
PEER REVIEWED
Vitamin B12 Deficiency Optic Neuropathy
Amber R. Scharnweber, OD, FAAO, ABCMO, and Richard J. Zimbalist, OD, FAAO
Abstract
Optic neuropathy is a rare complication of vitamin B12 deficiency. Incomplete treatment of vitamin B12 deficiency with oral B12 supplementation coupled with oral folic acid can aggravate neurological impairment secondary to vitamin B12 deficiency if the B12 deficiency is not corrected first. The patient in this teaching case report developed painless, progressive vision loss with temporal optic disc pallor and central scotomas after oral replacement of B12 and folic acid. The patient experienced significant visual recovery after implementation of parenteral B12 therapy followed by oral folic acid supplementation. This teaching case highlights the diagnosis, pathogenesis and treatment of vitamin B12 deficiency optic neuropathy.
Key Words: vitamin B12 deficiency, optic neuropathy, pernicious anemia, folate deficiency, optic atrophy, cobalamin
Background
Vitamin B12 (also known as cobalamin) is an essential vitamin for neurological function. Vitamin B12 deficiency optic neuropathy is a rare complication of this deficiency that results in progressive, bilateral, painless vision loss that is often associated with reduced color vision and central or cecocentral scotomas. The following case report discusses the diagnosis and management of vitamin B12 deficiency optic neuropathy and is appropriate as a teaching guide for third- and fourth-year optometry students as well as optometry residents. The case report explores multiple facets of vitamin B12 deficiency including pathogenesis, epidemiology, manifestations, differential diagnosis and treatment modalities. The role of the optometrist in managing this condition to optimize visual recovery is also highlighted.
Case Description
A 63-year-old Caucasian male presented to the eye clinic for a second opinion regarding cataract surgery in February 2011 following a gradual decline in his vision over the previous two months. He received new glasses from a private provider in December 2010 but continued to experience decreased visual acuity. He was also referred to a private ophthalmologist for cataract surgery, but the procedure was not performed as it was believed that the lenticular changes were not the primary etiology of his visual loss.
 Figure 1A. SITA Standard 30-2 Humphrey Visual Field testing from the initial visit in February 2011 shows central scotoma OD. |
 Figure 1B. SITA Standard 30-2 Humphrey Visual Field testing from the initial visit in February 2011 shows central scotoma OS. |
The patient’s medical history was positive for obesity, nicotine dependence, gouty arthropathy, mild carotid artery stenosis, throat cancer and stomach ulcer. He was status post a December 2004 resection of an oropharyngeal tumor and neck dissection. The stomach ulcer was treated with gastric surgery, date unknown, with resultant pernicious anemia. His current medications included allopurinol 100 mg daily, cyanocobalamin 1000 mcg/mL intramuscularly monthly, folic acid 1 mg daily, and aspirin 81 mg daily. He had an allergy to hydrochlorothiazide, which caused hyponatremia. The patient denied alcohol and recreational drug use. His family history was unremarkable. Recent blood pressure was normotensive at 121/80 mmHg (left arm, sitting) and his calculated BMI was 30.78. Ocular history was only remarkable for recently diagnosed cataracts. The patient was oriented to time, place and person, and his mood and affect were appropriate.
The patient’s entering aided visual acuities were 20/400 OD and 20/400 OS at distance. His current prescription measured OD: +1.75 DS and OS: +2.00 -0.50×049. Pupils were equally round and reactive to light, without an afferent pupillary defect. Extraocular muscles were full without restriction. Confrontation visual fields were full to finger count OD and OS without extinction. Cover test was orthophoric at distance. Subjective refraction was OD: +2.00 DS and OS: +2.00 DS. The subjective refraction did not improve the best-corrected visual acuities. The patient was able to see only the test plate on color vision testing with Ishihara plates OD and OS.
Anterior segment evaluation was unremarkable except for 1+ nuclear sclerotic lenticular opacities in both eyes. Intraocular pressures as measured by Goldmann tonometry were 16 mmHg OD and 16 mmHg OS.
Dilated fundus examination showed distinct, flat optic nerves with cup to disc ratios of 0.5 OD, 0.5 OS and mild temporal optic nerve head pallor in both eyes. The maculae were flat with even pigment, and a positive foveal light reflex was noted in both eyes. The rest of the posterior segment was unremarkable OU.
SITA Standard 30-2 Humphrey Visual Field (HVF) revealed central scotomas OD and OS; however, testing was somewhat unreliable due to fixation losses. The mean deviations were -6.07 dB OD and -4.90 dB OS. (Figure 1) Optical coherence tomography (OCT, Stratus) macular testing was normal, but the scans were off-center with poor signal strength. Retinal nerve fiber layer (RNFL) evaluation with OCT revealed a small wedge of temporal thinning OD and was unreliable OS. The OCT scans were less than optimal due to poor patient fixation and technique.

Table 1.
Click to enlarge
An in-depth chart review revealed that the patient had been diagnosed with vitamin B12 deficiency in October 2010 as a result of routine bloodwork. (Table 1) At that time, he was prescribed vitamin B12 1000 mcg po daily and folic acid 1 mg po daily. The patient’s primary care provider consulted hematology, and treatment was amended in January 2011 to intramuscular cyanocobalamin 1000 mcg/mL once weekly for four weeks and monthly thereafter to be followed by folic acid 1 mg daily po. This change was recommended because incompletely treated vitamin B12 deficiency with oral replacement by folic acid can aggravate the neurological impairment related to B12 deficiency if the B12 is not corrected first. The goal was to ensure vitamin B12 was bioavailable in the presence of any malabsorption issues the patient may have had secondary to the previous gastric ulcer surgery.
The patient was diagnosed with bilateral optic neuropathy due to vitamin B12 deficiency. Magnetic resonance imaging (MRI) of the brain and orbits was ordered to rule out other neurological etiologies.
Follow-up 1: one month after initial presentation
The patient reported his vision was stable. He continued to receive cyanocobalamin 1000 mcg/mL intramuscularly. The MRI of the brain and orbits was unremarkable. His best-corrected visual acuity remained 20/400 OD and 20/400 OS and he was only able to see the test plate of the Ishihara color vision test OD and OS. The patient refused repeat HVF testing at this visit. Repeat RNFL OCT testing revealed stable temporal thinning OD and was unreliable OS. The plan was to continue intramuscular supplementation with cyanocobalamin.
Follow-up 2: five months after initial presentation

Figure 2.
Click to enlarge

Table 2.
Click to enlarge
The patient reported his vision had improved slightly since his last exam. He continued to receive cyanocobalamin 1000 mcg/mL intramuscularly. His best-corrected visual acuity improved to 20/80 OD and 20/80-2 OS. His color vision had also improved to 2/8 OD and 4/8 OS with Ishihara plates. HVF SITA Fast 24-2 revealed improved central defects with mean deviation OD: -1.57 dB and OS: -2.65 dB. (Table 2) Visual field testing was modified to the shorter 24-2 to improve patient cooperation.
Follow-up 3: nine months after initial presentation
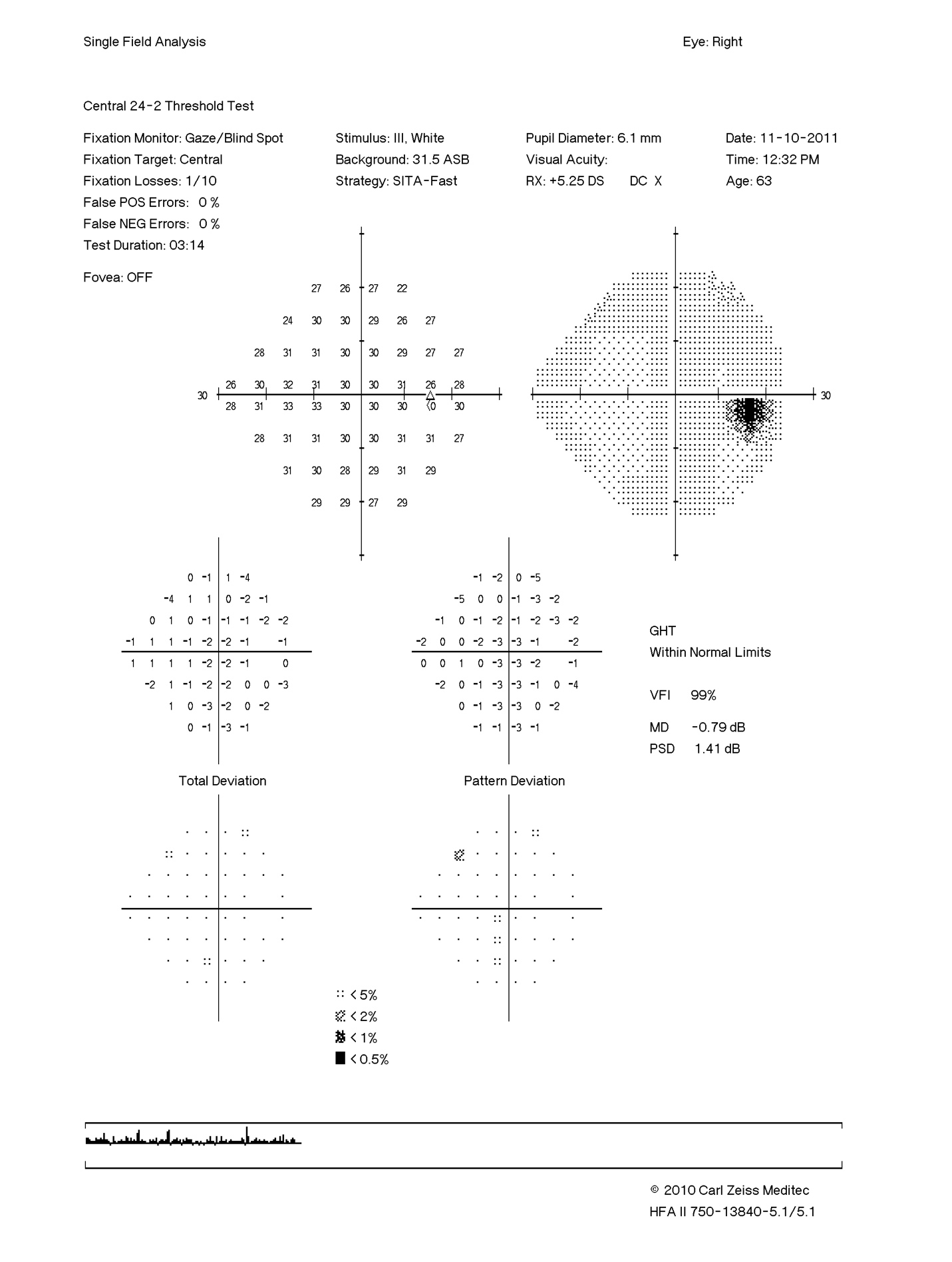 Figure 3A. SITA Standard 24-2 Humphrey Visual Field testing OD from the patient’s final visit in November 2011 shows a clear visual field. |
 Figure 3B. SITA Standard 24-2 Humphrey Visual Field test results OS from the patient’s final visit in November 2011. Note the improvement in the central scotoma compared with initial testing as seen in both the threshold and pattern deviations. |
 Figure 4. Cirrus HD-OCT RNFL imaging from Nov. 10, 2011 (10 months after the change in therapy by hematology). |
The patient continued to report visual improvement and was able to get his driver’s license reinstated. He continued to receive cyanocobalamin 1000 mcg/mL intramuscularly, and his serum B12 and folate levels had noticeably improved from baseline. (Figure 2) His best-corrected visual acuity was 20/40- OD and 20/80- OS. His color vision had improved to 5/8 OD and remained stable at 4/8 OS with Ishihara plates. HVF 24-2 testing revealed a clear visual field OD and a stable central scotoma OS. (Figure 3) Mean deviations were OD: -0.79 and OS: -2.87. RNFL OCT testing (Cirrus HD-OCT 4000) revealed temporal and inferior thinning OD and OS. (Figure 4) It was also noted that the patient had developed a posterior subcapsular cataract in his left eye. The funduscopic views of the left eye were decreased consistent with the cataract formation, thus the cataract was likely also limiting the patient’s best-corrected visual acuity. The patient was instructed to continue the cyanocobalamin injections and return in six months for follow-up. Unfortunately, he passed away in February 2012. The cause of death was unknown.
Education Guidelines
Key concepts
- Understand the systemic causes of vitamin B12 deficiency
- Understand the systemic and ocular manifestations of vitamin B12 deficiency
- Recognize the additional testing necessary to identify the cause of optic neuropathy and the importance of reviewing the medical record and history
- Understand the treatment of vitamin B12 deficiency
- Understand the importance of collaborating with other health professionals in managing vitamin B12 deficiency optic neuropathy
- Understand the need to investigate further if the clinical picture does not match the best-corrected visual acuity
Learning objectives
At the conclusion of this case discussion, participants should be able to:
- Describe the ocular presentation of toxic/nutritional optic neuropathy
- Describe additional testing that can be performed to confirm the diagnosis of optic neuropathy
- Understand the pathogenesis of vitamin B12 deficiency optic neuropathy
- Describe treatment and team management for vitamin B12 optic neuropathy
- Identify differential diagnoses that can present with similar findings to B12 deficiency optic neuropathy
Discussion questions
- What are the demographics of vitamin B12 deficiency and vitamin B12 deficiency optic neuropathy?
- What are the classic systemic signs and symptoms of vitamin B12 deficiency?
- What is the ocular presentation of vitamin B12 deficiency?
- What are the differential diagnoses for vitamin B12 deficiency optic neuropathy?
- How is vitamin B12 deficiency optic neuropathy treated?
- Why is it important to treat vitamin B12 completely before supplementing with oral folic acid?
- What is the visual prognosis and limitations for visual recovery from vitamin B12 deficiency optic neuropathy?
- How would you further evaluate the effect of cataract on a patient’s best-corrected visual acuity?
- How could this case have been handled differently?
Learning assessment
- Facilitate case discussion to achieve learning objectives
- Clinical skills can be tested via practicum of visual field, OCT and fundus photography
- Knowledge base can be assessed by comparison of normal and abnormal visual fields, OCTs, fundus photos and MRI
- Knowledge base can be assessed by student presentations of differential diagnoses or written theoretical case examples
Discussion

Table 3.
Click to enlarge
Vitamin B12 is one of eight components of the vitamin B complex. It plays a key role in DNA synthesis, maintaining normal brain function, protein metabolism and erythropoiesis.1 The best sources of vitamin B12 are eggs, milk, cheese, meat, fish, shellfish and poultry.1,2 The recommended daily requirement is 6-9 mcg. Most individuals in developed countries consume this amount. The liver can store approximately 500 times the recommended daily allowance; therefore, vitamin B12 deficiency due to dietary insufficiency alone is quite rare.1
Acquired conditions, such as pernicious anemia, also cause inadequate absorption of B12. Pernicious anemia is a condition in which the body does not produce enough red blood cells due to decreased intrinsic factor, a glycoprotein secreted by the stomach. Intrinsic factor is commonly reduced in atrophic gastritis, autoimmune diseases, and secondary to gastric surgery. Table 3 lists additional etiologies that can contribute to an acquired vitamin B12 deficiency.
Pathophysiology of B12 deficiency
Vitamin B12 has several vital roles in the body. It contributes to the formation of methionine, an important part of DNA synthesis in cells that undergo rapid turnover, including those of the hematopoietic system and of the enteric lining that produces intrinsic factor. A deficiency in vitamin B12 can lead to megaloblastic erythropoiesis, a form of anemia that is characterized by large red blood cells that fail to divide via mitosis. Additionally, vitamin B12 plays a crucial role in limiting the amount of plasma homocysteine, which in high amounts can lead to endothelial cell toxicity.1 Vitamin B12 deficiency also leads to elevated levels of methylmalonyl CoA, which interferes with fatty acid synthesis and contributes to abnormal myelin formation.
Of particular relevance to this case report, vitamin B12 acts as a cofactor in the formation of succinyl CoA, an integral part of the Krebs cycle that ultimately produces adenosine triphosphate (ATP).3 This impaired oxidative metabolism causes a depletion of ATP. Due to the high metabolic demand of the papillomacular bundle in the retina, it is believed that this depletion of ATP damages these sensitive papillomacular bundle fibers resulting in the commonly noted bitemporal optic nerve atrophy and cecocentral scotoma seen in B12 deficiency optic neuropathy.4
Epidemiology
The prevalence of vitamin B12 deficiency increases with age, and it is estimated that 10% of people over age 75 have the disease with 10% also having coexistent folate deficiency.5 Deficiencies in both vitamin B12 and folate result in megaloblastic anemia, but only the vitamin B12 deficiency causes neurological impairment.6 Vitamin B12 and folic acid are intertwined biochemically.1 Folic acid can minimize the hematological abnormalities of vitamin B12 deficiency, but not the neurological symptoms. Folic acid supplementation has also been shown to cause more rapid progression of neurological symptoms if vitamin B12 is not bioavailable or the B12 deficiency is not treated first.7
Manifestations of B12 deficiency
The classic neurological symptoms caused by vitamin B12 deficiency consist of a subacute combined degeneration and diffuse demyelination of the posterior and lateral spinal columns resulting in extremity numbness, weakness and loss of vibratory sense.6,8 The neuropathy is usually symmetrical and patients may present with ataxia, spasticity, hyperactive knee and ankle jerks, and even urinary and fecal incontinence.6,8 Similar pathological changes can occur in the cerebral hemispheres due to a defect in myelin formation that is not completely understood.5,6,8,9 Other systemic manifestations of B12 deficiency include generalized pallor, tachycardia, fatigue, palpitations, megaloblastic anemia, unexplained neurological symptoms (i.e., dementia, sensory ataxia, personality changes, loss of positional sense) and osteoporosis.6
Optic neuropathy secondary to vitamin B12 deficiency occurs in less than 1% of B12 deficient patients.5 It results in progressive, bilateral, painless vision loss that is often associated with reduced color vision and central or cecocentral scotomas. The optic nerve may appear normal in the early stages of disease until optic atrophy develops. In approximately 30% of cases, the visual deficiencies precede other neurological and hematological signs often due to the presence of folic acid.7 Optic nerve head involvement (in the form of optic atrophy) is rare, but can lead to significant visual decline.10
Diagnosis of B12 deficiency
Serum vitamin B12 is the most frequently ordered laboratory test when a patient’s history is suggestive of vitamin B12 deficiency. It is important to note, however, that a low concentration of vitamin B12 only indicates a short-term imbalance. Short-term imbalances will normalize quickly by the ingestion of a well-balanced meal with an emphasis on meat and dairy products. Interestingly, studies have shown that up to 5% of individuals can have normal vitamin B12 levels when they are, in fact, deficient.11
Diagnosing B12 deficiency can be difficult based on serum B12 levels alone. Deceitfully normal levels can be seen in hepatic disorders, and falsely low levels can be seen in folate deficiency and pregnancy.4,12 It is helpful to measure methylmalonate and homocysteine, which are precursors in the B12 pathway, as 85% of patients with B12 deficiency will have elevated levels of these compounds.4 This is particularly useful when the B12 level is in the low- to borderline-low range.4 Additionally, a complete blood count with an elevated mean corpuscular volume (MCV) over 110 fl is also suggestive of vitamin B12 deficiency and warrants further testing.13
Evaluation of a patient with progressive vision loss in the presence of bilateral optic atrophy with central or cecocentral scotomas should include a detailed history including family and dietary backgrounds. The evaluation should include a thorough ophthalmic examination including careful pupillary examination, automated visual field assessment, color vision testing and OCT analysis. MRI of the brain and orbits is required to rule out compressive, ischemic, inflammatory, demyelinating and/or infiltrative etiologies. Laboratory testing should also be performed to rule out B12 deficiency.
Differential diagnosis for B12 deficiency optic neuropathy

Table 4.
Click to enlarge

Table 5.
Click to enlarge
Optic neuropathy refers to any condition in which the optic nerve is damaged. A targeted history and thorough ophthalmic examination is necessary to narrow down a list of probable diagnoses. Progressive, painless, bilateral loss of vision and temporal optic atrophy with central or cecocentral scotomas are signs and symptoms seen in a handful of miscellaneous optic neuropathies. These optic neuropathies can be further isolated with appropriate laboratory testing, imaging studies and a detailed patient history. While this list is not exhaustive, the most common differential diagnoses (Table 4) are:
- Compressive optic neuropathy can occur from any intraorbital mass and is most easily diagnosed with MRI. Similarly, infiltrative optic neuropathies are best diagnosed with neuroimaging and cerebrospinal fluid and/or vitreous analysis.4,14
- Leber’s hereditary optic neuropathy is maternally inherited and usually found in young men age 15-30. Diagnosis is confirmed by genetic testing for the primary mutations: 11778, 3460, 15257 and 14484.4 Dominant optic atrophy most commonly manifests by six years of age and can be diagnosed with genetic testing for the OPA1 gene on whole blood.4,14
- Radiation optic neuropathy typically develops one to five years after radiation therapy for the eye, orbit, sinus, nasopharynx or brain and can be detected on MRI.14
- Toxic optic neuropathy can result from numerous substances. (Table 5) Identification of the suspected toxin should be performed through blood serum and urinalysis. Tobacco-induced optic neuropathy has been controversial for several years. The mechanism of action has not been determined, but it is thought to be multifactorial.9 There is also a theory that vitamin B12 may play a role as tobacco itself may interfere with the absorption of B12.9
Treatment of B12 deficiency
Vitamin B12 deficiency has traditionally been treated with intramuscular injections at a dosage of 1 mg weekly for eight weeks followed by 1 mg monthly for life or until the underlying etiology is eliminated.15 Oral and nasal B12 formulations came to the market several years ago and offer a suitable alternative to parenteral dosing; however, they require greater patient compliance. As mentioned above, incompletely treated vitamin B12 deficiency with oral replacement of folic acid can actually aggravate the neurological impairment related to B12 deficiency if the B12 deficiency is not corrected first.
This paper presents a rare case of partial visual recovery following vitamin B12 deficiency optic neuropathy. Most reports in the literature describe expectations for visual recovery from vitamin B12 deficiency optic neuropathy as guarded, citing time to diagnosis and treatment as the primary limiting factors.7,9,10,16 Improvement of visual symptoms is greatest with early and aggressive therapy.3 Interestingly, this patient recovered vision despite the presence of optic nerve pallor. In most circumstances, visual recovery does not occur once axonal loss has ensued and optic nerve pallor has formed.
Conclusion
This case report is intended to educate eyecare providers on the presentation and management of vitamin B12 deficiency optic neuropathy. It highlights the clinical importance of careful history, ophthalmic examination and use of ancillary testing. Since the advent of bariatric surgery, the importance of ophthalmic surveillance in the presence of vitamin deficiencies has been more frequently discussed in the literature.16 Additionally, Turkyilmaz et. al found that temporal quadrant retinal nerve fiber layer thickness correlates with plasma vitamin B12 levels.17 Eyecare providers should look beyond the eye and order appropriate lab work in light of pertinent ocular findings and be cognizant that incompletely treated vitamin B12 deficiency with oral supplementation with folic acid can aggravate neurological symptoms. Prompt diagnosis and recognition of vitamin B12 deficiency optic neuropathy is paramount to visual recovery.
References
- Schrier SL. Physiology of vitamin B12 and folate deficiency. In: UpToDate, Motil, KJ (Ed), UpToDate, Waltham, MA. Accessed June 1, 2016. Available from: https://www.uptodate.com/contents/physiology-of-vitamin-b12-and-folate-deficiency
- Food sources of vitamin B12 [Internet]. Dietitians of Canada; c2014 [cited 2014 May 6]. Accessed June 29, 2016. Available from: https://www.dietitians.ca/Your-Health/Nutrition-A-Z/Vitamins/Food-Sources-of-Vitamin-B12.aspx
- Orssaud C, Roche O, Dufier JL. Nutritional optic neuropathies. J Neurol Sci. 2007;262:158-64.
- Chan, JW. Optic nerve disorders: diagnosis and management. New York, NY: Springer Science+Business Media, LLC; 2007.
- Lennihan L, Rowland LP. Nutritional disorders: malnutrition, malabsorption, and B12 and other vitamin deficiency. In: Merritt’s Neurology 12th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2010.
- Schrier SL. Etiology and clinical manifestations of vitamin B12 and folate deficiency. In: UpToDate, Mentzer, WC (Ed), UpToDate, Waltham, MA. Accessed Oct. 6, 2015. Available from: https://www.uptodate.com/contents/etiology-and-clinical-manifestations-of-vitamin-b12-and-folate-deficiency
- Mindel JS. Vitamins. In: Duane’s Ophthalmology 12th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2013.
- Phillips PH. Toxic and deficiency optic neuropathies. In: Walsh & Hoyt’s Clinical Neuro-Ophthalmology 6th Edition. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
- Stojsavlijevic N, Levic Z, Drulovic J, Dragutinovic G. A 44-month clinical brain MRI follow-up in a patient with B12 deficiency. Neurology. 1997 Sep;49(3):878-81.
- Larner AJ. Visual failure caused by vitamin B12 deficiency optic neuropathy. Int J Clin Pract. 2004;58:977-78.
- Naurath HJ, Joosten E, Riezler R, Stabler SP, Allen RH, Lindenbaum J. Effects of vitamin B12, folate, and vitamin B6 supplements in elderly people with normal serum vitamin concentrations. Lancet.1995 Jul 8;346(8967):85-9.
- Metz J, McGrath K, Bennett M, Hyland K, Bottiglieri T. Biochemical indices of vitamin B12 nutrition in pregnant patients with subnormal serum vitamin B12 levels. Am J Hematol. 1995 Apr;48(4):251-5.
- Schrier SL. Diagnosis and treatment of vitamin B12 and folate deficiency. In: UpToDate, Mentzer, WC (Ed), UpToDate, Waltham, MA. Accessed May 31, 2016. Available from: https://www.uptodate.com/contents/diagnosis-and-treatment-of-vitamin-b12-and-folate-deficiency
- Ehlers JP. The Wills Eye Manual: office and emergency room diagnosis and treatment of eye disease: 5th edition. Baltimore, MD: Lippincott Williams & Wilkins; 2008.
- Langan RC, Zawistoski KJ. Update on vitamin B12 deficiency. Am Fam Physician. 2011 Jun 15;83(12):1425-30.
- Sawicka-Pierko A, Obuchowsak I, Hady RH, Mariak Z, Dadan J. Nutritional optic neuropathy following bariatric surgery. Wideochir Inne Tech Maloinwazyjne. 2014 Dec;9(4):662-6.
- 17. Turkyilmaz K, Oner V, Turkyilmaz AK, Kirbas A, Kirbas S, Sekeryapan B. Evaluation of peripapillary retinal nerve fiber layer thickness in patients with vitamin B12 deficiency using spectral domain optical coherence tomography. Curr Eye Res. 2013 Jun;38(6):680-4.

