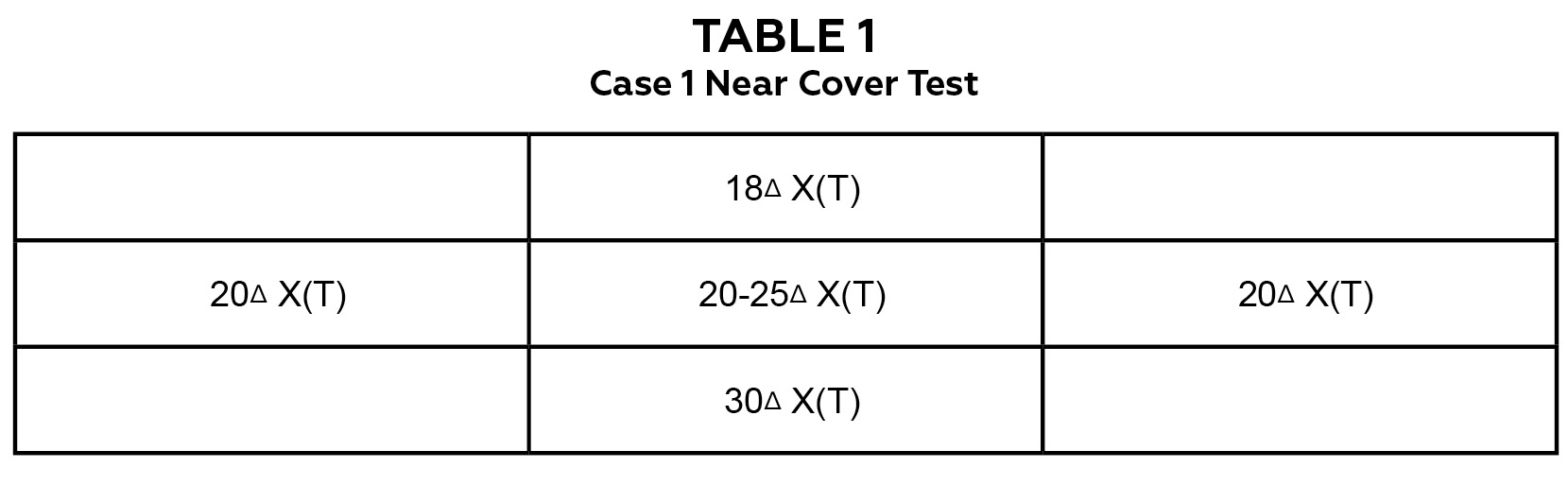
Table 1. Case 1: near cover test in multiple positions of gaze demonstrating an A-pattern exotropia.
Click to enlarge
Observation of the child from the waiting room to the exam room still revealed a chin-down posture, but no overt strabismus. Distance visual acuity with LEA matching was 20/63 OD/OS/OU, and near visual acuity with LEA matching was 20/50 OD/OS/OU. No objection to occlusion was noted. Confrontation fields and pupils were still unremarkable. Color vision testing was completed at this visit with normal findings, and global stereopsis was 400 arcsec with Randot 3. Ocular motilities were stable with 2+ SOOA OD/OS revealing an A-pattern. No restrictions or underactions were noted in ductions. Distance cover test showed 5△ XP, Mayo scale 0. Near cover test revealed ~20-25△ X(T), Mayo scale 4. Covering an eye for greater than 3 seconds again resolved the AHP. Multiple positions of gaze cover test confirmed the A-pattern, as shown in Table 1.
Near cover test was repeated with 2 DS overminus (calculated from previous cycloplegic retinoscopy) OU and 2△ base-down yoked prism. The patient’s head immediately straightened with the trial frame, and near cover test showed 12△ X(T), Mayo scale 2. A glasses prescription was provided with OD: -1.50-1.25×010, 2△ BD and OS: -1.75-1.25×180, 2△ BD. The patient was asked to return in 8 weeks for follow-up.
At the second follow-up visit 8 weeks later, the grandmother noted that the patient wore the glasses full-time, and AHP and squinting fully resolved. She reported a rare eye turn outward, only when the patient was angry or crying. The grandmother also noted that the glasses sometimes slip down the child’s nose. There was no change since last eye exam reported for medical history, medications or family history.
Observation of the child from the waiting room to the exam room revealed no AHP or overt strabismus. Distance visual acuity with LEA matching was 20/40 OD/OS/OU, and near visual acuity with LEA matching was 20/40 OU. No objection to occlusion was noted. Confrontation fields and pupils were still unremarkable. Ocular motilities were stable with 2+ SOOA OD/OS revealing an A-pattern. No restrictions or underactions were noted in ductions. Distance cover test showed 4△ XP, Mayo scale 0, and near cover test showed 10△ XP, Mayo scale 0. Stereopsis with Randot 3 was 100 arcsec. It was recommended that the patient continue full-time glasses wear, and rubber temple hooks were recommended for the glasses to prevent slippage. The patient was asked to return for follow-up in 8-12 weeks, or sooner if symptoms or frequency of the eye turn changed.
Case 2 Description
An 11-year-old African American male presented with his father for a complete eye exam. He reported blurred vision at near while reading, which began a couple of years prior. He was unsure of the exact timing of the symptom onset after beginning reading, but noted that it happens “pretty quick.” Associated symptoms included sharp frontal headaches, asthenopia and binocular horizontal diplopia. The patient had no history of glasses wear. He noted that the only way to improve symptoms was to discontinue reading. Sometimes his symptoms interfered with his hobby of playing video games, after he is on the computer for long periods of time. The patient and his father denied ever noticing an eye turn, AHP or frequent eye closure. The father reported that the patient does well in school, but it is difficult to get him to read for school or fun. He was in the sixth grade and denied having an individualized education plan or other extra help/services. His most recent eye exam had been 3 years ago, and the father noted that everything was “normal” at that time. After the previous exam note was reviewed, the assessments were mild hyperopia OU (functional emmetropia) and a convergence insufficiency type intermittent exotropia with “good control.”
The patient’s medical history was positive for asthma for which he used Flovent and ProAir inhalers. He had no history of surgeries, hospitalizations or known drug allergies. Family history was positive for hypertension, diabetes and asthma.

Table 2. Case 2: distance cover test in multiple positions of gaze demonstrating an A-pattern exotropia. Click to enlarge
Uncorrected distance visual acuity was 20/20 OD, 20/20-1 OS, and 20/20 OU. Uncorrected near visual acuity was 20/20 OD/OS/OU. Ocular motilities were significant for 1+ SOOA OD and 2+ SOOA OS. No underactions or restrictions were noted on ductions. Distance cover test was 8△ XP and near was 12-14△ XP. Table 2 shows cover test findings in multiple positions of gaze. NPC was 8/10 cm, left eye out with suppression. Stereopsis was nil, but Worth 4 Dot (W4D) testing showed fusion at both distance and near. After an A-pattern deviation was noted in cover testing, stereopsis and W4D tests were repeated. Stereopsis was 12.5 arcsec with Randot 3 in primary gaze, and W4D showed crossed diplopia in down gaze. Confrontation fields, pupils and anterior segment biomicroscopy were within normal limits. Dry retinoscopy was +0.75 DS OU.
After prism adaptation testing, the patient was stable and comfortable with 8△ base-in total (4△ base-in OD and 4△ base-in OS). Modified Thorington in down gaze showed a 4△ exotropia deviation, NPC was to the nose, and W4D demonstrated fusion in down gaze at near. The patient was given a children’s sports magazine to read for 30 minutes. At the conclusion of this trial, the patient reported continued comfort and reported he had never been able to read for that long in one sitting. Clear and single vision was reported for 100% of the trial period.
Digital pressures were soft and equal to palpation. The patient was dilated with 2 gtts of 1% tropicamide OU and retinoscopy was +1.50 DS OD and +1.25 DS OS. The dilated posterior ocular health exam was unremarkable.
Treatment options were discussed. These included ergonomic changes/behavioral modifications such as using a slant board to prop up reading material more in primary gaze rather than down gaze. The option of prism glasses was discussed including insurance’s replacement policy if glasses were lost or broken. A vision therapy program was also discussed. The patient and father chose a combination of prism glasses and use of a slant board. A plano glasses prescription was provided with split base-in prism (4△ base-in OD and 4△ base-in OS). No hyperopic correction was included due to good uncorrected visual acuity and lack of blur symptoms during prism testing.
A follow-up call was conducted 3 months later. The patient and father reported resolution of symptoms with the glasses, which the patient wears for all near work. An annual comprehensive eye exam was recommended at that time.
Education Guidelines
Key concepts
- Primary, secondary and tertiary actions of cyclovertical extraocular muscles
- Adaptations when binocular vision is compromised
- Ancillary testing in sensorimotor evaluations
Learning objectives
After this case discussion, participants should be able to:
- Recognize the different signs/symptoms in patients with primary gaze deviations vs. those with non-comitant deviations
- Develop an ocular motility protocol to evaluate a pattern strabismus
- Know the difference between objective and subjective testing of strabismus
- Understand the pathophysiology of A-pattern exotropia
- Understand potential issues related to quality of life and barriers to care
Discussion questions
1. Knowledge and concepts
- How is strabismus classified?
- What different types of pattern strabismus are there?
- What type of testing can be done to evaluate strabismus?
2. Differential diagnosis
- What are the differential diagnoses to be considered?
- Is it a pathological or non-pathological deviation?
- Are there associated amblyopia or amblyogenic risk factors?
3. Management
- Does the patient require optical intervention?
- What kind of prism could be used?
- How can prism adaptation be assessed?
- Could vision therapy play a role?
- Is the patient eligible for surgical intervention?
- What is the most appropriate follow-up schedule?
4. Patient education and barriers to care
- What is the most effective way to educate a patient or parent regarding this condition?
- How does this affect the patient’s quality of life?
- What options are provided for young children who have trouble with the fit of glasses or frequently break them?
Assessment of learning objectives
- Students can be tested on the classification of strabismus
- Students can be presented with a case of reported or presumed strabismus and be required to conduct the components of patient history and ask the pertinent questions
- Students should be evaluated on their ability to come up with a list of differential diagnoses and how to rule out each
- Critical-thinking skills can be evaluated by asking students which adjunct testing can be used to assess strabismus and evaluate the effect of the chosen treatment
Discussion
Beyond direction of the deviation, strabismus has further classifications: horizontal vs. vertical, unilateral vs. alternating, constant vs. intermittent, comitant vs. non-comitant. Each aspect is important in understanding the cause and impact of the strabismus. For younger patients, it is especially important to treat amblyogenic strabismus. To assist in quantifying the patient’s control, intermittent exotropia control scales such as Newcastle or Mayo can be used. The Mayo scale has been well-studied and is therefore used in this case discussion. It is a 5-point scale ranging from phoria (0) to constant exotropia (5) that describes whether or not the intermittent exotropia manifests spontaneously or only under dissociated conditions.4
It is important to note that non-comitant deviations can be phorias or tropias; therefore, patients may not always present with diplopia complaints, but potentially asthenopic complaints and/or avoidance behaviors. Vertical incomitancy describes a horizontal misalignment that differs in up and down gazes.2,5 By convention, these findings are not considered clinically significant unless different by ≥ 10 prism diopters for A-patterns5 and ≥ 15 prism diopters for V-patterns.2,3,6 The practitioner should obtain measurements that are ~25-35 degrees above and below the midline to ensure that the patient is looking far enough in the desired direction.2,3,5,6
Pattern deviations describe relative convergence and divergence, and the letters are assigned based on the shape the eyes mimic. V and A patterns are most common, and X, Y and λ (lambda) are less common. The most common non-pathological non-comitant pattern deviation is V-pattern exotropia. These patients typically present with inferior oblique overaction and fewer symptoms than in A-pattern exotropia because up gaze is not as frequently used in day-to-day activities. Down gaze tends to be the most important functionally after primary gaze. The prevalence of A-patterns among all strabismus ranges from 4.5-36% in various epidemiology studies, with A-pattern esotropia deviations being ~2x as common as A-pattern exotropia deviations.5 There are no known racial, age or sex predilections. Adults may become more symptomatic for A-pattern exotropia deviations at the start of presbyopia as they look down through bifocal or progressive-addition lenses as opposed to unconsciously moving material upward toward primary gaze in single-vision lenses. All non-comitant deviations require careful testing to rule out other neurological conditions.
The differentials include, but are not limited to, uncorrected refractive error, non-strabismic binocular vision disorder, pathological strabismus and pseudostrabismus. The first step is always to correct any significant refractive error as this may cause pseudo pattern deviations (such as in accommodative esotropia) and better vision tends to promote better binocularity. In the absence of strabismus, patients may have symptoms that are similar if there are accommodative, vergence or oculomotor dysfunctions. Pathological strabismus can be caused by ocular disease, paralytic or restrictive etiologies, which can be assessed with ductions (including forced duction testing) and a thorough anterior and dilated posterior ocular health exam. Imaging should always be considered if any neurological findings are present or when the cause of the pattern cannot be confidently identified.
Ductions should be conducted for patients with pattern strabismus or those with any apparent underaction during version testing. Although patterns are often detected through version testing, multiple positions of gaze cover test is important for determining comitancy and isolating which muscles are most likely affected. Interestingly, ocular torsion can be seen on fundus exam when comparing the positions of the fovea and optic nerve head.3,6 Stereopsis, W4D and diplopia field testing are all useful sensory evaluations. Modified Thorington can be additive in understanding the subjective angle vs. the objective angle measured by cover test. Double Maddox rod is of further use when assessing torsion.
The stereopsis and W4D tests are of interest in case 2, as practitioners need to consider in which gaze the testing is conducted. The stereopsis books are often held upright in down gaze, not always straight ahead. Due to the A-pattern exotropia in this patient, his stereopsis was significantly different when tested in the two positions. Similarly, W4D testing is often conducted in primary gaze, but practitioners should also consider the complaint or findings when conducting this test. If only obtained in primary gaze, this patient’s findings appeared normal, but testing in down gaze reaffirmed his complaint of diplopia when reading. Sensory findings may vary depending on whether the patient is phoric in any position of gaze or if the strabismus is intermittent. If the patient is strabismic in all or the majority of positions, suppression and anomalous retinal correspondence (ARC) may be noted. Interestingly, in regard to ARC, the angle of the anomaly varies with the angle of deviation.3 In cases where ARC is found, prisms are not an appropriate management option.7
Patients may present with chin-down posture, which keeps eyes in the preferred position (up gaze), or they may present with avoidance behaviors as described above. In cases of AHP, the nose tends to point where the eyes cannot go (i.e., the most affected gaze). If AHP is not restrictive or paralytic in nature, covering an eye will often induce automatic head straightening as the patient is only symptomatic binocularly. Yoked prisms can be helpful in these cases. The minimum amount of prism needed to resolve the AHP is best for weight considerations in the glasses. Practitioners use a variety of techniques to determine the amount of horizontal prism needed, but most often use a relieving prism. Prior to prescribing prism, it is imperative to evaluate the ability for sensory fusion. If prism can improve sensory fusion status, prism is used to relieve or eliminate the motor demand. If there is no potential for sensory fusion, then prism should not be used as a mode of treatment.7 Sheard’s criteria8 or Caloroso’s Residual Vergence Demand (RVD) can be applied in such cases. RVD is best used in patients who have vergence ranges that have been maximally trained through vision therapy, but still need prism to maintain comfortable binocular vision in free space.9 There can be a difference in the objective and subjective angle. Some practitioners use techniques such as Modified Thorington to guide their prism prescribing in order to relieve the subjective angle and thereby relieve diplopia. Surgery is indicated in patients who have significant AHP or strabismus that cannot be easily managed with prism or vision therapy.
Due to the young age of the patient in case 1, vision therapy was deferred. The patient was prescribed overminus treatment to assist in the control of the intermittent exotropia by increasing her accommodative convergence. Although not thoroughly discussed here, the plan is to slowly wean her out of the overminus over time as she increases her convergence ability. When she is older, active vision therapy can be initiated if her control is fairly good, or surgical treatment can be considered if she has not gained better control.
Although there is no known genetic predisposition to this pattern strabismus, it is interesting to note that the father in case 2 also reported similar symptoms beginning in childhood and persisting into adulthood. A quick assessment of versions was conducted on the father and showed an A-pattern exotropia deviation. The pathophysiology of A-pattern exotropia deviations most commonly arises from oblique muscle dysfunctions ― in this case, primary SOOA. This results in a tertiary abduction effect that torques the eyes outward in down gaze, increasing relative divergence.3,6 In the case of primary SOOA, there is no identifiable etiology. Secondary SOOA may include inferior oblique paresis (rare) leading to an overaction of the ipsilateral superior oblique muscle (Hering’s Law).2,5,10
Horizontal rectus dysfunction may be the proposed cause in the absence of SOOA. This theory attributes the dysfunction to underaction of the medial rectus in down gaze and lateral rectus underaction in up gaze; however, there is some controversy regarding this theory.2,3,5 Vertical rectus dysfunction is another proposed theory in the absence of SOOA, though this is generally less accepted. Muscle pulley anomalies or mislocations have been supported by MRI studies, showing even small displacement can cause vertical incomitance. For example, a superior displacement of the lateral rectus pulley can induce an A-pattern.2,5
Orbital anomalies such as those seen in craniofacial disorders may also show pattern deviations and can be difficult to treat. Neither of the patients presented in this case report had one of these conditions.
Pattern deviations not acquired due to pathology do not resolve, but associated control of the horizontal deviation (i.e., intermittent exotropia) may change over time. Younger children should be followed more closely due to the risk of amblyopia and potential for more frequent refractive error changes. Patient and guardian education about AHP and quality of life is important. Quality of life issues can include musculoskeletal health and comfort, diplopia, risk of amblyopia if strabismus is amblyogenic, and positional awareness in places such as classrooms or movie theaters. For example, patients with A-pattern exotropia will have to develop a significant AHP in stadium seating if they are looking down from the top, or may have more difficulty managing stairs if they look down. In the classroom or at home, slant boards are useful for propping up material to lessen the need for down gaze. Young children are very active; therefore, the fit of glasses is extremely important not only for comfort but also to prevent them from falling down the nose or off the face. Cable temples and ear hooks/temple tips are useful.11
Conclusion
Optometrists have many tools for evaluating and treating pattern strabismus. Both motor and sensory evaluations are important in the differential diagnosis and management of strabismus. Multiple treatment options are available to optometrists, and careful history evaluation will help guide the decision of which treatment to use.
References
- Evidence-Based Clinical Practice Guideline: Comprehensive Pediatric Eye and Vision Examination [Internet]. American Optometric Association. 2017 [cited 2020 Apr 1]. Available from: https://www.aoa.org/AOA/Documents/Practice%20Management/Clinical%20Guidelines/EBO%20Guidelines/Comprehensive%20Pediatric%20Eye%20and%20Vision%20Exam.pdf.
- Saxena R, Dhiman R. Pattern Strabismus [Internet]. American Academy of Ophthalmology. 2020 [cited 2021 Jan 2]. Available from: https://www.aao.org/disease-review/pattern-strabismus.
- Hoyt C, Taylor D. Pediatric Ophthalmology and Strabismus. 4th ed. UK: Elsevier Health Sciences; 2012.
- Mohney BG, Holmes JM. An office-based scale for assessing control in intermittent exotropia. Strabismus. 2006 Sep;14(3):147-50.
- Plotnik JL. A-Pattern Esotropia and Exotropia [Internet]. Medscape. 2020 [cited 2020 Apr 1]. Available from: https://emedicine.medscape.com/article/1199714-overview.
- Agrawal S. Strabismus: For Every Ophthalmologist. Singapore: Springer; 2019.
- Jenewein EC. Perfecting Prism [Internet]. Review of Optometry. 2019 [cited 2020 Apr 1]. Available from: https://www.reviewofoptometry.com/article/perfecting-prism.
- Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders. 5th ed. Philadelphia: Wolters Kluwer Health; 2020.
- Caloroso, EE, Rouse, MW. Clinical Management of Strabismus. UK: Butterworth- Heinemann; 1993.
- Chen J, Mai G, Deng D, Lin X, Guo Y, Yang X, Yuan C. Clinical features and surgical treatment of A-pattern exotropia. Yan Ke Xue Bao. 2004 Sep;20(3):163-7.
- Glasses Fitting for Children [Internet]. American Assocation for Pediatric Ophthalmology and Strabismus. 2020 [cited 2020 Apr 1]. Available from: https://aapos.org/glossary/glasses-fitting-for-children.

