
PEER REVIEWED
Queering Optometric Education
Marlee M. Spafford, OD, MSc, PhD, FAAO, Paula S. McDowell, OD, FAAO, and Lillian Kalaczinski, OD, FAAO
Abstract
People identifying as sexual or gender minorities experience preventable health disparities through decreased opportunities to achieve optimal health and increased burdens of disease, injury, and violence. Some health professional schools have introduced relevant curricula, yet the optometric education literature is silent on such training, suggesting a potential problematic gap in the training of future optometrists. In this paper we lay out a justification for updating optometric education and offer curricular and pedagogical guidance. We adapt medical competencies for optometry to stimulate a conversation among optometric educators about how we train optometry students to provide competent care to diverse and often mistreated communities.
Key Words: optometric education, competencies, sexual and gender minorities, queer, health disparities
Introduction
Providing competent eye and vision care for all is an ideal espoused in optometric accreditation standards, cultural competence guidelines, and codes of ethics.1–4 Yet, neither these sources nor the optometric literature explicitly address the care implications for patients who identify as sexual or gender minorities. This absence is important because sexual and gender minorities experience preventable health disparities through fewer opportunities to achieve optimal health and a greater burden of disease, injury, and violence.5 Some health professional schools have introduced curricula that consider the impact of gender and sexual identity on patient care priorities and needs.6–10 However, the optometric education literature has remained silent on this aspect of training, suggesting a potential problematic gap in the training of future optometrists.
The lack of explicit attention to this area of care begins with the Accreditation Council on Optometric Education (ACOE) standards that require graduates of the professional optometric degree to attend to “diverse populations” (2.9.5), “diversity, equity, and inclusion principles” (2.9.6), and “culturally competent communications” (2.9.8).1 Similarly, graduates of ACOE optometric residencies must provide patient education, communication, and shared decision-making that is “culturally competent” (2.4.1).1 Nowhere, however, is “cultural competence” defined. In contrast, American medical schools can map their curricula to the Association of American Medical Colleges (AAMC) general competencies that include an explicit recognition of multiple relevant identities: “Demonstrate sensitivity and responsiveness to a diverse patient population, including but not limited to diversity in gender, age, culture, race, religion, disabilities, and sexual orientation” (5.5).11
Despite this AAMC competency, problems persist. In Canada and the United States, medical education about sexual and gender minorities’ health has been described as limited, inconsistent, and devoid of agreed-upon specific core competences.12 Studies in the past 10 years have found that formal education on this topic is limited to a median of 5 hours13 and most students judge their training as “fair” or worse.14 Transgender training is typically identified as the most limited sector of sexual and gender minorities health education.15–17 Limited trans health education has been found to be a barrier to competent care by medical students and residents.13,18–23 In a qualitative study of Canadian physicians, Snelgrove et al.24 compellingly characterized medical care of transgender patients as “completely out-at-sea” in part because of the normative practice of “two-gender medicine.”
Reviews and studies of medical student and resident training do not reveal pedagogical and curricular consensus; however, there is support for adopting multi-modal, scaffolded approaches that are founded in cultivating values, exploring self-awareness of privilege and bias, and enhancing communication skills.25–28
The AAMC publication “Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals who are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators”29 discusses competencies, strategies for integrating and assessing these competencies, as well as clinical scenarios and discussion points. Thirty competencies have been set across eight domains: knowledge for practice, patient care, practice-based learning and improvement, interpersonal and communication skills, professionalism, systems-based practice, interprofessional collaboration, and personal and professional development.
To date, there are few indications that the profession of optometry recognizes the need for care and training that attends to sexual and gender minorities. Denial et al.30 and the Association of Schools and Colleges of Optometry (ASCO) “Guidelines for Culturally Competent Eye and Vision Care”4 acknowledge that culturally competent optometric care includes a consideration of gender and sexual orientation, although no specific guidance is provided. The ASCO guidelines4 — currently under review — may ultimately deepen consideration of sexual and gender minority care because ASCO recently released a set of case studies31 that includes one case about respecting a patient’s pronouns and preferred name. Two of us (PSM & LK) have provided American Academy of Optometry lectures on “Optometric Care of Transgender Patients.”32,33
In this paper we aim to start redressing this apparent educational gap by laying out a justification for updating optometric education and providing curricular and pedagogical guidance. We take the AAMC competencies29 and adapt them for optometry in an attempt to stimulate a conversation among optometric educators about how we train optometry students to provide competent care to diverse and often mistreated communities.
Justifying a 2SLGBTQ+ Inclusive Optometry Curriculum
The justification for inclusive optometry curricula lies in the regularity that members of sexual and gender minority communities present for eye care, the health disparities they routinely experience, and the prevalent health impacts they encounter. A brief review of this literature anchors this justification.
Defining the communities
LGBT (lesbian, gay, bisexual, and transgender) is widely used, yet it mixes populations whose identities are based on sexual orientation (i.e., lesbian, gay, bisexual) and gender identity (i.e., transgender), it falsely implies mutually exclusive categories, it incorrectly presumes homogeneity regarding needs and priorities, and it presupposes binary masculine/feminine and hetero/cisgender norms. Cover34 discusses the continually evolving “taxonomy” that proliferates in an attempt to include disenfranchised voices from traditional LGBT and binary-norming discourses. The recognition that LGBT fails to fully describe all sexual and gender minorities has led to various longer acronyms. In this paper, we use 2SLGBTQ+ to acknowledge that “two-spirit” (2S) Indigenous people were the first sexual and gender minorities living on Turtle Island (North America), gender queer individuals (Q) have non-binary gender identities, and additional sexual and gender minorities exist (+).35
The AAMC “Resource for Medical Educators”29 maintains the LGBT “shorthand,” separating the differing care needs within that grouping, and considers two additional diverse populations to address the LGBT-identity shortfall: people who are “gender nonconforming” and people “born with differences in sex development” (DSD). Gender non-conforming people purposefully express their gender differently from gendered societal norms, while people born with DSD have atypical features of their gonads, genitalia, or sex chromosomes (e.g., congenital adrenal hyperplasia, androgen insensitivity syndrome, Klinefelter Syndrome, Turner Syndrome). This AAMC resource importantly notes that identities are declared by the person; the process of establishing one’s identity naturally evolves over time, particularly among youth; and gender identities do not predict sexual histories, practices, and feelings.
Estimates of the 2SLGBTQ+ population in North America depend on self-reporting and survey wording.36 Statistics Canada and the United States Census Bureau have historically collected binary female/male data; however, this strategy fails to recognize sex-gender differences or capture non-binary identities. This can be remedied with a survey that employs a two-step question about the person’s assigned sex at birth and their current gender identity, with the latter including transgender and non-binary options. Statistics Canada has collected sexual orientation data since 2003 and adopted the two-step question in its 2021 census,36–38 while the United States Census Bureau has yet to collect either.39 American estimates can be gleaned from the annual Behavioral Risk Factor Surveillance System (BRFSS),40 which includes questions about sexual orientation and gender identity without employing the two-step question.
Adult 2SLGBTQ+ community estimates are 3.6% in Canada41 and 4.5% in the United States42; however, age impacts these estimates. North American surveys of younger adults (under 35 years of age) report estimates two to three times higher than surveys of all ages.41–44 Blackless et al.45 estimate that one in 100 people are born with DSD, noting that DSD itself does not determine sexual or gender identity. Depending on practice demographics, optometrists will regularly or frequently provide care to 2SLGBTQ+ patients.
Drivers of health disparities
Sexual and gender identities are social determinants of health; this is particularly true of gender identity. Hatzenbuehler and Link46 identify the underpinnings of health disparities among gender minorities as structural (e.g., government policy, institutional practices), interpersonal (e.g., abuse, rejection, discrimination), and individual (e.g., concealing identity, internalized stigma). Gender identity is a social stratifier that can exclude people from society and services.25 Sexual and gender minorities experience greater health disparities if they identify with additional socially constructed marginalized identities.47,48 For example, in addition to facing heterosexist, homophobic, and transphobic oppression, two-spirit Indigenous individuals encounter racist and colonial oppression by government and mainstream society and marginalization within a Western LGBT community.49 These traumas combine to significantly increase rates of substance abuse, addiction, suicide, morbidity, and mortality relative to non-Indigenous peers.49 Ng50 posits that health practitioners need to proactively practice through a lens of intersectionality by acknowledging that membership in multiple minority groups affects patient health in terms of risks, care experiences, decision-making, and outcomes.
Sexual and gender minorities are marginalized by societal heteronormativity and cisnormativity. The former assumes people are and should be heterosexual; the latter presumes gender aligns with assigned sex at birth.25 These normative assumptions fuel phobias that can be hostile, particularly in the case of transphobia.25 Social norms regarding sexual and gender identities can inform laws about what constitutes legal consensual sexual behavior and hate crimes, leaving some people — particularly those who are older or have lived in certain countries — not expecting safe health care.29,51,52 Stigmatized social status creates a “minority stress” that risks mental health and heightens vigilance regarding further negative experiences.53,54 While minority stress can build resilience in the form of “group-level coping” among members of minority groups,54 repeated and significant trauma more likely creates vulnerability in the form of negative health outcomes or risky behaviors.29
People who are transgender or gender non-conforming routinely encounter negative healthcare experiences, including discrimination, microaggressions, hostility, abuse, and knowledge gaps.55–60 Gender minorities delay or avoid health care because of concerns about practitioner behavior, affordability due to socioeconomic status or insurance coverage, and potential negative outcomes of hormonal therapy.61–63 They are reluctant to disclose their gender identity, and health facilities are ill-equipped to accurately collect their identity data.63
Sexual and gender societal norms can problematically impact health education and health research.25 Societal homophobia and transphobia are not unlearned through healthcare education when it is taught through biomedical or biopsychosocial positivist approaches that silence or limit consideration of the social constructs of gender and sexuality.25,64 Das Gupta et al.65 argue that health education must be informed by a social justice lens to avoid commonly occurring harmful practices such as service providers deciding whether patients will obtain access to gender-affirming care.66–68
Health research can further obfuscate the mindset of healthcare providers. For example, there is limited research about two-spirit Indigenous health, and the destruction and distortion of records by priests, missionaries, and researchers have skewed some research findings.49 The research-based classification systems of the American Psychiatric Association’s “Diagnostic and Statistical Manual of Mental Disorders” (DSM) and the World Health Organization’s (WHO) “International Classification of Disease” (ICD) may also impact health provider attitudes.25 Homosexuality was classified as a mental illness by the DSM until 1973,69 and gender diversity did not appear in the ICD until 1975.70 Currently, gender diversity is classified as “gender dysphoria” by DSM-5 and “gender identity disorder” by ICD-10. In 2022, ICD-11 will adopt the term “gender incongruence” and move it from the “Mental and Behavioural Disorders” chapter to “Conditions Related to Sexual Health.”25 Proponents of current DSM and ICD classifications argue that they minimize stigma, acknowledge psychological stress, and support access to care, including gender-affirming modalities, whereas detractors maintain that gender diversity in and of itself is not a pathology requiring classification.25
Transgender individuals experience harm via government-issued documents, lab work orders, patient records, and coding and billing systems that are founded in hetero- and cis-normative assumptions.71 Identity documentation should first determine the patient’s gender identity, name, and pronouns — which are most important to the patient — and then determine assigned sex and name at birth — which may impact assessment decisions.71 Clinic staff should accept government-issued documentation as presented and not make assumptions when the documentation differs from the patient’s stated identity.71
The increased use and implementation of electronic medical records (EMRs) can constrain or enable gender-affirming care. The World Professional Association for Transgender Health EMR Working Group provides several recommendations.71 There should be an optional field for recording preferred name, gender identity, and pronouns that is separate from the field containing assigned sex and name, needed for billing. Gender identity and pronoun options should be flexible to accommodate changing patient preferences and evolving gender minority taxonomies. The system must be able to flag differences between assigned and preferred identity at the right time for each EMR end-user. Additionally, EMRs must support an updatable anatomy inventory and gender-affirming medical care record (e.g., surgery, hormones) that can auto-populate appropriate workup templates. This information must be decoupled from gender and sex identity fields. Tuite et al.72 also note that the pedigree nomenclature used in some patient records needs updating to represent patients who are gender non-conforming or born with DSD.
Health impacts
Discrimination, stigmatization, rejection, and internalized homophobia and transphobia trigger physiologic responses (e.g., activating the hypothalamic–pituitary–adrenal axis) that contribute to a higher prevalence of internalizing disorders like depression and anxiety as well as externalizing disorders such as substance abuse, self harm, and suicidal ideation and behavior.38,53,73,74 Encouragingly, competent care can reduce the occurrence of mental illness. For example, similar depression rates among cisgender children and gender minority children experiencing gender transition social supports suggest these supports can offset typically higher depression rates among gender minorities.75
Compared with heterosexual peers, LGB adults have higher risks of asthma and cardiovascular disease, bisexual individuals have double the smoking rate, and gay men experience disproportionally higher rates of human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs).76
Transgender people, particularly trans women, face disproportionately higher rates of systemic disease compared with cisgender peers.63 Trans women experience significantly higher rates of HIV and other STIs. If they have pursued gender-affirming hormonal therapy (i.e., estrogens and anti-androgens), they also have higher rates of vascular disease (e.g., venous thrombosis, myocardial infarction, type 2 diabetes, cerebrovascular disease), osteoporosis, and autoimmune disease (e.g., systemic lupus erythematosus and autoimmune hepatitis).63 The latter may be tied to elevated C-reactive protein.77 Thus, a key gender-affirming step of many transgender people — hormonal therapy — may support their mental well-being yet work against some aspects of their physical well-being.
Long-term gender-affirming hormone therapy in trans women may be linked to a higher risk of neuro-ophthalmic disease according to case reports of bilateral non-arteritic anterior ischemic neuropathy and post-surgical cerebral venous sinus thrombosis.78,79 Hollar et al.63 argue that transgender people may be more likely to experience progressive glaucomatous optic neuropathy, diabetic neuropathy, and reduced retinal ganglion cell survival after traumatic optic neuropathy. They suggest that brain-derived neurotrophic factor may play a role and that trans women may more likely be missing this neuroprotective factor.
The increased prevalence of osteoporosis among transgender women taking gender-affirming hormones may elevate their risk of inflammatory conditions of the eye and ocular adnexa (e.g., uveitis, episcleritis/scleritis, optic neuropathy, orbital inflammation).63 Gender-affirming hormone therapy for transgender men may cause idiopathic intracranial hypertension, leading to papilledema and ocular motor dysfunction.
A significantly higher prevalence of HIV infection and increased risk of type 2 diabetes and thromboembolic events among trans women means that eyecare practitioners should consider the greater likelihood of HIV retinopathy, CMV retinitis, other opportunistic retinal infections, diabetic retinopathy, and retinal occlusive disease.63 Higher smoking rates among this community may exacerbate the risk of these retinopathies.80
Gender-affirming hormone therapy may improve (testosterone) or worsen (estrogen) ocular surface disease.81 Optometrists need to also understand that gender-affirming surgery for some individuals includes facial surgical procedures such as eyebrow lifting and hairline lowering that may impact ocular functions.63
These health impacts complicated by notable health disparities necessitate developing a set of competencies for optometrists that considers the diversity of the 2SLGBTQ+ communities.
Competencies for a 2SLGBTQ+ Inclusive Optometry Curriculum
The AAMC “Resource for Medical Educators”29 has created the only comprehensive set of competencies that addresses the care needs of 2SLGBTQ+ communities. Included with each of the 30 AAMC competency objectives are examples of demonstrating the competency and educational modalities that may help students meet the competency. We adapted the AAMC competencies29 for optometric practice using a consensus building approach, which started with a version created by one of us (MMS). Modifications were made through an iterative discussion among the three of us. A similar approach was taken to providing non-exhaustive examples of demonstrating competencies and education modalities. For the latter, we created unique examples that focused on one of four types of learning activities: case, discuss, skill, project.
We determined that all eight AAMC competency domains applied to optometrists. At the specific competency objective level, differences in practice scope triggered some changes. Of the six “patient care” domain competencies, two were altered and one was eliminated. In addition, one of the six “system-based practice” domain competencies was eliminated.
Tables 1 to 8 show the adapted AAMC competencies and related examples across 8 competency objectives: knowledge for practice (Table 1), patient care (Table 2), practice-based learning and improvement (Table 3), interpersonal and communication skills (Table 4), professionalism (Table 5), systems-based practice (Table 6), interprofessional collaboration (Table 7), and personal and professional development (Table 8). For brevity, we did not explicitly identify the patient cohort in each cell unless it pertained to a subset of the 2SLGBTQ+ communities. In doing this work, we recognized the inter-relatedness of aspects of the eight competencies. For example, certain knowledge for practice (Table 1) is required to provide competent patient care (Table 2), which might include specific interpersonal and communication skills (Table 4). The eight competencies and related examples may help optometric educators consider ways to adapt their curricula as needed.
 Table 1. Click to enlarge |
 Table 2. Click to enlarge |
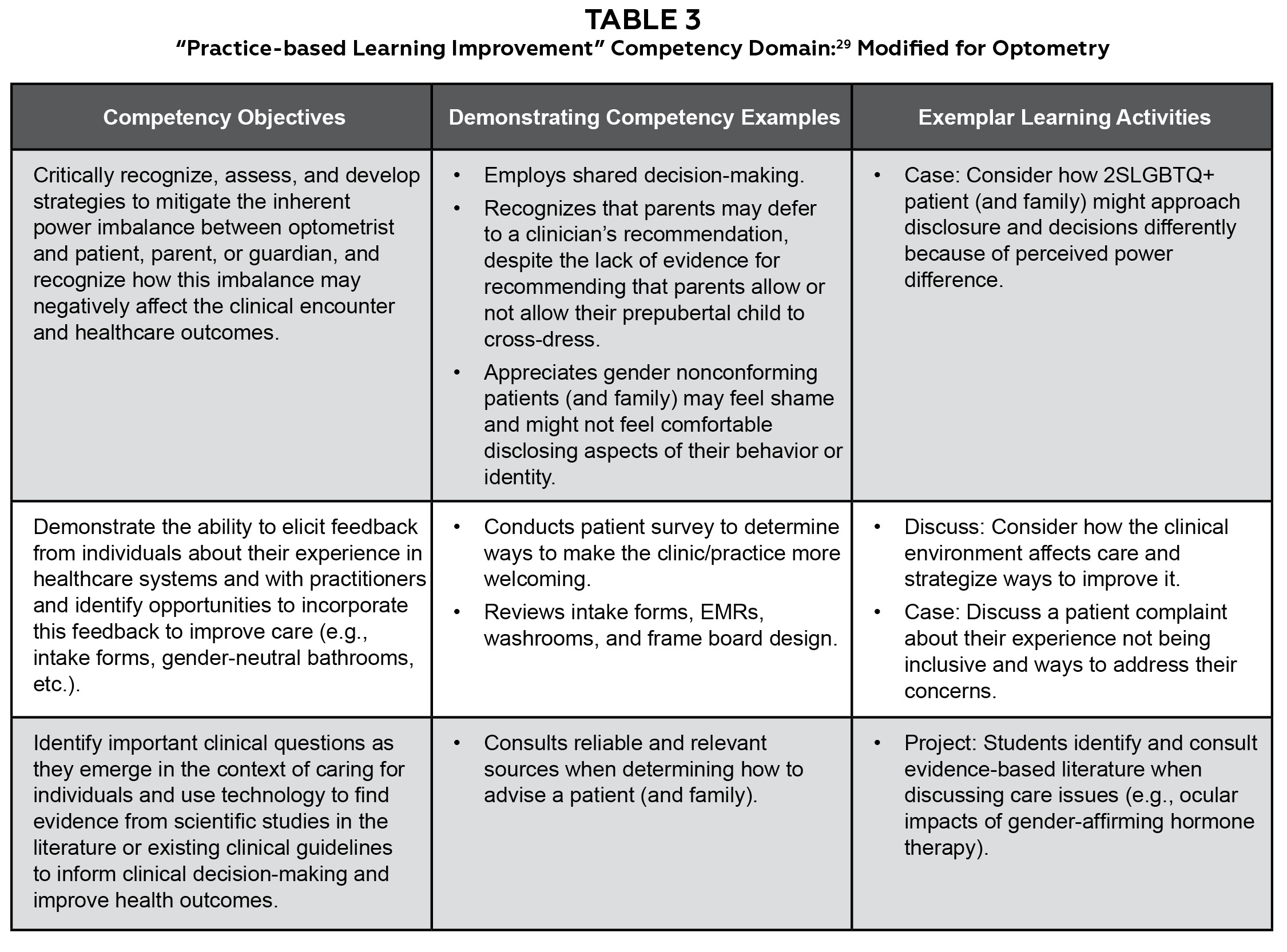 Table 3. Click to enlarge |
 Table 4. Click to enlarge |
 Table 5. Click to enlarge |
 Table 6. Click to enlarge |
 Table 7. Click to enlarge |
 Table 8. Click to enlarge |
Planning for Curricular Change
Integrating competencies that support culturally safe optometric care of patients requires individual, institutional, and system changes. Curtis et al.82 problematize health practitioners and organizations who aim for cultural competence, which has been historically limited to cultural knowledge acquisition by individuals. Instead, cultural safety requires health practitioners, and related organizations and systems, to examine the “potential impact of their own culture on clinical interactions and healthcare service delivery” via ongoing critical consciousness, self-reflection, and accountability.82
While outside the scope of this article on training clinical novices, training for optometric staff and continuing education for optometrists is also needed. Optometric educators and administrators can benefit from guidelines created by other health educators and organizations (e.g., AAMC,83 Egale Canada,84 Gay & Lesbian Medical Association,85 National LGBT Health Education Center,86 The Fenway Institute87). These can be adjusted, where needed, for differences in professional identity, jurisdictional scope of practice, and educational accreditation standards. This work will help optometric educators meet evolving ACOE standards.
Before considering curricular and pedagogical matters, care must be taken to create an institutional climate that supports safety and openness regarding discussions, teaching, learning, and research. Compared with their peers, health students identifying as 2SLGBTQ+ experience increased social isolation and stress, decreased social support, and a degraded emotional environment because of discrimination and bias.29 Attention to creating safe spaces for 2SLGBTQ+ instructors, staff, and students must precede the creation of safe spaces for 2SLGBTQ+ patient care. Evolving a positive climate occurs through institutional engagement (e.g., recruitment, admissions, hiring practices, continuing education, resource centers), inclusive policies and practices (e.g., student and employee orientation, discrimination policies), diversity support (e.g., pride event recognition, employee and resource center support lists), community outreach and engagement (e.g., community partnerships, event hosting), and supportive technologies (e.g., digital presence, culturally sensitive data collection).29
Energy should also be expended to identify and consider potential barriers to creating and delivering 2SLGBTQ+ health curricula. Barriers may include instructor discomfort or unpreparedness to address content; difficulty differentiating core from elective topics, especially in the presence of an already packed curriculum; and student discomfort or unwillingness to engage with topics due to religious, political, or personal beliefs.8,29
In addition to ensuring that educators can competently manage relevant curricular content, Carter et al.88 call upon educators to create what Little and Stubbs have called “a brave space” for educational conversations where bias and phobias exist. Constructive educator strategies include conducting a self-assessment of privilege, bias, prejudice, and stereotype, identifying and challenging system level, historical institutional inequities, role-modeling openness and a willingness to listen, and demonstrating empathy and cultural humility.88 Recognizing that some students may espouse values that could hinder the quality of 2SLGBTQ+ care, educators still need to set clinical competencies to manage diverse student populations.8
In creating 2SLGBTQ+ health curricula, recommended practices call for curricular co-creation that involves 2SLGBTQ+ faculty, staff, students, and patients, scaffolded design, interprofessional opportunities where possible, and competency-based learning objectives.8,29 A curricular mapping process can help identify 2SLGBTQ+ health gaps in current curricula.8 In addition to improving basic knowledge and facilitating clinical preparedness, curricular design needs to enable attitudinal awareness through cultivating values, exploring self-awareness of privilege and bias, and enhancing communication skills.29 Thus, pedagogical approaches that support deep learning, self-awareness, and critical-thinking will be most effective. Towards this end, recommended health profession 2SLGBTQ+ learning activities include self-reflections, group discussions, role plays, standardized patients, and interactions with people who identify as 2SLGBTQ+.5,89 Noonan et al.5 report that standardized patients who identify with the gender they portray are more effective because their lived experiences allow them to authentically play the role and provide constructive feedback to the learner in a safe learning environment. Team-based learning or flipped classrooms that support facilitated class discussions and objective structured clinical examinations that provide a safe environment for demonstrating clinical skills are also advocated pedagogical strategies.5,8 As with all learning environments, learning objectives should be articulated and aligned with learning activities and assessments.90
Conclusion
We have identified a potential gap in optometric education, provided a justification for why it should be addressed, and proposed a set of competencies to help optometric educators review their curricula for any problematic or absent content. A broader discussion and potential modification of these competencies may be warranted for the benefit of training optometry students to provide culturally safe care that considers the unique needs and priorities of patients who identify with the 2SLGBTQ+ communities.
Thus far, the literature about teaching 2SLGBTQ+ patient care has occurred in health settings outside optometry. While this emerging knowledge may translate reasonably well, we encourage research situated in optometry settings to unpack unique elements of optometry’s professional and educational environments. Some clinicians will have limited formal training in the unique and varied care needs of these diverse communities and many more clinicians will lack formal training in teaching specific associated communication skills. Thus, optometry schools and colleges can help students provide culturally safe care to members of 2SLGBTQ+ communities if they offer faculty/clinician training that addresses healthcare needs, critical consciousness, and teaching strategies.
References
- Accreditation Council on Optometric Education. Accreditation Resources and Directories of Programs: Professional Optometric Degree Program Resources [cited Sept 17, 2021]. Available from: https://theacoe.org/resources-and-directories-of-programs?sso=y.
- Canadian Association of Optometrists. Code of Ethics | The Canadian Association of Optometrists [cited June 9, 2021]. Available from: https://opto.ca/code-ethics.
- American Optometric Association. Ethics & Values [cited June 9, 2021]. Available from: https://www.aoa.org/about-the-aoa/ethics-and-values?sso=y.
- Marshall EC, Fink B, Pang Y, et al. ASCO Guidelines for Culturally Competent Eye and Vision Care. 2008 [cited Oct 14, 2021]. Available from: https://optometriceducation.org/files/Guidelines-for-Cult-Com-v2-7-24-2020.pdf.
- Noonan EJ, Sawning S, Combs R, et al. Engaging the transgender community to improve medical education and prioritize healthcare initiatives. Teach Learn Med. 2018;30(2):119-132.
- Butler-Foster T, Butler-Foster T, Chin-Yee I, Chin-Yee I, Huang M, Jackson KT. Toward understanding culturally sensitive care for transgender blood donors: A scoping review of health care provider knowledge. Trans Health. 2020;5(2):104-115.
- Click IA, Mann AK, Buda M, et al. Transgender health education for medical students. Clin Teach. 2020;17(2):190-194.
- Llayton CK, Caldas LM. Strategies for inclusion of Lesbian, gay, bisexual, transgender, queer, intersex, and asexual (LGBTQIA+) education throughout pharmacy school curricula. Pharm Pract. 2020;18(1).
- Nowaskie DZ, Patel AU, Fang RC. A multicenter, multidisciplinary evaluation of 1701 healthcare professional students” LGBT cultural competency: Comparisons between dental, medical, occupational therapy, pharmacy, physical therapy, physician assistant, and social work students. PLoS ONE. 2020;15(8 August).
- Lim FA, Brown Jr. DV, Kim SMJ. Addressing health care disparities in the lesbian, gay, bisexual, and transgender population: A review of best practices. Am J Nurs. 2014;114(6):24-34.
- Englander R, Cameron T, Ballard AJ, Dodge J, Bull J, Aschenbrener CA. Toward a common taxonomy of competency domains for the health professions and competencies for physicians. Acad Med. 2013;88(8):1088-1094.
- Schreiber M, Ahmad T, Scott M, Imrie K, Razack S. The case for a Canadian standard for 2SLGBTQIA+ medical education. CMAJ. 2021;193(16):E562-E565.
- Obedin-Maliver J, Goldsmith ES, Stewart L, et al. Lesbian, gay, bisexual, and transgender-related content in undergraduate medical education. JAMA. 2011;306(9):971-977.
- White W, Brenman S, Paradis E, et al. Lesbian, gay, bisexual, and transgender patient care: Medical students” preparedness and comfort. Teach Learn Med. 2015;27(3):254-263.
- Braun HM, Garcia-Grossman IR, Quiñones-Rivera A, Deutsch MB. Outcome and impact evaluation of a transgender health course for health profession students. LGBT Health. 2017;4(1):55-61.
- Vance SR, Halpern-Felsher BL, Rosenthal SM. Health care providers” comfort with and barriers to care of transgender youth. J Adolescent Health. 2015;56(2):251-253.
- McPhail D, Roundtree-James M, Whetter J. Addressing gaps in physician knowledge regarding transgender health and healthcare through medical education. Can Med Educ J. 2016;7(2):e70-e78.
- Dy GW, Osbun NC, Morrison SD, Grant DW, Merguerian PA. Exposure to and attitudes regarding transgender education among urology residents. J Sex Med. 2016;13(10):1466-1472.
- Morrison SD, Dy GW, Chong HJ, et al. Transgender-related education in plastic surgery and urology residency programs. J Grad Med Educ. 2017;9(2):178-183.
- Sanchez AA, Southgate E, Rogers G, Duvivier RJ. Inclusion of lesbian, gay, bisexual, transgender, queer, and intersex health in Australian and New Zealand medical education. LGBT Health. 2017;4(4):295-303.
- Parameshwaran V, Cockbain BC, Hillyard M, Price JR. Is the lack of specific lesbian, gay, bisexual, transgender and queer/questioning (LGBTQ) health care education in medical school a cause for concern? Evidence from a survey of knowledge and practice among UK medical students. J Homosexual. 2017;64(3):367-381.
- Chisolm-Straker M, Willging C, Daul AD, et al. Transgender and gender-nonconforming patients in the emergency department: What physicians know, think, and do. Ann Emerg Med. 2018;71(2):183-188.e1.
- Beagan, Brenda, Fredericks, Erin, Bryson, Mary. Family physician perceptions of working with LGBTQ patients: physician training needs. Can Med Educ J. 2015;6(1):e14-22.
- Snelgrove JW, Jasudavisius AM, Rowe BW, Head EM, Bauer GR. “completely out-at-sea” with “two-gender medicine”: A qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv Res. 2012;12(1).
- De Vries E, Kathard H, Müller A. Debate: Why should gender-affirming health care be included in health science curricula? BMC Med Educ. 2020;20(1).
- Dubin SN, Nolan IT, Streed CG, Greene RE, Radix AE, Morrison SD. Transgender health care: Improving medical students’ and residents’ training and awareness. Adv Med Educ Pract. 2018;9:377-391.
- Stroumsa D, Shires DA, Richardson CR, Jaffee KD, Woodford MR. Transphobia rather than education predicts provider knowledge of transgender health care. Med Educ. 2019;53(4):398-407.
- Desrosiers J, Wilkinson T, Abel G, Pitama S. Curricular initiatives that enhance student knowledge and perceptions of sexual and gender minority groups: a critical interpretive synthesis. Can Med Educ J. 2016;7(2):e121-e138.
- Hollenbach AD, Eckstrand KL, Dreger AD. Implementing Curricular and Institutional Climate Changes to Improve Health Care for Individuals Who Are LGBT, Gender Nonconforming, or Born with DSD: A Resource for Medical Educators. Association of American Medical Colleges; 2014.
- Denial A, Hoppe E, Carlson N. Assessing cultural competency in optometric faculty. Optom Educ. 2006;31(3):92-95.
- Diversity and Cultural Competency Committee. Case Studies in Cultural Competency. Association of Schools and Colleges of Optometry; 2021:60 [cited Oct 28, 2021]. Available from: https://optometriceducation.org/wp-content/uploads/2021/09/Case-Studies-in-Cultural-Competency.2021.FINAL_.pdf.
- McDowell P, Kalaczinski L. Optometric Care of Transgender Patients. Published 2020 [cited June 9, 2021]. Available from: https://aaopt.org/past-meeting-abstract-archives/?SortBy=&ArticleType=&ArticleYear=&Title=Optometric+Care+of+Transgender+Patients&Abstract=&ArticleAuthor=Paula+McDowell&Affiliation=&PROGRAM+NUMBER=.
- McDowell P, Kalaczinski L. Optometric Care of Transgender Patients. Presentation (PH-05) at the annual meeting of the American Academy of Optometry; Oct. 25, 2019, Orlando, FL.
- Cover R. Populist contestations: Cultural change and the competing languages of sexual and gender identity. Sexualities. 2020;0(0):1-16.
- Pereira C, Sauer J. Connecting Communities: Creating Safe Spaces for 2SLGBTQ+ Students and Staff [cited Oct 31, 2022]. Available from: https://joshsauerpr.com/2020/07/27/connecting-communities-creating-safe-spaces-for-2slgbtq-students-and-staff/.
- Waite S, Denier N. A research note on Canada’s LGBT data landscape: Where we are and what the future holds. Can Rev Sociol. 2019;56(1):93-117.
- Government of Canada SC. Sex and Gender. Published Feb 18, 2019 [cited June 9, 2021]. Available from: https://www12.statcan.gc.ca/census-recensement/2021/road2021-chemin2021/fs-fi/sex-and-gender.cfm.
- Government of Canada SC. Same-Sex Couples and Sexual Orientation … by the Numbers. Published June 23, 2015 [cited June 9, 2021]. Available from: https://www.statcan.gc.ca/eng/dai/smr08/2015/smr08_203_2015.
- Wang H. U.S. Census to Leave Sexual Orientation, Gender Identity Questions Off New Surveys. NPR.org. Published 2017 [cited June 9, 2021]. Available from: https://www.npr.org/sections/thetwo-way/2017/03/29/521921287/u-s-census-to-leave-sexual-orientation-gender-identity-questions-off-new-surveys.
- Centers for Disease Control and Prevention. CDC – BRFSS – Questionnaires. Published August 26, 2021 [cited Dec 17, 2021]. Available from: https://www.cdc.gov/brfss/questionnaires/index.htm.
- Government of Canada SC. Sex at Birth and Gender: Technical Report on Changes for the 2021 Census. Published July 20, 2020 [cited June 9, 2021]. Available from: https://www12.statcan.gc.ca/census-recensement/2021/ref/98-20-0002/982000022020002-eng.cfm.
- Conrad KJ, Goldberg SK. UCLA School of Law Williams Institute. Adult LGBT Population in the United States: July 2020 [cited June 9, 2021]. Available from: https://williamsinstitute.law.ucla.edu/wp-content/uploads/LGBT-Adult-US-Pop-Jul-2020.pdf.
- Woodford M, Coulombe S, Marshall Z, Schwabe N, Krzesni D, Canadian Centre for Gender and Sexual Diversity. Querying Canadian Higher Education: A Snapshot of LGBT+ Students’ Experiences and Mental Health; 2019. Available from: https://lgbtq2sthrivingoncampus.ca/wp-content/uploads/2020/02/NRP-28-Woodford-et-al.-2019-Querying-Canadian-Higher-Education.pdf.
- Gallup Inc. LGBT Identification in U.S. Ticks Up to 7.1%. Gallup.com. Published Feb 17, 2022 [cited Feb 25, 2022]. Available from: https://news.gallup.com/poll/389792/lgbt-identification-ticks-up.aspx.
- Blackless M, Charuvastra A, Derryck A, Fausto-Sterling A, Lauzanne K, Lee E. How sexually dimorphic are we? Review and synthesis. Am J Hum Biol. 2000;12(2):151-166.
- Hatzenbuehler ML, Link BG. Introduction to the special issue on structural stigma and health. Soc Sci Med. 2014;103:1-6.
- Kattari SK, Walls NE, Whitfield DL, Langenderfer-Magruder L. Racial and ethnic differences in experiences of discrimination in accessing health services among transgender people in the United States. Int J Transgenderism. 2015;16(2):68-79.
- Ard K, Makadon H. Improving the Health Care of Lesbian, Gay, Bisexual and Transgender (LGBT) People: Understanding and Eliminating Health Disparities. The National LGBT Health Education Center, The Fenway Institute. Available from: https://www.lgbtqiahealtheducation.org/wp-content/uploads/Improving-the-Health-of-LGBT-People.pdf.
- Brotman S, Ryan B, Jalbert Y, Rowe B. Reclaiming space-regaining health: The health care experiences of two-spirit people in Canada. J Gay Lesbian Soc Serv. 2002;14(1):67-87.
- Ng HH. Intersectionality and shared decision making in LGBTQ health. LGBT Health. 2016;3(5):325-326.
- Mendos LR, Botha K, Carrano Lelis R, Lopez de la Pena E, Savelev I, Tan D. State-Sponsored Homophobia 2020: Global Legislation Overview Update. International Lesbian, Gay, Bisexual, Trans and Intersex Association (ILGA); 2020 [cited June 9, 2021]. Available from: https://ilga.org/downloads/ILGA_World_State_Sponsored_Homophobia_report_global_legislation_overview_update_December_2020.pdf.
- Statistics Canada, Integration and Analysis Program, Canadian Centre for Justice Statistics. Hate Crime in Canada: An Overview of Issues and Data Sources. Statistics Canada, Integration and Analysis Program, Canadian Centre for Justice Statistics; 2001 [cited June 9, 2021]. Available from: https://www150.statcan.gc.ca/n1/en/pub/85-551-x/85-551-x1999000-eng.pdf?st=89oSz_HA.
- Feinstein BA, Goldfried MR, Davila J. The relationship between experiences of discrimination and mental health among lesbians and gay men: An examination of internalized homonegativity and rejection sensitivity as potential mechanisms. J Consult Clin Psych. 2012;80(5):917-927.
- Hendricks ML, Testa RJ. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the minority stress model. Prof Psych: Res Prac. 2012;43(5):460-467.
- Jaffee KD, Shires DA, Stroumsa D. Discrimination and delayed health care among transgender women and men. Med Care. 2016;54(11):1010-1016.
- Samuels EA, Tape C, Garber N, Bowman S, Choo EK. “Sometimes you feel like the freak show”: A qualitative assessment of emergency care experiences among transgender and gender-nonconforming patients. Ann Emerg Med. 2018;71(2):170-182.e1.
- Clark BA, Veale JF, Greyson D, Saewyc E. Primary care access and foregone care: A survey of transgender adolescents and young adults. Fam Pract. 2018;35(3):302-306.
- Lindroth M. “Competent persons who can treat you with competence, as simple as that” – an interview study with transgender people on their experiences of meeting health care professionals. J Clin Nurs. 2016;25(23-24):3511-3521.
- Riggs DW, Coleman K, Due C. Healthcare experiences of gender diverse Australians: A mixed-methods, self-report survey. BMC Public Health. 2014;14(1).
- James S, Herman J, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality; 2016 [cited Oct 21, 2021]. Available from: https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf.
- Javid A, Akram S, Batool A, Afghani T, Sehar G, Manzoor H. Prevalence of ocular findings in transgender and barriers for not reporting to eye hospitals and clinics. Adv Ophthalmol Vis Sys. 2020;10(2):23-27.
- Bakko M, Kattari SK. Transgender-related insurance denials as barriers to transgender healthcare: Differences in experience by insurance type. J Gen Intern Med. 2020;35(6):1693-1700.
- Hollar MW, Zhang MM, Mawn LA. Ophthalmic disparities in transgender patients. Sem Ophthalmol. 2016;31(4):426-431.
- Müller A, Crawford-Browne S. Challenging medical knowledge at the source – attempting critical teaching in the health sciences. Agenda. 2013;27(4):25-34.
- DasGupta S, Fornari A, Geer K, et al. Medical education for social justice: Paulo Freire revisited. J Med Hum. 2006;27(4):245-251.
- Tomson A. Gender-affirming care in the context of medical ethics – gatekeeping v. informed consent. S Afr J Bioethics Law. 2018;11(1):24-28.
- Deutsch MB. Use of the informed consent model in the provision of cross-sex hormone therapy: A survey of the practices of selected clinics. Int J Transgenderism. 2012;13(3):140-146.
- Schulz SL. The informed consent model of transgender care: An alternative to the diagnosis of gender dysphoria. J Humanist Psychol. 2018;58(1):72-92.
- King M, Smith G, Bartlett A. Treatments of homosexuality in Britain since the 1950s—an oral history: the experience of professionals. BMJ. 2004;328(7437):429.
- Beek TF, Cohen-Kettenis PT, Kreukels BPC. Gender incongruence/gender dysphoria and its classification history. Int Rev Psych. 2016;28(1):5-12.
- Deutsch MB, Green J, Keatley J, Mayer G, Hastings J, Hall AM. Electronic medical records and the transgender patient: Recommendations from the world professional association for Transgender Health EMR working group. J Am Med Inform Assoc. 2013;20(4):700-703.
- Tuite A, Dalla Piazza M, Brandi K, Pletcher BA. Beyond circles and squares: A commentary on updating pedigree nomenclature to better represent patient diversity. J Genet Couns. 2020;29(3):435-439.
- Meader N, Chan MKY. Sexual orientation and suicidal behaviour in young people. Brit J Psychiat. 2017;211(2):63-64.
- Delozier AM, Kamody RC, Rodgers S, Chen D. Health disparities in transgender and gender expansive adolescents: A topical review from a minority stress framework. J Pediatr Psychol. 2020;45(8):842-847.
- Olson KR, Durwood L, DeMeules M, McLaughlin KA. Mental health of transgender children who are supported in their identities. Pediatrics. 2016 Mar;137(3):e20153223.
- Institute of Medicine (US) Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. National Academies Press (US); 2011 [cited June 14, 2021]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK64806/.
- Gooren LJ, Kreukels B, Lapauw B, Giltay EJ. (Patho)physiology of cross-sex hormone administration to transsexual people: The potential impact of male-female genetic differences. Andrologia. 2015;47(1):5-19.
- Oster JM, Shastri P, Geyer C. Cerebral venous sinus thrombosis after gender reassignment surgery. Gender Med. 2010;7(3):270-275.
- Wierckx K, De Zaeytijd J, Elaut E, Heylens G, T’Sjoen G. Bilateral non-arteritic ischemic optic neuropathy in a transsexual woman using excessive estrogen dosage. Arch Sex Behav. 2014;43(2):407-409.
- Fallin A, Goodin A, Lee YO, Bennett K. Smoking characteristics among lesbian, gay, and bisexual adults. Prev Med. 2015;74:123-130.
- Sullivan DA, Rocha EM, Aragona P, et al. TFOS DEWS II Sex, Gender, and Hormones Report. Ocul Surf. 2017;15(3):284-333.
- Curtis E, Jones R, Tipene-Leach D, et al. Why cultural safety rather than cultural competency is required to achieve health equity: A literature review and recommended definition. Int J Equity Health. 2019;18(1).
- Association of American Medical Colleges. AAMC Videos and Resources about LGBT Health and Health Care [cited Oct 31, 2022]. Available from: https://www.aamc.org/about-us/equity-diversity-inclusion/lgbt-health-resources/videos.
- Egale – Equal Not Other [cited Sept 29, 2021]. Available from: https://egale.ca/.
- GLMA – GLMA Publications [cited Sept 29, 2021]. Available from: https://www.glma.org/index.cfm?fuseaction=Page.viewPage&pageId=622&parentID=534&nodeID=1.
- National LGBTQIA+ Health Education Center. LGBTQIA+ Health Education Center [cited Sept 29, 2021]. Available from: https://www.lgbtqiahealtheducation.org/.
- Makadon HJ, Mayer KH, Potter J, Goldhammer H (editors). Fenway Guide to Lesbian, Gay, Bisexual, and Transgender Health, 2nd Edition. Philadelphia, PA: American College of Physicians, 2015.
- Carter K, Crewe S, Johner M, McClain A, Sheperis CJ, Townsell S. Educating Health Professions Educators to Address the “isms.” NAM Perspectives, Commentary, National Academy of Medicine, Washington, DC. 2020 [cited Sept 17, 2021]. Available from: https://nam.edu/educating-health-professions-educators-to-address-the-isms/.
- Balbona J, Patel T. The hidden curriculum: Strategies for preparing residents for practice. Curr Urol Rep. 2020;21(10).
- Biggs JB, Tang C. Teaching for quality learning at university: What the student does. [4th ed.] McGraw-Hill/Society for Research into Higher Education; 2011.

