
PEER REVIEWED
An Atypical Case of Uveitis-Glaucoma-Hyphema Syndrome
Claire Henry, OD, Deana Lum, OD, FAAO, and Alvaro J. Castillo, OD, FAAO
Abstract
Uveitis-glaucoma-hyphema (UGH) syndrome is a rare complication of cataract extraction with intraocular lens (IOL) implantation. UGH syndrome is caused by excessive mechanical interaction between the IOL and the iris structure, leading to inflammation, release of iris pigment, hemorrhaging within the anterior chamber, and increased intraocular pressure. If not addressed promptly, this mechanical chafing may lead to glaucoma. Patients may report pain, photophobia, erythropsia, and/or blurry vision. When UGH syndrome is diagnosed promptly, patients often have a good surgical outcome.
Key Words: uveitis-glaucoma-hyphema syndrome, hyphema, intraocular lens, circumferential iris transillumination defects, cataract complications
Background
Uveitis-glaucoma-hyphema (UGH) syndrome was first described in the late 1970s by F. Thomas Ellingson, MD, as a triad of findings caused by mechanical chafing of the anterior iris by the closed haptic loops of an anterior chamber intraocular lens (ACIOL).1 Though incidence has greatly decreased with the improved design of ACIOLs and the shift to posterior chamber intraocular lenses (PCIOLs), UGH syndrome remains a concern after cataract extraction.2,3 With PCIOLs, mechanical interaction between the intraocular lens (IOL) and the posterior iris or ciliary body causes irritation and erosion of the uveal structures, leading to release of pigment. Ultimately, this breakdown of the blood-aqueous barrier leads to the release of proteins and red blood cells (RBCs) into the anterior chamber. Pigment, blood, and inflammatory cells block aqueous outflow via the trabecular meshwork, which leads to increased intraocular pressure (IOP).
In a single-center retrospective study conducted between 2014 and 2018, iris-sutured IOLs accounted for 50% of the UGH syndrome cases.4 In-the-bag IOLs accounted for 20%; scleral-sutured IOLs accounted for 13.3%; sulcus-positioned IOLs accounted for 10%; and IOLs having “in-and-out” position accounted for 6.7% of the UGH syndrome cases.4 Prognosis for UGH syndrome depends on the timing of diagnosis. If IOP remains elevated without treatment for a prolonged period of time, the patient can develop glaucomatous optic neuropathy. Surgical intervention to either replace or reposition the IOL is preferable to medical therapy alone.4 Surgical IOL repositioning or replacement typically has a good visual prognosis and prevents recurrence.2,5
In this report, we describe the case of a 74-year-old Caucasian male who presented urgently for a red eye and was diagnosed with UGH syndrome. We review differential diagnoses for hyphema, the history, pathogenesis, and clinical signs of UGH syndrome, as well as the treatment and management of hyphema and UGH syndrome. The intended audience is third- and fourth-year optometry students, optometry residents, and practicing optometrists.
Case Description
Initial visit (day 1)
A 74-year-old Caucasian male presented for an urgent exam complaining of a red right eye (OD) for 4 days. He reported mild irritation with foreign body sensation, but denied pain, photophobia, mucus, discharge, and any recent trauma or illness. His ocular history was significant for pseudophakia of both eyes (OU) with PCIOL displacement and subsequent repair OD, radial keratotomy (RK) OU, and two retinal detachments OD, one being macula-off. He was also being managed for severe primary open angle glaucoma OD and suspicion of glaucoma in the left eye (OS) and treated with latanoprost every evening OU. His medical history was significant for hypertension and history of mild stroke, for which he had been prescribed lisinopril and low-dose aspirin. He denied diabetes, sickle cell anemia, and any recent symptoms of a transient ischemic attack. He also denied any drug allergies.
His best-corrected visual acuity OD was light perception, reduced from hand motion at 1 foot 2 months prior, and stable OS at 20/25. Given his reduced vision, he was unable to perform confrontation visual field testing OD, but confrontation visual field was full to finger counting OS. Extraocular motility was grossly full OU. The pupil was difficult to visualize OD at this visit, and the left pupil was round and reactive to light. He appeared to have a stable 3+ relative afferent pupillary defect OD, tested by reverse pupil testing.
Anterior segment examination revealed unremarkable eyelids and eyelashes OU, significant hyperemia of the bulbar conjunctiva OD compared with a white and quiet bulbar conjunctiva OS. The cornea had stable cataract extraction and RK scars OU without Seidel sign, and RBCs on the inferior half of the corneal endothelium OD. The anterior chamber was deep and formed OU. There was a 1.5-mm hyphema OD with 3+ cell (mostly RBCs) and 3+ flare (Figure 1), while OS was quiet. There was poor visibility of the iris and lens OD, while OS had mild nasal iris atrophy and a clear, well-positioned PCIOL.
IOP measured 18 mmHg OD and 16 mmHg OS via Goldmann applanation tonometry. B-scan ultrasound revealed a grossly intact posterior segment OD, with no indication of vitreous hemorrhage, ocular malignancy, or retinal detachment. Posterior pole OS was unremarkable and grossly stable to previous findings on undilated fundus exam. The patient was diagnosed with hyphema OD of uncertain etiology, primarily due to the inability to visualize the iris and retina.
At this visit, atropine 1% twice a day OD was initiated to stabilize the blood-aqueous barrier, and the patient was instructed to continue latanoprost every evening OU. As the patient was not symptomatic for uveitis, steroid treatment was deferred. The primary care physician was notified of the recommendation to order a carotid ultrasound. Discontinuation of aspirin was considered, but ultimately not advised unless evidence indicated it was causing a re-bleed. Standard hyphema precautions were advised including avoiding physical exertion, remaining at a minimum 45-degree incline, and using a protective eye shield for sleeping. The patient was instructed to return to the clinic the next day, or to go to the emergency department sooner if he experienced pain.
Follow-up care
Though IOP was normotensive on day 1, it increased to 30 mmHg OD at the first follow-up visit. As a result, latanoprost every evening OU was discontinued due to its pro-inflammatory effect and replaced with timolol 0.5%/dorzolamide 2% twice a day OU. Despite combination therapy, IOP remained in the 28- 32-mmHg range OD while the hyphema was present. IOP remained stable and normotensive OS.
Over the course of the next 2 weeks, the vertical height of the hyphema decreased while on atropine 1% twice a day OD until it was noted as a microhyphema on day 13. The patient’s vision had returned to baseline at hand motion at 1 foot OD, and 20/20 OS.
By day 13, 3+ cell remained (including RBCs) OD but flare decreased to a grade of 1+, allowing visualization of the iris and appreciable midperipheral circumferential transillumination defects (TIDs) at 1:00-4:00, 6:00-7:00, and 9:00-10:00, and no neovascularization of the iris (Figure 2). The PCIOL was present but flush with the iris. Gonioscopy revealed angles open to ciliary body 360 degrees OU with 1+ pigment in the trabecular meshwork OU, flat iris approach OU, and no evidence of neovascularization of the angle, angle recession, or peripheral anterior synechiae OU. The view to the retina OD remained hazy, but no appreciable vitritis or vitreous hemorrhage was noted. All anterior segment findings OS were within normal limits.
 Figure 1. External photo of the right eye at initial presentation: A 1.5-mm hyphema is visible in the inferior anterior chamber, and 3+ flare is obscuring the view of the pupil. The cornea has stable radial keratotomy scars with visible endothelial red blood cell staining on the inferior half. The conjunctiva has significant hyperemia. Eyelids and eyelashes are unremarkable. |
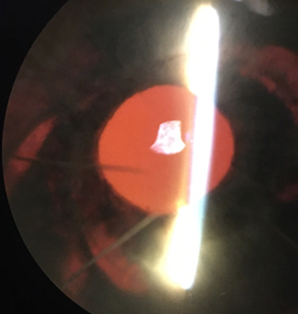 Figure 2. Retro-illumination of the iris of the right eye on day 13: Circumferential transillumination defects 1-4:00, 6-7:00, and 9-10:00 are appreciable. They follow the shape of the IOL optic and haptics. Click to enlarge |
 Figure 3a. Anterior segment OCT of the right eye on day 13: The anterior aspect of the PCIOL is apposed to the posterior iris with significant interaction at the pupil margin. |
 Figure 3b. Anterior segment OCT of the left eye on day 13: No interaction between the PCIOL and the posterior iris. |
The patient was instructed to continue atropine 1% twice a day OD and timolol 0.5%/dorzolamide 2% twice a day OU. He was informed that he no longer needed to maintain a 45-degree incline but was advised to return to the clinic if redness or discomfort returned. The carotid ultrasound was completed and did not reveal any significant or asymmetric stenosis, ruling out ocular ischemic syndrome (OIS) as a diagnosis. Improved visibility of the iris confirmed lack of iris neovascularization, reducing the likelihood of neovascularization due to retinal vascular occlusion. However, because the fundus remained obscured, retinal vascular occlusion could not be definitively eliminated. Retro-illumination of the iris allowed visualization of significant iris TIDs, indicating mechanical interaction between the posterior iris and the PCIOL. Anterior segment optical coherence tomography (OCT) was used to confirm that the PCIOL was displaced anteriorly and interacting excessively with the iris (Figure 3a and 3b), supporting the diagnosis of UGH syndrome. The patient was referred to ophthalmology for evaluation of the IOL.
One month after onset, the patient was evaluated by the general ophthalmologist. At this visit, the hyphema resolved and IOP returned to normotensive with consistent use of timolol 0.5%/dorzolamide 2% twice a day OU. Given that the patient was now asymptomatic and had a long history of complicated and unsuccessful ocular surgeries, he declined surgical intervention. He stated that he was not motivated to preserve vision OD, and he opted to be monitored.
Case history
Given the rarity of in-the-bag PCIOLs causing UGH syndrome, a review of the patient’s ocular history helps to explain why this patient developed such a rare complication. In 2014, he underwent cataract extraction OU. In 2015, he was treated with pneumatic retinopexy for a macula-on retinal detachment OD. Two weeks later, the patient experienced a subluxated PCIOL OD, which the surgeon retrieved and repositioned into the ciliary sulcus. Soon after, the patient experienced a complete macula-off retinal detachment OD, which was subsequently treated with scleral buckle, pneumatic retinopexy, pars plana vitrectomy, endolaser, and silicone oil infusion. When the retina was stable, the retina specialist performed silicone oil removal and fluid-gas exchange.
As a result of this complicated history, the patient developed glaucoma OD, and vision declined to hand motion. The patient’s history of multiple retinal detachments, repeated intraocular surgeries, and IOL dislocation with repositioning into the sulcus likely increased his risk of UGH syndrome compared with non-complicated cataract extraction with PCIOL implantation.
Education Guidelines
Key concepts
- The blood-aqueous barrier: importance and breakdown
- Role of inflammation secondary to mechanical chafing on uveal tissue: pathophysiology and consequences
- IOL malposition: clinical signs, complications, and treatment
Learning objectives
With this case discussion, participants should be able to:
- Learn about the different etiologies and treatment of hyphema
- Identify the signs/symptoms of UGH syndrome
- Learn about the management of UGH syndrome
Discussion questions
- What role do IOLs play in UGH syndrome, and to what extent do ACIOLs and PCIOLs differ in UGH syndrome? (How does the placement of the IOL in the eye increase/decrease the likelihood of UGH syndrome – ACIOL vs. PCIOL in the sulcus vs. in the bag?)
- What is the typical pattern of TIDs seen in UGH syndrome cases? Why does this type of pattern occur?
- What are differential diagnoses for a hyphema?
- Why should we consider what medications a patient is on when diagnosing a hyphema?
- What is the treatment for UGH syndrome? How successful is it?
Teaching instructions
The authors recommend reviewing the discussion and going over the discussion questions to ensure a thorough understanding of the topic. Use of figures/diagrams and photos to review the different locations in which an IOL may be implanted would be helpful in understanding the key concepts and pathophysiology of UGH syndrome. Also helpful would be a review of photos of circumferential TIDs and OCT images that highlight the iris/lens interaction.
Discussion
When UGH syndrome was first described in the 1970s, it was exclusively associated with the ACIOLs of the time. With updated lens design, improved lens fabrication, and evolved surgical techniques, the incidence of UGH syndrome has substantially decreased. With the transition to PCIOLs, many thought UGH syndrome would no longer occur as a post-surgical complication of cataract extraction. However, although it happens infrequently, PCIOLs are capable of causing inflammation and breakdown of the blood-aqueous barrier via mechanical chafing on uveal tissue, as is evidenced by this case. While prompt surgical intervention is recommended in most cases, this patient’s ocular history and limited visual prognosis allowed for less aggressive treatment.
Differential diagnoses for hyphema in adults
Hyphema due to trauma
The most common cause of hyphema is trauma. Hyphema-related orbital trauma is most commonly caused by a high-energy blow to the orbit (61-66%), followed by projectile (30.2-36%) and explosion (2.4-3%).6 There are several possible sources of bleeding in a traumatic hyphema. A direct blow may cause ruptured blood vessels at the anterior ciliary body or iris root, but equatorial expansion and elevated IOP may also cause rupture of ciliary body or iris blood vessels.6
Neovascularization of the iris or angle
Ocular neovascularization is the result of ischemia to ocular structures, most often in the form of retinal hypoxia. Ocular ischemia results in release of angiogenic factors, including vascular endothelial growth factor (VEGF) and others, that stimulate new blood vessel growth.7 Unlike normal ocular blood vessels, these new blood vessels tend to leak fluid and blood and can lead to hyphema when they form in anterior structures. The most common causes of ocular neovascularization are diabetic retinopathy, retinal vein occlusion, and OIS.8
- Diabetic retinopathy: Poor glycemic control in diabetic patients can result in severe retinal ischemia, causing the distressed ocular tissue to release pro-angiogenic factors. This can result in both proliferative diabetic retinopathy and anterior segment neovascularization. Rubeosis iridis may or may not precede angle neovascularization, making gonioscopy a necessity in cases of hyphema or suspected neovascular glaucoma.8
- Retinal vein occlusion: After a retinal vein occlusion, ischemia and capillary nonperfusion lead to an upregulation of inflammatory cytokines and VEGF, resulting in ocular neovascularization.9 An ischemic central retinal vein occlusion can lead to neovascularization of the iris and neovascular glaucoma anywhere between 2 weeks to 2 years after the occlusion, but it most often occurs around 3 months.8
- OIS: ocular ischemic syndrome is hypoperfusion as a result of stenosis or occlusion of the common or internal carotid artery.10 Typical retinal manifestations are dilated retinal veins, mid-peripheral retinal hemorrhages, and neovascularization of the disc. Anterior segment involvement may lead to hypotony due to ciliary body hypoperfusion, but if iris and angle neovascularization occurs, this can also result in elevated IOP or hyphema.
Hyphema due to iris melanoma
Though extremely rare, hyphema can be caused by iris melanoma.11 Though only 2% of iris nevi converted to iris melanoma within 5 years in a Shields study of 1,611 eyes, hyphema was one predictive feature of growth.12
Uveitis-glaucoma-hyphema syndrome
UGH syndrome is a condition that occurs after cataract extraction with IOL implantation. This condition is caused by mechanical chafing of the IOL with the iris, causing hemorrhaging, inflammation, and subsequent IOP increase.5 Though more frequently associated with ACIOLs, UGH syndrome can also occur with poorly positioned PCIOLs.3
In the early days of cataract surgery, the anterior chamber was the preferred location for IOL implantation due to frequent dislocation of PCIOLs. The polymethyl methacrylate (PMMA) lenses of the time were too heavy to be supported posteriorly by the zonules and capsular bag, so surgeons viewed the anterior chamber as a more stable location. However, the anterior chamber placement was not without complications. In 1978, Ellingson first published his observation of the triad of uveitis, hyphema, and glaucoma caused by poorly fabricated ACIOLs.1 Initially coined Ellingson syndrome, uveitis-glaucoma-hyphema syndrome was attributed to poorly finished lenses, primarily warped footplates and poor edge finish.13 Lenses of similar design, but better manufacture quality, are still used today for ACIOLs with much lower frequency of complications. Other improvements made to ACIOLs over the years include discontinuation of nylon and metal as haptic materials and a switch to flexible semi-rigid loops. Also, lens insertion glides and viscoelastic have allowed for smoother lens insertion.13,14
A significant decrease in the incidence of UGH syndrome is attributed to the rise of PCIOLs. In-the-bag placement reduces the risk of direct contact between the PCIOL optics or haptics with uveal tissue. Altogether, these improvements in lens design and surgical technique led to a decrease in annual incidence of UGH syndrome from 2.2-3.0% per year to 0.4-1.2%.3,13 Case reports of UGH syndrome associated with PCIOLs rarely, if ever, corresponded to uncomplicated cataract surgeries. PCIOL complications that have led to UGH syndrome include haptic migration into the anterior chamber,15 bag tearing with haptic migration into the sulcus,16,17 pseudophacodonesis secondary to pseudoexfoliation syndrome,18 and focal capsular fibrosis leading to mechanical chafing on the posterior iris.19 In this patient’s case, repositioning of the PCIOL into the sulcus likely led to excessive interaction between the iris and PCIOL.
In this case and many others, TIDs can provide helpful clues in diagnosis of UGH syndrome. TIDs after cataract extraction are common, but pattern and location can differ based on cause. In contrast with pupillary margin TIDs caused by surgical instruments during cataract extraction, circumferential shape and mid-peripheral location of TIDs indicate chafing of the IOL optics and haptic on the posterior iris. This unique pattern is indicative of excessive PCIOL interaction with the iris and is frequently seen in UGH syndrome.5
Several treatment options are available for patients with traumatic hyphema. Typically, patients are given an eye shield and told to sleep at an incline to keep the blood in the inferior anterior chamber. Antifibrinolytic agents have been demonstrated to reduce the risk of re-bleeding in traumatic hyphema, but may prolong the duration of hyphema.20,21 Additionally, many patients reported side effects of nausea and vomiting, and the systemic formulation is contraindicated in patients with renal disease, as in the case with this patient. Also, topical formulations of antifibrinolytic agents must be requested from a compounding pharmacy and are difficult to access. Topical corticosteroids and cycloplegics decrease the risk of developing posterior synechiae, stabilize the blood-aqueous barrier, and reduce symptoms of uveitis.22 Furthermore, cycloplegics may increase uveoscleral outflow, and corticosteroids reduce the risk of re-bleeding.6,20 Given the poor visual potential and the initial unknown etiology due to poor visualization of the iris and posterior segment, a conservative management approach was taken with this patient. As the patient was not symptomatic for uveitis, he was treated only with atropine 1% twice a day OD until the hyphema resolved. The prostaglandin analog glaucoma therapy was also replaced with a combination beta blocker/carbonic anhydrase inhibitor (CAI) due to inadequate IOP control on prostaglandin alone throughout the course of the hyphema.
Currently, there is no consensus regarding what effect aspirin has on the risk of re-bleeding in traumatic hyphema. Some clinical trials have found that use of aspirin made no difference in incidence of re-bleeding.23 Conversely, other studies found that use of aspirin increased the risk of re-bleed after traumatic hyphema. One small study found that 7 of 12 patients who used aspirin after traumatic hyphema experienced a re-bleed, compared with 1 of 13 patients who did not use aspirin.24 As a result, the decision to discontinue aspirin or other anticoagulant therapy in the case of hyphema should be made on a case-by-case basis. If a patient uses aspirin purely for its analgesic properties, it would be reasonable to recommend a different analgesic. However, if the patient has been prescribed aspirin or other anticoagulants to reduce the risk of stroke, as was the case with this patient, optometrists should be extremely cautious before recommending discontinuation of anticoagulants. Low-dose aspirin has been proven to reduce risk of ischemic stroke,25 and discontinuation of aspirin has been shown to lead to increased risk of recurrent stroke from 29% to 51% in moderate-to-high-risk patients.26 Therefore, discontinuation of aspirin was not recommended in this case, and the patient did not experience a re-bleed. Extreme caution is advised before discontinuing aspirin in cases of hyphema when the patient is at risk of stroke.
Another consideration in this case was the use of prostaglandins for IOP control in the context of active uveitis. The role of prostaglandins as an inflammatory mediator is well-established, but the suggested association between prostaglandins and uveitis remains controversial. In the late 1990s, Warwar and colleagues published a series of case reports indicating the incidence of anterior uveitis was 6% and the incidence of cystoid macular edema was 2% in patients using latanoprost, suggesting that topical prostaglandins led to intraocular inflammation.27 Smith et al. found that initiation of latanoprost induced uveitis in 1% of patients without history of uveitis, caused recurrences in 23% of patients with history of uveitis, but did not cause worsening inflammation in patients with active uveitis.28 In a case series in which four patients experienced resolution of uveitis after discontinuation of latanoprost, all four experienced recurrences when latanoprost was re-challenged.29 However, a more recent study found no difference in anterior uveitis or cystoid macular edema in patients using prostaglandin analogs vs. other IOP-lowering therapies.30 Overall, these findings indicate that a very small percentage of people are susceptible to prostaglandin-induced uveitis, and prostaglandins may increase risk of recurrences in patients with history of uveitis.
Because of their slow mechanism of action, prostaglandin analogs are not recommended for treating acute elevated IOP in patients with hyphema or UGH syndrome. However, there is no current recommendation regarding use of prostaglandin analogs for pre-existing glaucoma during the treatment course of hyphema. While it is unknown if the pro-inflammatory properties of prostaglandins alter or prolong the healing course of UGH syndrome, it is unlikely to effectively control further elevated IOP due to hyphema. Therefore, beta blockers and CAIs are recommended during hyphema because they are fast-acting and target aqueous production.6
In this case, the patient’s IOP was no longer well-controlled with a prostaglandin analog after the development of hyphema, and he was switched to beta blocker/CAI combination therapy to better control IOP.
With respect to other glaucoma medications, oral CAIs, especially acetazolamide, are contraindicated in patients with sickle cell disease or trait as they can increase sickling of erythrocytes. If an oral CAI must be used, methazolamide would be a better choice.
For hyphema caused by UGH syndrome, surgical repositioning of the IOL is the recommended treatment to prevent re-bleeding and prolonged IOP elevation. In a retrospective study looking at the outcome of 71 cases of UGH syndrome associated with PCIOLs, 60 patients underwent surgery. Of these, 46 never had a recurrence of UGH syndrome, seven had only a single recurrence that subsequently resolved, and seven had no recurrences after a second repositioning surgery. In the 11 cases that were not treated surgically, five had a recurrence of UGH syndrome within the first year of follow-up. Of the 60 surgical interventions, 14 had IOL exchange and 46 underwent repositioning of the existing IOL with 71-74% success in preventing recurrences after the initial surgery. Even in cases where surgical intervention did not prevent recurrence, there was significant improvement in best-corrected visual acuity and IOP in the surgical group compared with the non-surgical group.5
These findings indicate that the patient in this case report is at high risk of a re-bleed due to declining surgical intervention. However, this patient has profoundly reduced baseline vision and was generally asymptomatic during his bout of UGH syndrome, so there are limited benefits to surgical intervention. The goal of this patient’s ophthalmic care has shifted to comfort rather than vision preservation. Therefore, surgical intervention can continue to be deferred unless ocular comfort is compromised.
Conclusion
UGH syndrome is a rare but vision-threatening complication of cataract surgery. Though uncommon, especially in the case of PCIOLs, it should remain a differential diagnosis in non-traumatic presentations of hyphema. In this case, the patient’s complicated history of retinal detachment and retinal surgeries led to malpositioning of the IOL, resulting in mechanical chafing and subsequent uveitis and hyphema. Though surgical intervention is recommended in most cases to improve vision and prevent recurrence, this patient declined surgery due to poor visual potential and resolution on conservative topical therapy. Nevertheless, surgical repositioning or replacement of the IOL will result in the best outcome for patients with UGH syndrome and reduce the risk of glaucomatous optic neuropathy. The current recommendation for management of hyphema is bed rest and elevation, topical corticosteroids and/or cycloplegics, avoidance of unnecessary anticoagulants, and control of IOP. These patients must be monitored closely until resolution of the hyphema, and the optometrist must investigate all possible etiologies of hyphema to address the cause and prevent recurrence.
References
- Ellingson FT. The uveitis-glaucoma-hyphema syndrome associated with the Mark VIII anterior chamber lens implant. J Am Intraocul Implant Soc. 1978 Apr;4(2):50-3. doi: 10.1016/s0146-2776(78)80054-8.
- Elhusseiny AM, Lee RK, Smiddy WE. Surgical management of uveitis-glaucoma-hyphema syndrome. Int J Ophthalmol. 2020 Jun 18;13(6):935-940. doi: 10.18240/ijo.2020.06.12.
- Zemba M, Camburu G. Uveitis-glaucoma-hyphaema syndrome. general review. Rom J Ophthalmol. 2017 Jan-Mar;61(1):11-17. doi: 10.22336/rjo.2017.3.
- Duchêne M, Iscar C, Muraine M, Gueudry J. Caractéristiques et prise en charge du syndrome uvéite-glaucome-hyphéma [Characteristics and management of uveitis-glaucoma-hyphema syndrome]. J Fr Ophtalmol. 2020 Mar;43(3):205-210. French. doi: 10.1016/j.jfo.2019.07.030.
- Armonaite L, Behndig A. Seventy-one cases of uveitis-glaucoma-hyphaema syndrome. Acta Ophthalmol. 2021 Feb;99(1):69-74. doi: 10.1111/aos.14477.
- Bansal S, Gunasekeran DV, Ang B, et al. Controversies in the pathophysiology and management of hyphema. Surv Ophthalmol. 2016 May-Jun;61(3):297-308. doi: 10.1016/j.survophthal.2015.11.005.
- Shazly TA, Latina MA. Neovascular glaucoma: etiology, diagnosis and prognosis. Semin Ophthalmol. 2009 Mar-Apr;24(2):113-21. doi: 10.1080/08820530902800801.
- Rodrigues GB, Abe RY, Zangalli C, et al. Neovascular glaucoma: a review. Int J Retina Vitreous. 2016 Nov 14;2:26. doi: 10.1186/s40942-016-0051-x.
- Ip M, Hendrick A. Retinal vein occlusion review. Asia Pac J Ophthalmol (Phila). 2018 Jan-Feb;7(1):40-45. doi: 10.22608/APO.2017442.
- Terelak-Borys B, Skonieczna K, Grabska-Liberek I. Ocular ischemic syndrome – a systematic review. Med Sci Monit. 2012 Aug;18(8):RA138-144. doi: 10.12659/msm.883260.
- Kaliki S, Shields CL. Uveal melanoma: relatively rare but deadly cancer. Eye (Lond). 2017 Feb;31(2):241-257. doi: 10.1038/eye.2016.275.
- Shields CL, Kaliki S, Hutchinson A, et al. Iris nevus growth into melanoma: analysis of 1611 consecutive eyes: the ABCDEF guide. Ophthalmology. 2013 Apr;120(4):766-72. doi: 10.1016/j.ophtha.2012.09.042.
- Apple DJ, Mamalis N, Loftfield K, Googe JM, Novak LC, Kavka-Van Norman D, Brady SE, Olson RJ. Complications of intraocular lenses. A historical and histopathological review. Surv Ophthalmol. 1984 Jul-Aug;29(1):1-54. doi: 10.1016/0039-6257(84)90113-9.
- Mamalis N. Explantation of intraocular lenses. Curr Opin Ophthalmol. 2000 Aug;11(4):289-95. doi: 10.1097/00055735-200008000-00011.
- Lin CJ, Tan CY, Lin SY, Jou JR. Uveitis-glaucoma-hyphema syndrome caused by posterior chamber intraocular lens–a rare complication in pediatric cataract surgery. Ann Ophthalmol (Skokie). 2008 Fall-Winter;40(3-4):183-4.
- Aonuma H, Matsushita H, Nakajima K, Watase M, Tsushima K, Watanabe I. Uveitis-glaucoma-hyphema syndrome after posterior chamber intraocular lens implantation. Jpn J Ophthalmol. 1997 Mar-Apr;41(2):98-100. doi: 10.1016/s0021-5155(97)00005-1.
- Badakere SV, Senthil S, Turaga K, Garg P. Uveitis-glaucoma-hyphaema syndrome with in-the-bag placement of intraocular lens. BMJ Case Rep. 2016 Jan 19;2016:bcr2015213745. doi: 10.1136/bcr-2015-213745.
- Sousa DC, Leal I, Faria MY, Pinto LA. A rare manifestation of uveitis-glaucoma-hyphema syndrome. J Curr Glaucoma Pract. 2016 May-Aug;10(2):76-8. doi: 10.5005/jp-journals-10008-1205.
- Zhang L, Hood CT, Vrabec JP, Cullen AL, Parrish EA, Moroi SE. Mechanisms for in-the-bag uveitis-glaucoma-hyphema syndrome. J Cataract Refract Surg. 2014 Mar;40(3):490-2. doi: 10.1016/j.jcrs.2013.12.002.
- Gharaibeh A, Savage HI, Scherer RW, Goldberg MF, Lindsley K. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD005431. Update in: Cochrane Database Syst Rev. 2013;12:CD005431. doi: 10.1002/14651858.CD005431.pub2.
- Karkhaneh R, Naeeni M, Chams H, Abdollahi M, Mansouri MR. Topical aminocaproic acid to prevent rebleeding in cases of traumatic hyphema. Eur J Ophthalmol. 2003 Jan-Feb;13(1):57-61. doi: 10.1177/112067210301300108.
- Walton W, Von Hagen S, Grigorian R, Zarbin M. Management of traumatic hyphema. Surv Ophthalmol. 2002 Jul-Aug;47(4):297-334. doi: 10.1016/s0039-6257(02)00317-x.
- Marcus M, Biedner B, Lifshitz T, Yassur Y. Aspirin and secondary bleeding after traumatic hyphema. Ann Ophthalmol. 1988 Apr;20(4):157-8.
- Ganley JP, Geiger JM, Clement JR, Rigby PG, Levy GJ. Aspirin and recurrent hyphema after blunt ocular trauma. Am J Ophthalmol. 1983 Dec;96(6):797-801. doi: 10.1016/s0002-9394(14)71926-9.
- Oza R, Rundell K, Garcellano M. Recurrent ischemic stroke: strategies for prevention. Am Fam Physician. 2017 Oct 1;96(7):436-440.
- Negm M, Abd El-Razek R. Role of aspirin discontinuation in recurrence of ischemic cerebrovascular stroke. Egypt J Neurol Psychiatry Neurosurg. 2019;(55)14. Available from: https://doi.org/10.1186/s41983-019-0066-y.
- Warwar RE, Bullock JD, Ballal D. Cystoid macular edema and anterior uveitis associated with latanoprost use. Experience and incidence in a retrospective review of 94 patients. Ophthalmology. 1998 Feb;105(2):263-8. doi: 10.1016/s0161-6420(98)92977-3.
- Smith SL, Pruitt CA, Sine CS, Hudgins AC, Stewart WC. Latanoprost 0.005% and anterior segment uveitis. Acta Ophthalmol Scand. 1999 Dec;77(6):668-72. doi: 10.1034/j.1600-0420.1999.770612.x.
- Fechtner RD, Khouri AS, Zimmerman TJ, Bullock J, Feldman R, Kulkarni P, Michael AJ, Realini T, Warwar R. Anterior uveitis associated with latanoprost. Am J Ophthalmol. 1998 Jul;126(1):37-41. doi: 10.1016/s0002-9394(98)00071-3.
- Chang JH, McCluskey P, Missotten T, Ferrante P, Jalaludin B, Lightman S. Use of ocular hypotensive prostaglandin analogues in patients with uveitis: does their use increase anterior uveitis and cystoid macular oedema? Br J Ophthalmol. 2008 Jul;92(7):916-21. doi: 10.1136/bjo.2007.131037.

