
PEER REVIEWED
Facilitators and Barriers of Clinical Learning in Optometry: A Qualitative Study in a Low-Resource Setting
Boaz Mucunguzi, Moreen Tumwine, Walker Guti, Ian Munabi, Sarah Kiguli, Arild Raaheim, Aloysius G. Mubuuke
Abstract
Background: There is a scarcity of studies on clinical training in optometry training programs especially in low-income countries. This study set out to explore the facilitators and barriers to optometry students’ clinical learning within a low-income country.
Methods: This qualitative study used in-depth interviews with 16 undergraduate optometry students.
Results: Supportive environment, exposure to a variety of cases, and hands-on practice facilitated students’ clinical learning while restriction on areas of hands-on practice, negative attitudes from staff, and limited space were barriers.
Conclusion: The importance of a supportive learning environment together with hands-on practical opportunities is consistent with the social constructivist theory of learning.
Keywords
Background
Visual impairment (VI) is a global challenge1 with about 2.2 billion people living with some form of VI.2 Of these, 80% of near VI is in sub-Saharan Africa3 while distance VI in low- and middle-income regions is four times higher than in high-income regions.1 A shortage in human resources for eye health is a huge burden in sub-Saharan Africa.4 For example, Uganda’s population of over 40 million is served by 40 ophthalmologists.5 To respond to the need, in 2014 Uganda introduced a 4-year undergraduate optometry degree program at Makerere University to train optometrists and the first cohort graduated in 2019.
Globally, the optometry degree program takes a duration of 4 to 6 years6 and includes a combination of both theoretical and clinical modules.7 At Makerere University, students undergo an intensive clinical training (CT) in the eye clinic at Mulago National Referral and Teaching Hospital (MNRTH), optometric teaching clinic, and Makerere University hospital for 8 weeks at each site during their fourth year. According to their optometry curriculum, the CT aims at developing optometry students’ clinical skills such as history taking; observation abilities; performance of a comprehensive eye examination including preliminary screening, refraction, binocular vision assessment; ocular health assessment; and formulation of a comprehensive and shared management plan. This aim of CT targets level three (applying) of the lowest three levels, and the highest three levels (analyzing, evaluating and creating) of the revised Bloom’s taxonomy.8
The aim of CT in health professions education is to incorporate theory and practice in a controlled setting to enable students to learn appropriate behaviors, skills, and attitudes.9 In optometry training programs, clinical learning (CL) involves students giving complete care of patients under the supervision of an optometrist for a given period of time towards the end of their training.10 Constructivism is the philosophical principle underpinning CL.11 But also, CL occurs in a social milieu of the clinical environment characterized by interaction between students themselves, supervisors, patients and caretakers.12 Hence CL can be explained by the social constructivist theory of learning.13
A clinical learning environment (CLE) that is without fear and inspires respect for the students14 stimulates students’ development of self-confidence and competence.15 Importantly, where students are adequately prepared and supported, engagement in clinical settings leads to valuable learning.10 A study by Denial and colleagues16 shows that feedback and supervisor demeanor (insightful, friendly, and respectful) are behaviors that contributed most toward increasing students’ clinical confidence. In Uganda, undergraduate medical students perceived MNRTH as having good learning opportunities because of the large number of patients, wide case mix and unrestricted access to patients.17
On the other hand, supervisor demeanor (negative qualities such as being close-minded, unreceptive, or yelling) contributed least to students’ confidence levels.16 Inadequate guidance and supervision, inadequate equipment, higher numbers of student teacher ratio, lack of resources, and theory-practice gap can negatively affect the quality of learning in the CLE.12,18,19 Also, inadequate workplace affordances, few opportunities for students’ participation, lecturers’ inappropriate approaches to clinical teaching17 and overcrowding20 have been identified as challenges to CL within low resource settings.
Several studies on CT have concentrated on students in medical and nursing education, leaving scarcity in optometry training programs especially in low- and middle-income countries. With the known disparities in employment settings, scope of practice, and clinical supervision models, discoveries from these disciplines may not be so easily applied to the optometry profession.21 Therefore, this study set out to explore possible facilitators and barriers to optometry students’ learning in a CLE at MNRTH in Uganda.
Methods
Study design: This was an exploratory qualitative study involving all the 16 undergraduate fourth year optometry students at Makerere University in Uganda during second semester of the 2022/2023 academic year. Participants were selected because they had undergone CT and thus suitable to provide an in-depth understanding of the possible facilitators and barriers to CL. Data was collected using one-on-one face-to-face in-depth interviews at the end of the 8 weeks of students’ clinical rotation at MNRTH.
Study setting: MNRTH is located on Mulago Hill in the north of Kampala Capital City, west of the university’s college of health sciences. It is the largest hospital within the country. The hospital is approximately 1.8 km from the college campus.17 The eye clinic is located south of MNRTH at level 5 of block H. It is staffed by eye care professionals employed by the hospital as well as faculty members from college of health sciences. The eye clinic offers comprehensive eye examinations, vision testing, diagnosis and treatment of eye conditions, and pre- and postoperative care.
Data collection and analysis: Participants willingly created appointments indicating time and place of convenience where the interviews would be conducted from. They were followed up with a phone call 1 day prior to the interview for a reminder. In-depth interviews were conducted from isolated places to maintain privacy and confidentiality. The interviewer initially asked open-ended questions that were followed by more probing questions with subsequent questions derived from the interviewee’s response.22 The questions had two main areas of focus, the first explored the learning opportunities (facilitators) and the second, barriers (hindrances) to CL. The interviews lasted 30-45 minutes and were audio recorded and later transcribed verbatim. Data saturation was achieved after 12 interviews. This was the point where no new information was coming up from the participants’ responses. Four more participants were added to confirm data saturation and to make sure that no information was left behind. Inductive thematic analysis was used to analyze the qualitative data.22 Data collection and analysis were done concurrently. Data was analyzed by three members separately, and they met frequently to discuss and reach a consensus on the findings.
Data quality control and rigor: To ensure credibility, an experienced research assistant with knowledge in qualitative techniques and interviewing was recruited to conduct the interviews while the principal investigator was taking notes of the interactions. The ideas raised from the audios, transcripts and notes were used to plan for the subsequent interviews. This iterative process of reviewing earlier interviews helped the team to identify areas where additional probing or clarification might be beneficial while maintaining the consistency of the core questions. To provide reflexivity, the principal investigator, a graduate optometrist who was training in health professions education recruited two data analysts who had no knowledge of CT. They gave their views through data collection and analysis to minimize bias.
Ethical considerations
Approval was granted by the School of Medicine Research and Ethics Committee (SOMREC) of the university. Participation in the study was voluntary and written informed consent was obtained from all participants. All methods for data collection were performed according to the guidelines and regulations of the Declaration of Helsinki.
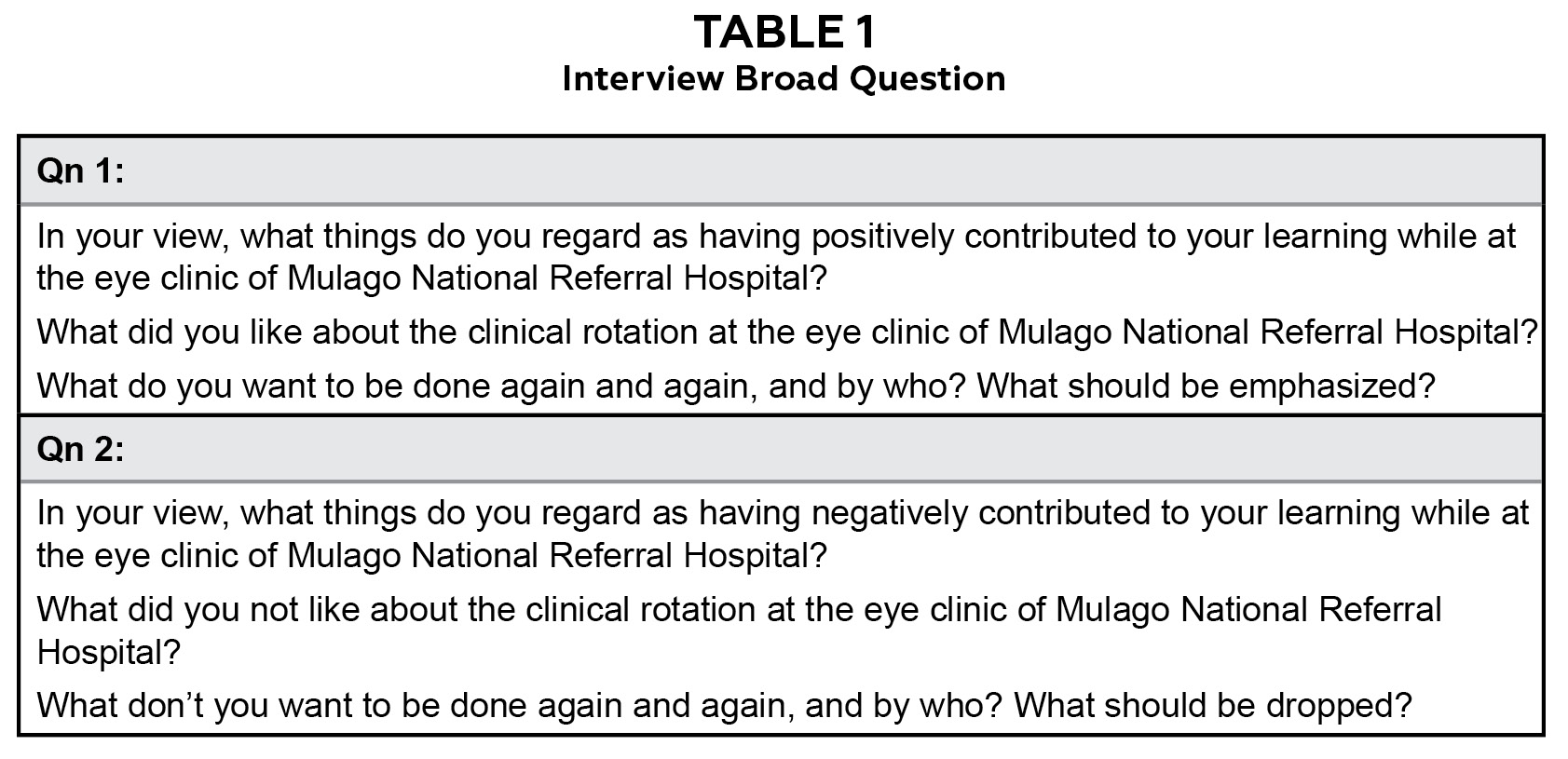
Table 1. Interview Broad Questions. Click to enlarge
RESULTS
Demographics Information
The study comprised of 16 participants with seven females and nine males. Thirteen of these were between 21-25 years. 81% (n=13) of the participants held a higher secondary school certificate while 19% (n=3) possessed a diploma in ophthalmic clinical medicine, as their highest level of education prior to joining the undergraduate optometry degree program.
Themes that emerged from the data
One theme with two corresponding sub-themes emerged from the qualitative data.
Theme: Learning in the clinical environment at the eye clinic of MNRTH.
Sub theme 1: Facilitators of clinical learning at the eye clinic of MNRTH.
Participants appreciated the many opportunities for learning such as the hands-on practice, real-life application of knowledge when working with patients, and observation as well as explanation from experienced professionals. Students labelled these as important methods of learning during their CT.
We learned from their expertise because whenever a doctor saw a case, they briefly explained it and worked as we observed (Participant N).
Working with a real patient who is experiencing vision problems is different from just practicing on artificial models or inducing errors on fellow students (Participant P).
Respondents reported that the CLE at the eye clinic was highly collaborative and supportive. They highlighted the support from their supervisors, fellow students, and positive interactions with some hospital staff as to have significantly facilitated their CL.
Our supervisor was very approachable and always willing to explain things (Participant G).
We discuss, exchange views and learn from one another’s experiences (Participant I).
Participants emphasized the importance of timely feedback that helped them to reflect, identify areas of improvement, and refine their skills. They received feedback from ophthalmologists, nurses, lecturers, optometric interns, fellow students and in logbooks.
After examining a patient and presenting the findings, we receive feedback right then and there. They review our work and identify any mistakes or areas of improvement (Participant I).
Our supervisors sign our logbooks, and they also comment (Participant J).
Optometry students emphasized the exposure to a variety of cases as to have greatly enhanced their CL. They mentioned that they encountered a wide range of eye conditions, some of which were complex, unique, and uncommon which helped to expand their clinical knowledge.
Being in a national referral, we were exposed to diverse and complex cases, including cancers and severe traumas (Participant H).
I was exposed to working with different age groups and understanding their specific needs (Participant E).
A majority (88%) of the respondents mentioned that positive patient interactions during their CT enhanced their confidence, clinical skills and knowledge which improved as they saw more patients. Respondents mentioned that patients were generally compliant and receptive to the care provided.
The patients were obedient, making it easier for me to work with them (Participant H).
I became more proficient in performing accurate refractions and conducting visual acuity tests for children (Participant N).
The lack of performance-related pressure and strict time constraints enabled students to learn at their own pace and spend ample time with patients. They expressed that they had sufficient time to comprehensively grasp each case.
The absence of pressure enabled us to take our time and learn at our own pace, ensuring a more comprehensive understanding of each case (Participant L).
We had ample opportunities to practice and interact with patients, which allowed us to see and touch, gaining a deeper understanding of the conditions we encountered (Participant E).
Sub-theme 2: Barriers of clinical learning at the eye clinic of MNRTH.
Fourteen respondents mentioned that they felt that their hands-on practice was restricted to refraction and they were not utilized to their full potential. They showed concern over the lack of chance to practice all aspects of knowledge and skills that were covered in class.
Despite having covered a variety of eye conditions and procedures, we were only seen as specialized in refraction (Participant A).
This limitation restricts our exposure to certain diagnostic procedures and techniques (Participant F).
Some participants were affected by negative attitudes from some hospital staff within the eye clinic. They mentioned instances where they were made to feel inferior and neglect of their opinions.
While we were open to listening to their views, they were not as willing to listen to ours, which created a bit of a challenge in terms of effective communication and collaboration (Participant D).
…we say our perspectives or insights to make a contribution to the case. However, encountering individuals who dismiss or disregard our opinions without giving them the recognition they deserve was frustrating (Participant C).
Respondents mentioned missing out on learning opportunities due to the small space in consultation rooms compared to a big group of students undergoing clinical rotation in ophthalmology. Overcrowding made it difficult to observe and participate in all cases.
The larger group size may result in difficulty hearing or fully observing certain aspects of the clinical procedures or discussions (Participant H).
The limited space in the consultation rooms made it difficult for all the students to be present during consultations (Participant F).
Some participants faced the challenge of language barrier when communicating with patients who didn’t speak English. Some were not citizens and others were from different regions of the country which made it hard for them to speak or understand the common local language used by the patients at the eye clinic.
Luganda was not a language that I was familiar with, and it posed difficulties when communicating with patients who didn’t speak English (Participant P).
As a foreign student, it can be difficult to gather information about their condition and understand their needs (Participant O).
Limited availability of some equipment hindered optometry students’ learning in certain areas. For example, respondents mentioned that failure to access the slit lamp biomicroscope limited their practice and skill development in using the instrument.
We couldn’t use the slit lamp for learning purposes, even though it’s an important tool for optometry (Participant K).
There is a lack of specific tools and a child-friendly environment to effectively examine young children in the optometry section (Participant A).
Although participants noted positive patient interactions, some mentioned to have faced challenges with complex cases, demanding patients, and those specific to patients of different age groups such as the elderly and children.
Children can be more difficult to handle… may exhibit fear or resistance during examinations. They may cry or become uncooperative (Participant A).
Discussion
The purpose of this study was to explore the facilitators and barriers to CL among optometry students in CT at the eye clinic of MNRTH in Uganda. Key findings are consistent with previous research carried out at MNRTH with medical students,17 and healthcare providers and administrators.20
Findings from the current study demonstrate that CT at the eye clinic offers optometry students with the chance to see and to do real life cases in the presence of experienced supervisors which provides learning opportunities completely different from a classroom or simulated setting. The opportunities are enhanced by a good supervisor-student relationship which greatly encourages students to feel comfortable and to be without fear because of the confidence that the expert would not only correct the mistake but also guarantee the safety of the patient. These findings are consistent with the study by Kirkman10 where optometry students saw the clinical rotations as opportunities to try the everyday reality of work and supervisor-student relationship as an important factor in their placement.
This study shows that surrounding students with supportive individuals from faculty, hospital staff, patients and peers create a safe CLE where students can rely on these individuals as critical pillars playing a key role as mentors and advisors. Such support ensures that students receive timely feedback which in turn improves students’ clinical performance. The long-term effect is that this will boost students’ motivation and hence skill development as is evident in this study. Other studies have shown the same effects that a supportive CLE is important for student learning,23 valuable learning experiences10 and impacts students’ knowledge, attitudes, skills and interest in their training.24 Feedback in a CLE has also been shown as essential for the student’s motivation, growth, self-esteem, confidence and overall improved clinical practice.25
Exposing optometry students to a variety of patient conditions helps them to acquire valuable insights and practical experience which improves their clinical competence in eye healthcare. The exposure and participation in the clinical environment offer a platform in which students can witness and appreciate what was covered in theory. It is therefore important to expose students to a CLE, and the earlier this happens in their training, the better for mastery of competency and professional development. Similar findings were reported by Sharif & Masoumi,15 among nursing students in Iran. However, unlike Kirkman et al10 participants in this study did not highlight the development of professional identity.
The constraints imposed by restriction on areas of hands-on practice, space, and equipment can significantly affect students’ CL in several ways. The limitation posed by areas of hands-on practice and equipment can restrict learning opportunities and prevent students from fully exploring and engaging in specific diagnostic and treatment procedures commonly used in the field. It is therefore essential to allow students an all-round practice with guidance, and to provide them with the basic equipment for use while in CT. Limited space can result into overcrowding due to the big group of students and this can block students from observing and can also limit their participation. At the end of the day; students may miss out on the intended learning outcomes. This highlights the need to regulate the number of students in consultation rooms or to allocate more space at training sites to improve the learning environment and ensure better clinical training experiences. These findings are consistent with those identified in others studies.12.17,18,19,20
Negative attitudes from the staff can create a hostile learning environment that can lead to hesitation of students to ask questions or seek guidance, hence missed learning opportunities. In order to have a productive CT, the CLE should be inclusive and receptive. It is important for all participants to respect and value each other’s opinions, regardless of their level of experience. In a CLE, staff should provide an environment in which students feel free to share their insights, and they should be heard. That way, the experts can then know how and where to help the student in a way that is not demeaning. Dismissing students’ view without listening may make students to feel incompetent which in turn may lower their self-esteem and demotivate them from active participation in the CLE. Denial, Nehmad, & Appel16 also reported negative attitudes as to affect students in a CLE.
It is important to note that CT at the eye clinic of MNRTH is to a large extent successful in developing the optometry students’ clinical skills as respondents mentioned having gained ability of diagnosing and managing various eye conditions; skills in refraction and binocular vision testing; and attitudes like, effective communication and self-confidence. Students noted that while at other training sites, they undertake hands-on practice for all procedures including those that were restricted at MNRTH.
Strength and Limitations
The strengths of the study lie in the use of an exploratory qualitative design and in-depth interviews which provided very rich descriptions of optometry students’ expressions of the facilitators and barriers of their CL. Key implications for practice arise. First, the facilitators of CL are important factors that contribute to an effective CT hence, there is a need for optometry educators to prioritize them. Second, the barriers are significant challenges to CL and addressing them can enhance the benefits of CT.
This study is limited by the fact that only students’ views were sought without input from their supervisors.
Conclusion
The importance of a supportive and collaborative learning environment together with hands-on practical opportunities seen in this study is consistent with the social constructivist theory of learning. It is therefore best for optometry students to undertake CT in eye clinics so as to develop the expected competences prior to graduation. The role of the optometry educators would be to provide a CLE that maximizes the identified facilitators while minimizing or eliminating the barriers of CL as identified in this or other studies. The kind of opportunities that CT in the eye clinic offers to optometry students are very valuable approaches to CL that may not be covered in textbooks and hence should be utilized. Subsequently, more research is suggested looking at the perceptions of faculty, hospital staff and patients towards optometry students’ CT in the eye clinic. Research on students’ and preceptors’ feedback literacy would yield an understanding of how optometry students receive and act on the feedback while in the CLE.26
Acknowledgements
We thank all optometry students for their time and participation in this study.
The present article was extracted from a master’s thesis that was supported by the Fogarty International Center of the National Institutes of Health under Award Number 1R25TW011213. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
We thank the HePed project under the Norwegian Partnership Programme for Global Academic Cooperation (NORPART) which facilitated the first author’s visit to the University of Bergen in Norway under grant number NORPART-2021/10358, from where he drafted the manuscript.
Authors declare that they have no competing interest.
References
- Steinmetz JD, Bourne RR, Briant PS, et al. Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: the Right to Sight: an analysis for the Global Burden of Disease Study. Lancet Glob Health. 2021 Feb 1;9(2):e144-60. DOI:10.1016/S2214-109X(20)30489-7
- World Health Organization. WHO global report on traditional and complementary medicine 2019. World Health Organization; 2019 May 16.
- Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmol. 2018 Oct 1;125(10):1492-9. DOI:10.1016/j.ophtha.2018.04.013
- Palmer JJ, Chinanayi F, Gilbert A, et al. Mapping human resources for eye health in 21 countries of sub-Saharan Africa: current progress towards VISION 2020. Hum Resour Health. 2014 Dec;12(1):1-6. DOI:10.1186/1478-4491-12-44
- Magyezi J, Arunga S. Eye care where there are no ophthalmologists: the Uganda experience. Community Eye Health. 2020;33(110):48.
- Abu SL. The History and Current Status of Optometric Education in Africa. Hindsight: J Optom Hist. 2020 Sep 28;51(4):84-92. DOI:10.14434/hindsight.v51i4.31557
- Moodley VR. Towards a culture of quality assurance in optometric education in sub-Saharan Africa. Afr Vis Eye Health. 2019 Jan 1;78(1):1-8. DOI:10.4102/aveh.v78i1.462
- Forehand M. Bloom’s Taxonomy: Original and Revised. In: Orey, M, editor. Emerging Perspectives on Learning, Teaching, and Technology (E-Book). 2005 Aug;8:41-4. Available from: https://textbookequity.org/Textbooks/Orey_Emergin_Perspectives_Learning.pdf
- Levy LS, Sexton P, Willeford KS, et al. Clinical instructor characteristics, behaviors and skills in allied health care settings: A literature review. Athl Train Educ J. 2009 Jan 1;4(1):8-13. DOI:10.4085/1947-380X-4.1.8
- Kirkman JM, Bentley SA, Armitage JA, Wood-Bradley RJ, Woods CA. Student perspectives of extended clinical placements in optometry: a qualitative study. BMC Med Educ. 2022 Jan 25;22(1):59. DOI:10.1186/s12909-022-03132-0
- Yardley S, Teunissen PW, Dornan T. Experiential learning: AMEE guide No. 63. Med Teach. 2012 Feb 1;34(2):e102-15. DOI:10.3109/0142159X.2012.650741
- Rajeswaran L. Clinical experiences of nursing students at a selected institute of health sciences in Botswana. Health Sci J. 2016;10(6):1. DOI:10.21767/1791-809X.1000471
- Amineh RJ, Asl HD. Review of constructivism and social constructivism. J Soc Sci Lit Lang. 2015 Apr 30;1(1):9-16.
- Midgley K. Pre-registration student nurses perception of the hospital-learning environment during clinical placements. Nurse Educ Today. 2006 May 1;26(4):338-45. DOI:10.1016/j.nedt.2005.10.015
- Sharif F, Masoumi S. A qualitative study of nursing student experiences of clinical practice. BMC Nurs. 2005 Dec;4:1-7. DOI:10.1186/1472-6955-4-6
- Denial A, Nehmad L, Appel J. Student and Faculty Perceptions of Factors Influencing the Clinical Learning Experience. Optom Ed. 2011 Oct 1;37(1).
- Kagawa MN, Kiguli S, Steinberg WJ, Jama MP. The workplace as a learning environment: Perceptions and experiences of undergraduate medical students at a contemporary medical training university in Uganda. Afr J Health Prof Educ. 2021 Jun 1;13(2):110-7. DOI:10.7196/AJHPE.2021.v13i2.1191
- Msiska G, Smith P, Fawcett T. The “lifeworld” of Malawian undergraduate student nurses: The challenge of learning in resource poor clinical settings. Int J Afr Nurs Sci. 2014;1, 35-42. DOI:10.1016/j.ijans.2014.06.003
- Jamshidi N, Molazem Z, Sharif F, Torabizadeh C, Najafi Kalyani M. The challenges of nursing students in the clinical learning environment: A qualitative study. ScientificWorldJournal. 2016 Jun5;. DOI:10.1155/2016/1846178
- Kizza IB, Tugumisirize J, Tweheyo R, et al. Makerere University College of Health Sciences’ role in addressing challenges in health service provision at Mulago National Referral Hospital. BMC Int Health Hum Rights. 2011 Dec;11:1-0. DOI:10.1186/1472-698X-11-S1-S7
- Kirkman JM, Bentley SA, Armitage JA, Woods CA. Could adoption of the rural pipeline concept redress Australian optometry workforce issues?. Clin Exp Optom. 2019 Nov 1;102(6):566-70. DOI:10.1111/cxo.12873
- Tavakol M, Sandars J. Quantitative and qualitative methods in medical education research: AMEE Guide No 90: Part II. Med Teach. 2014 Oct 1;36(10):838-48. DOI:10.3109/0142159X.2014.915297
- Nordquist J, Hall J, Caverzagie K, et al. The clinical learning environment. Med Teach. 2019 Apr 3;41(4):366-72. DOI:10.1080/0142159X.2019.1566601
- Adam AB, Druye AA, Kumi-Kyereme A, Osman W, Alhassan A. Nursing and midwifery students’ satisfaction with their clinical rotation experience: the role of the clinical learning environment. Nurs Res Pract. 2021 Apr 14;2021. DOI:10.1155/2021/7258485
- Clynes MP, Raftery SE. Feedback: an essential element of student learning in clinical practice. Nurse Educ Pract. 2008 Nov 1;8(6):405-11. DOI:10.1016/j.nepr.2008.02.003
- Carless D, Boud D. The development of student feedback literacy: enabling uptake of feedback. Assess Eval High Educ. 2018 Nov 17;43(8):1315-25. DOI:10.1080/02602938.2018.1463354

