
PEER REVIEWED
Valuable yet Judgmental: Optometry Students’ Perceptions of their Grand Rounds
Elzana Kempen, BOptom, PGDip Sports Vision, MHPE, PhD HPE, Mpho P Jama, BCur, MHiger Ed, PhD Higher Ed, Mathys J Labuschagne, MB ChB, MMed(Ophth); PhD(HPE)
Abstract
Background: The debate over the effectiveness of grand rounds prompted an optometry department to explore their students’ perceptions of this pedagogical tool. Methods: Data were collected with an open-ended questionnaire after 6 months of weekly grand rounds (n=68), with senior students (n=17) also providing data following their presentations. Results: Thematic analysis revealed that students perceived grand rounds for presenting clinical cases and learning from peers. While students appreciated the valuable insights, they felt a sense of criticism and judgment, highlighting the lack of a supportive learning environment. Conclusion: These findings emphasize how educators’ feedback plays a key role in shaping a student’s learning experience.
Key Words: grand rounds, optometry education, clinical learning environment, qualitative research
Background
In the realm of health education, the value and efficacy of grand rounds as a teaching-learning method has been a subject of debate.1 In contrast to several other health disciplines, optometry grand rounds have yet to be thoroughly studied.2,3,4 Consequently, there exists a gap in understanding whether this traditional educational pedagogy is still effective and aligns with the educational needs in optometry education. By identifying both the strengths and areas for enhancement of the method, a program can better align this teaching approach with evidence-based practices and recommendations, thereby ensuring its effectiveness in application.
Grand rounds have a long history in medical education and are a prevalent and effective teaching-learning method in health sciences education.1,2 Traditional grand rounds, as described in the literature, originated from bedside teaching, and due to popularity, students’ attendance increased, and the teaching moved from the bedside to a lecture hall.1 This teaching-learning method captures students’ interest by applying patient-centered, evidence-based practice compared to classic lecture presentations.5 Case discussions during grand rounds provide an educational platform for improving clinical knowledge development while increasing the student’s diagnostic reasoning abilities.5,6 Fasbinder et al.4 suggest that grand rounds should be used to create an educational environment where principles such as critical clinical thinking and integration of knowledge can be implemented. Sandal et al.7 affirm that grand rounds serve as a conduit for disseminating knowledge, changing health professionals’ behavior and improving patient outcomes.
Herbert and Wright2 report that grand rounds have always been a respected teaching-learning method, but it has lost its attraction due to audience boredom and lack of case appropriateness. It is also important to modernize this pedagogical approach to serve the current generation of students.8 While current literature offers guidance on the implementation of grand rounds,7,8 there exists a significant gap in our understanding, particularly concerning students’ perspectives about the learning environment through this pedagogical approach in optometry education. This article addresses that gap by exploring optometry students’ perceptions of grand rounds as a teaching and learning tool.
Study Design/Methods
Ethical clearance to conduct the study was obtained from the Health Sciences Research Ethics Committee (HSREC) (HSREC no 128/2016). The University of the Free State, South Africa, offers a four-year undergraduate Baccalaureus Optometry degree that prepares students to practice optometry in accordance with category three (ocular diagnostic services) as outlined in the World Council of Optometry (WCO) model framework.9 The department has embraced a didactic grand rounds teaching and learning strategy, which is widely recognized as the prevailing format for grand rounds in health sciences education.1 Attendance at Friday morning sessions was mandatory as it contributed to clinical attendance. This mandate applied to students in their second to fourth year and the department’s eight faculty members. Therefore, the sample population for this study included all students enrolled in their second, third and fourth year (Table 1, below) in the undergraduate optometry program during 2017 (n=68).
At the beginning of the academic year, a predetermined schedule assigned three students to present in each session, ensuring that each student presents only once. The sessions ran from March to September of 2017. During these sessions, third-year students presented self-identified general optometry cases. These included cases that only required refractive management interventions. This approach was employed to familiarize the students with the grand round format and to enhance their comfort level in speaking before a large audience. The fourth-year (final-year) students showcased specialized optometry cases, including those related to contact lenses, low vision, pathology, binocular vision, or pediatric vision. According to the schedule, all fourth-year students presented during the first half of the year, followed by the third-years, completing the schedule in September. Students were provided with a rubric and a presentation template at the beginning of the year. Students also participated in an introductory session where all expectations and requirements were thoroughly explained. To adhere to the guidelines mentioned by Sandal et al.,7 the presenters were assessed according to the given rubric. Academic staff members and fellow students did the assessment. The assessment mark counted towards the overall formative assessment mark for the relevant module.
This study formed part of a larger project aimed at determining undergraduate optometry students’ experiences and perceptions of teaching-learning methods based on the experiential learning theory.10 All members of the sample population received information regarding the research project at the beginning of the year and were invited to participate in the study. The informed consent affirmed participants’ voluntary agreement to partake in the research, with the option to withdraw at any point during the questionnaire completion. No compensation was offered for participation. Participants were also assured of confidential data handling and guaranteed anonymity as no personal information such as names or student numbers were requested, and unique code numbers were assigned to each questionnaire. This study used a qualitative case study approach with an open-ended questionnaire. By employing the questionnaire, students were prompted to partake in reflective practice and to facilitate this, the questionnaire was customized to align with Gibbs’s cycle of reflection.11 Appendix A contains the open-ended questions that were asked and provided in hard copy after the completion of the learning experience. The questionnaire required approximately 20-30 minutes to complete.
During the first half of the year, the questionnaire was exclusively extended to fourth-year students (n=17) following their individual presentation experience. This was done to capture the presenter’s viewpoint. As the third-year students presented for the purpose of familiarization, they were not included in the invitation to participate in the questionnaire as presenters. On the last session in September (2017), the second-, third- and fourth-year students (67) who attended the specific session were invited to complete the questionnaire. They were asked to reflect on their experience as attendees throughout the year. As a result, the fourth-year students completed the same questionnaire twice to incorporate their perspectives as both presenters and attendees.
Thematic analysis was conducted to identify key themes.12 During the analysis, the first author was guided by three key phases.13 In the descriptive phase, the first author gained intimate knowledge of the data and obtained a sense of the whole by typing the questionnaires verbatim.14 The analysis phase followed, identifying and refining themes using response codes.15 The number of themes was reduced by creating a table with initial categories and patterns, and connections within and between themes were made to create primary and sub-categories.16 An independent co-worker checked the groupings and categories to ensure authenticity. In the final stage, interpretation or compilation, the themes and connections were used to explain the findings and to attach meaning and significance to the analysis.16 Themes were further refined to include supporting quotations made by the participants. To support trustworthiness, the researchers in this study kept an audit trail of the procedures and processes used.17
Results
The response rate for completing the questionnaire at the end of the year from an attendee’s perspective was 98.5% (Table 1).
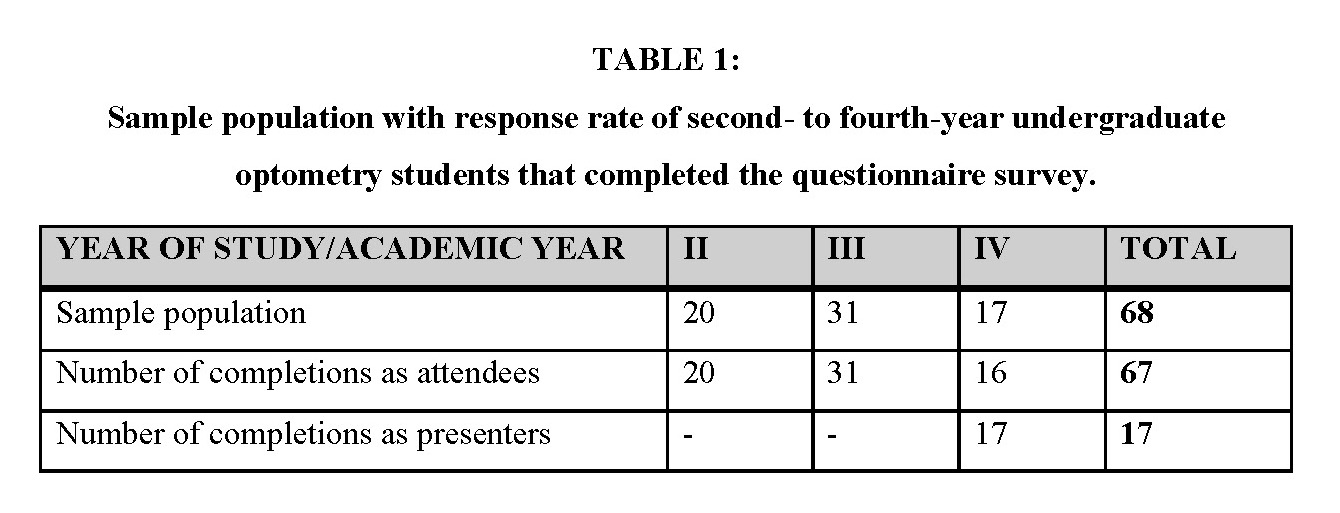
Table 1. Click to enlarge
Females dominated the attendee population, and only 29.4% were male. The median age of the students was 21.0 years, with a minimum age of 19 and a maximum age of 33. All 17 students completed the questionnaire as presenters. Within this group, only four were male, and a majority of eleven students were 21 years old, while the remainder were 22. In the questionnaire, participants were asked about their experiences and perceptions of grand rounds as a teaching and learning method, along with themes of the objective, strengths and weaknesses, personal feelings and recommendations. After the interrogation of the data, subthemes emerged. The results below portray the themes (Figure 1) and the responses of the presenters and the attendees.
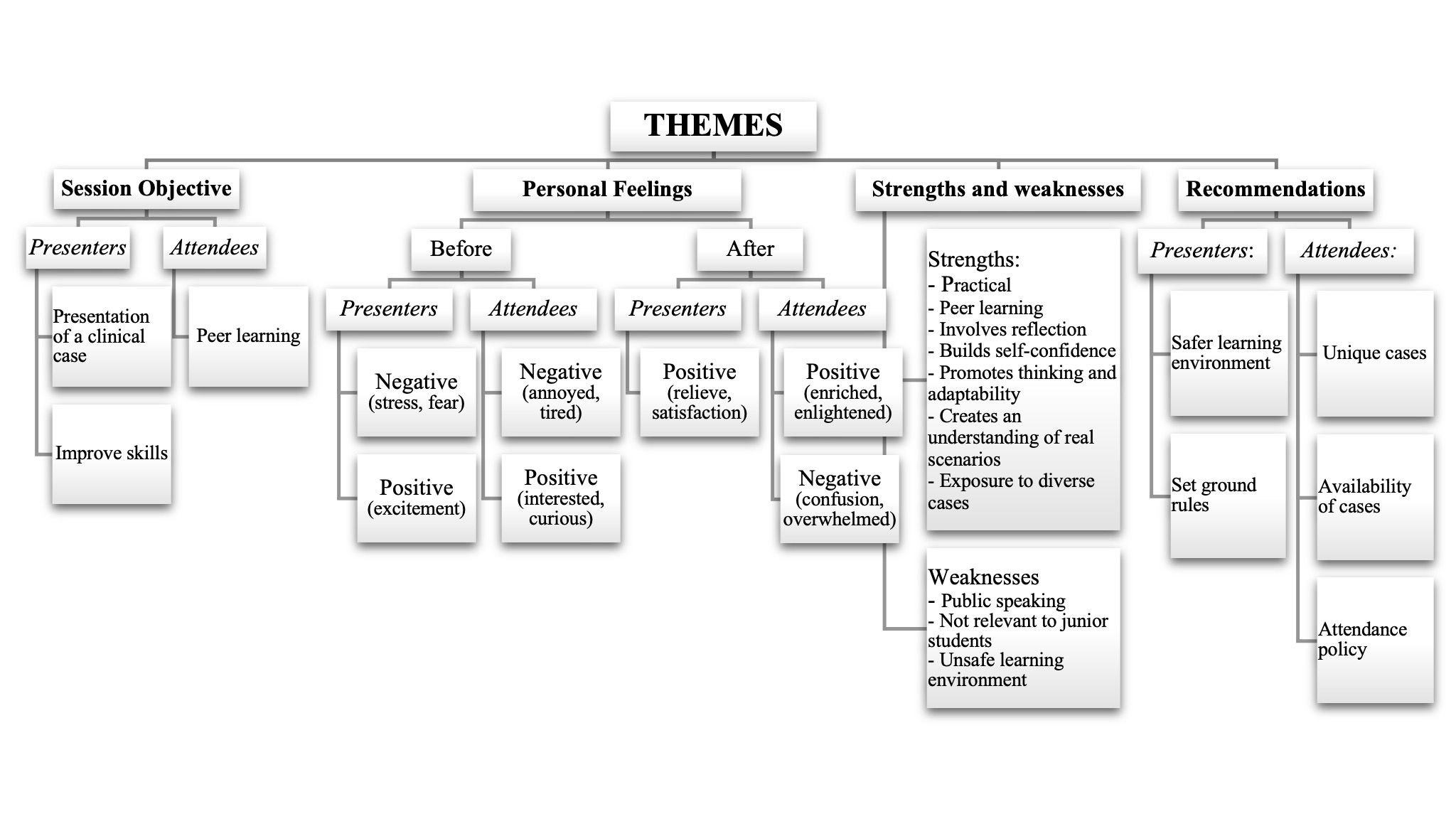
Figure 1. Click to enlarge
Theme 1: Objective. What were the objectives of the session in which the teaching and learning method was used?
Presenters: In the questionnaire, participants were asked about the objective of grand rounds, and from the presenter’s view, many reported that it was the presentation of a clinical case to peers. They elaborated that to present the clinical case, they had to reflect on their experience in the clinic, analyze the tests performed on the patient and the results and research other cases similar to the relevant clinical case. The advice provided by peers and faculty members on a specific case was also included. One participant described the objectives as follows:
Presenting a case seen in the clinic, where you then present the clinical finding and do research on a relevant topic. Students and lecturers then advise you on how to improve skills. [P3]
Attendees: Most attendees expressed that the primary objective of attending grand rounds was to learn from the clinical cases and experiences shared and discussed by fellow students. Within this peer learning experience, they could learn from other’s mistakes and improve their clinical skills as they observed different clinical experiences of their peers. The more senior students specifically mentioned that by attending grand rounds, they could improve their knowledge of pathology because rare cases often were presented as one participant labelled the objective as
to see different cases of patients, to improve our clinical techniques and to know how to approach different types of patients. [P22]
Theme 2: Personal feelings. How did you feel before, during and after this teaching and learning method / experience?
Presenters: Most of the participants who presented felt negative before the learning experience. Feelings of stress, nervousness and fear were expressed. These feelings mainly surfaced because this experience involved public speaking. Some participants had positive feelings before the presentation, such as excitement and enjoyment, like this participant who stated,
‘(I was) excited to talk about my interesting case I had in the clinic that had myself and the supervisors thinking outside the box’ [P9].
The participants’ negative feelings transformed into positive ones, with nearly all respondents indicating a positive shift in their feelings after presenting their cases. They were mostly relieved after the grand rounds, experiencing it as positive. Other feelings mentioned included enlightenment, happiness and satisfaction. The positive feelings stemmed primarily from participants’ perceptions that they had worked hard as this participant mentioned
‘I feel I’ve done a good job! I could answer my questions carefully because I was well prepared’ [P6].
The positive emotions stemmed from their perception of the experience as informative. Additionally, they noted an enhanced integration between foundational knowledge and clinical application and acknowledged the importance as expressed by this participant:
‘Just realised again how important it is to apply what we learn theoretically practically and not to separate theory and practical’ [P12].
Attendees: The attendees’ feelings before the experience were evenly divided between positive and negative. Participants voiced negative feelings mainly because the grand rounds was early on a Friday morning, so they felt annoyed, tired and not in the mood. A second-year student mentioned feelings of irritation, intimidation and nervousness and reported that
‘as second year I know little and I get on my nerves if the third and fourth years speak with a lot of knowledge (it feels unreal that I almost have to treat patients), and I felt that I had little knowledge and was unsure why I had to attend’ [P10]
Positive feelings, such as excitement, interest, relaxation, calmness, curiosity and eagerness, were reported during the learning experience. The participants contended to have felt interested and informed during the grand rounds. In the words of participant 42:
‘I was excited to see many new things and learn about weird and wonderful cases’.
The interest in and sense of expanding knowledge were sparked, particularly by the unique and fascinating cases, especially those involving research.
Most of the participants reported that they felt positive after attending grand rounds. Other feelings related to being informed were expressed.
‘I am informed about other diseases that I did not know about and also have extra knowledge from cases and mistakes’[P1].
Other feelings mentioned were feelings of becoming educated, enlightened, enriched, fulfilled and satisfied and enlightened as this participant expressed the feeling after.
‘Enlightened and feeling like I know a bit more or want to see or try something different in clinic’ [40].
These feelings they reported were mainly due to the participants experiencing the grand rounds as a meaningful interactive teaching-learning method. A few participants responded with negative feelings after the grand rounds. Feelings reported were confusion, being overwhelmed, tiredness, fear and being upset. These negative feelings mainly originated from the comments and questions after the grand rounds as this participant voiced their feelings as
‘scared and upset more often than not because the lecturers’ comments made me question my career choice’ [P36]
Theme 3: Strengths and weaknesses. Based on your experience, what would you say are the strengths and weaknesses of this teaching and learning method?
Presenters and attendees: The participants identified several strengths of this teaching and learning method. The first strength is that they identified it as a practical teaching and learning method that creates interaction and insightful discussions. They also felt that the teaching and learning method created an opportunity for peer learning and to derive valuable lessons from both personal and other’s mistakes. As one participant mentioned,
you learn the best through mistakes, so you can relate to the students presenting and learn from their mistakes [P13].
They also benefitted and felt that the reflection on the case and the engagement in research provided valuable insights and enhanced clinical techniques. Knowing that they will need to present ensured thoroughness in the clinic to avoid oversights during the presentation, and the presentation itself built self-confidence and promoted thinking and adaptability, as noted by this participant,
it forces us to think fast and step out of our comfort zones. [P13].
The cases presented also created an understanding of real-world patient scenarios, and the sessions provided exposure to a diverse range of cases and that
would have taken me years to obtain experience in all these cases myself. Now I saw all of them. [P22]
The participants mentioned a few weaknesses of this experience. The experience involved the presentation to a large audience, and some participants found it stressful as this participant stated,
‘The fact that it is done in front of many people can often make non-public speakers feel uncomfortable and can, at times, be very unpleasant’ [P13]
Another area for improvement, according to participants, is that they felt that it might not be relevant to junior students in the department, as students in the early years might not have the foundational knowledge. This was not only mentioned by the second and third years but also by the fourth years, as they had experienced it in their early study years. One participant mentioned,
‘The second years may feel lost in the beginning because there are terms used that had not been taught to us yet, and then we don’t necessarily concentrate, and the learning experience was wasted.’ [P9]
The main weakness of this teaching-learning method, as identified by the participants, is that they believed it needed to be applied in a safe learning environment. They felt that the experience was critical and judgemental, like being executed or being in a court trial. As stated by these participants,
‘Not feel safe in environment – you feel on edge if presenting if you’re going on an execution.’ [P45]
‘students are just students and grand rounds is a learning experience and not a court trial’ [P11].
Based on the data, it appears that the presence of faculty members during the sessions contributed to this weakness as one participant mentioned,
‘It often happens that (faculty members) strongly criticise the students, so I was incredibly scared what they would say after the time’ [P51]
‘they aren’t always aware of the difficulty of the patient, therefore being too judgemental and strict.’ [P54]
This weakness was reported throughout the data. Participants felt exposed during this experience and perceived it as intimidating. They provided the following reasons:
- The feedback was sometimes destructive and exposed the student:
‘The feedback is a bit harsh at times and critical and not constructive, which not only puts a damper on the proceedings but fuels the negative association with this experience.’ [P2]
- Challenging questions are asked and the way the questions were asked was negative:
‘The questions asked afterwards sometimes are rude and degrading.’[P28]
- Mistakes were only pointed out and not explained
Theme 4: Recommendations. What can you recommend to enhance the teaching and learning method in the future?
Presenters: From the presenter’s view, a category to create a safer learning environment emerged. Firstly, the participants recommended that the supervisor involved in the case should review the case before the presentation as this participant mentioned that
‘Supervisors guide students in clinic and help with differential diagnosis and final diagnosis. Thus, the final diagnosis isn’t always that of the student, but a supervisor. It will help if supervisors give feedback on cases before presented’ [P3]
Secondly, they recommend that the criticism provided should be constructive and not to destruct the students’ self-esteem. Several participants also recommended that the feedback be given in private to each presenter and not in the presence of the whole audience. The participants mentioned that, in their opinion, the feedback should be
‘more educational and supportive rather than the bad criticizing environment it is in at this stage’[P59].
The presenters also advised establishing ground rules regarding attendee punctuality. One participant emphasized,
‘I would only suggest that all persons attending grand rounds should be on time, including lecturers as it is very rude to be late and enter the room in the middle of a students’ presentation [P54].
They also felt that only a certain number of questions should be allowed to be asked to each presenter. They recommended setting clear expectations for each year-group on the presentations to feel better prepared.
Attendees: The participants also made recommendations about the type of case presented. The participants stated that there should be a standard set for cases to prevent non-interesting cases from being presented. One participant mentioned that only interesting cases from the specialized clinics should be presented. Moreover, it should be ensured that there is no repetition of cases. A fourth-year student also mentioned that the research should be on new information and not a repetition of lectures. They also recommended that lecturers present unusual cases they had seen. The participants also suggested that the case reports should be accessible post-presentation, in line with the recommendation put forth by a specific participant:
‘Maybe students can also make a grand rounds journal to remember all the cases and conditions and management’ [P33].
A final recommendation made by the participants involved the attendance of the grand rounds. However, there was no unanimous agreement on which year groups should attend in grand rounds. Some participants asserted that second-year students should exclusively attend later in the year. As this second year stated,
‘I would let the second years sit in for the second semester when they have been taught the majority of the terms and tests being talked about so that they know what’s going on’ [P9].
Some third- and fourth-year students proposed that even first-year students should be present according to the view of this participant:
…first years should also attend grand rounds. This will enhance their knowledge from an earlier stage. [67].
Due to compulsory attendance, certain participants suggested a modification in the schedule by shifting the time and holding the sessions every other Friday.
Discussion
In the evolving landscape of health sciences education, grand rounds has held its place as a venerable teaching-learning method. However, despite its historical reverence, this pedagogical approach has encountered challenges that demand attention. The decline in appeal has raised questions about its overall efficacy. This study explored new and uncharted territory by acknowledging the necessity to update educational approaches in line with the preferences of the current generation of students. This study successfully addressed this gap, and its importance lies in the revelation of student viewpoints. Exploring student perspectives is vital to ensuring the effectiveness, enduring value and relevance of grand rounds in the optometry programme at the University of the Free State, South Africa.
The exit level outcome of presenting a clinical case requires students to demonstrate the integration of required theoretical knowledge and clinical skills. This demonstration occurs during the presentation to fellow students and optometrists, focusing on the clinical analyses of the case. Additionally, students must reflect on this case, demonstrating the appropriate management of ocular and visual problems. Through this reflection, the students can draw connections between knowledge learned in the classroom and their clinical learning experiences.18 From the presenters’ responses, it could be inferred that grand rounds as a teaching-learning method provided this reflective learning experience. Our findings reinforce previous research, which has reported that principles such as critical thinking and integration were stimulated during the reflection. Literature also suggests that going through reflective practice improves clinical skills.5,6,7
The main element contributing to the attendees’ positive experience was peer learning through the presentation of a peer’s personal clinical experience. Students recognized that they learned more from their peers and supported using grand rounds as a teaching-learning method. This might be due to their close association with their peers’ experience, their respect for the presenter’s work and the effort of standing in front of a group of people to present the case. Furthermore, the exposure to different, interesting and unique cases was acknowledged as a key factor that enhanced the learning for the attendees. It seems that students preferred a visual, practical teaching-learning method and perceived the presentation of a clinical experience beneficial, as well as the research component that also added to the knowledge enhancement.
The most significant finding of the data analysis on this experience was the voice of the participants urging educators to remember that they are merely students and should be treated as such. The success of this experience was overshadowed by an atmosphere that participants perceived as stressful, degrading, critical, judgmental and cruel. While we acknowledge that moderate stress can enhance learning19, it is important to exercise caution to avoid suppressing learning experiences by minimizing the occurrence of intimidation and aggressive behaviours. Students will take risks and engage in learning activities when they feel that they and the educator have a relationship of trust and respect.20 The data revealed the validity of Edmondson’s definition of psychological safety and the trust relationship between the student and educator, wherein students should have confidence that educators will not embarrass, disrespect, or punish them.21 The adverse impact of destructive criticism extended beyond the presenters and adversely affected the attendees as well. The absence of support and assistance they experienced could have led to disengagement from the learning experience. When examining previous research indicating that learning behaviour thrives on trust, respect, empathy and recognizing mistakes as integral to the learning process, it becomes evident that these elements were lacking during the grand rounds in this study.20
The overall data analysis indicated that students appreciate the educational value of grand rounds, suggesting early exposure as a recommended practice. This supports continuing with second-year attendance, although some participants will disagree. The authors believe that with this early exposure, the students are empowered to scaffold their theoretical and clinical knowledge progressively and, ultimately, their understanding and independence, which will favour their ability to do their own presentations in the future. It would prepare and encourage participation in discussions on clinical matters. Early exposure to clinical situations also motivates and fosters the integration of theory and clinical practice. This was confirmed by the responses of several fourth-year optometry students who expressed the opinion that, after having gone through this experience for three years, they recommended that even first-years become part of this teaching-learning exercise. This confirms the positive contribution of this experience over several years.
Limitations include the possibility of participants completing the questionnaire to please academic staff members despite the anonymization of the questionnaire. Upon reviewing the results, the authors maintain confidence that the responses genuinely reflect the participants’ experiences. This study offers valuable insights into the adaptation of teaching-learning pedagogy for grand rounds within a particular institution and with a specific cohort of students. However, due to this specificity, the findings cannot be generalized. Therefore, there is a need for additional research to explore students’ perspectives on grand rounds as a teaching-learning method.
Conclusion
The results of the study show that one of the main objectives of the grand rounds is to allow students to learn from each other and share their experiences. Optometry students in this program found grand rounds to be a site of valuable learning but emphasized the need for improvements in constructive feedback and creating a safer, more supportive learning environment.
References
- Agee N, Komenaka IK, Drachman D, Bouton ME, Caruso DM, Foster KN. The Effectiveness of Grand Rounds Lectures in a Community-Based Teaching Hospital. J Surg. Educ. 2009 Nov-Dec;66(6): 361-366. doi: 10.1016/j.jsurg.2009.07.006
- Herbert RS, Wright SM. Re-examining the Value of Medical Grand Rounds. Acad Med 2003 Dec;78(12): 1248-1525. doi: 10.1097/00001888-200312000-00013.
- Laibhen-Parkes N, Brasch J, Gioncardi L. Nursing Grand Rounds: A Strategy for Promoting Evidence-Based Learning Among Paediatric Nurses. J Pediatr Nurs. 2015 Mar-Apr;30: 338-345. doi: 10.1016/j.pedn.2014.07.008
- Fasbinder DJ, Heys DR, Holland GR, Keerthy A, Murdoch-Kinch CA, Inglehart MR. Grand Rounds for Dental Students: An Exploration. J Dent Educ. 2015 May;79(5): 510-522.
- Gardner G, Woollett K, Daly N, Richardson B, Aitken LM. Innovation in clinical learning for the acute hospital environment: Nursing grand rounds. Nurse Educ Today. 2010 Nov;30: 737-741. doi: 10.1016/j.nedt.2010.01.015
- Stieger S, Praschinger A, Kletter K, Kainberger F. Diagnostic grand rounds: A new teaching concept to train diagnostic reasoning. Eur J Radiol. 2011 Jun;78: 349-352. doi: 10.1016/j.ejrad.2009.05.015
- Sandal S, Iannuzzi MC, Knohl SJ. Can We Make Grand Rounds “Grand” Again? J Grad Med Educ. 2013 Dec;5(4): 560-563. doi: 10.4300/JGME-D-12-00355.1
- Jattan A, Francois J. Twelve tips for adapting grand rounds for contemporary demands. Med Teach. 2022 Feb;44(2):144-148. doi: 10.1080/0142159X.2021.1898573
- A Global Competency-Based Model of Scope of Practice in Optometry [Internet]. St. Louis, MO: World Council of Optometry; c2015 [cited 2023 November 10]. https://worldcouncilofoptometry.info/wp-content/uploads/2017/03/wco_global_competency_model_2015.pdf
- Kolb AY, Kolb,D. Experiential Learning Theory as a Guide for Experiential Educators in Higher Education. A Journal for Engaged Educators. 2017 Jun;1(1): 7-44.
- Husebø SE, O’Regan S. Reflective Practice and Its Role in Simulation. Clin Simul Nurs. 2015 Jul;11: 368-375. doi:1016/j.ecns.2015.04.005
- Maguire M, Delahunt B. Doing a thematic analysis: A practical, step-by-step guide for learning and teaching scholars. All Ireland Journal of Higher Education. 2017 Oct;9:3351. doi:10.62707/aishej.v9i3.335
- Burns N, Grove, S. The Practice of Nursing Research. 5th ed. Missouri: Elsevier Saunders; 2005.
- Nieuwenhuis J. Qualitative research designs and data gathering techniques. In Maree K, editor. First steps in research. Pretoria: Van Schaik. 2007.
- Castro FG, Kellison JG, Boyd SJ, Kopak A. A Methodology for Conducting Integrative Mixed Methods Research and Data Analyses. J Mix Methods Res. 2010 Sep;4(4): 342-360. doi: 1177/1558689810382916
- Taylor-Powell E, Renner M. Analysing Qualitative data [Internet]. Semantic Scholar; c2003. Available from: https://pdfs.semanticscholar.org/8ee4/a0c8532720200bb4359cf5a3741fac60ca74.pdf
- Polit DF, Beck CT. Essentials of nursing research – methods, appraisal and utilization. Philadelphia: Lippincott Williams & Wilkens; 2006.
- King AE, Joseph AS, Umland EM. Student perceptions of the impact and value of incorporation of reflective writing across a pharmacy curriculum. Curr Pharm Teach Learn. 2017 Sep;9: 770-778. doi: 10.1016/j.cptl.2017.05.010
- Córdova A, Caballero-García A, Drobnic F, Roche E, Noriega DC. Influence of Stress and Emotions in the Learning Process: The Example of COVID-19 on University Students: A Narrative Review. Healthcare (Basel). 2023 Jun;17;11(12):1787. doi: 10.3390/healthcare11121787.
- Johnson CE, Keating JL, Molloy EK. Psychological safety in feedback: What does it look like and how can educators work with learners to foster it? Med Educ. 2020 Jun;54(6):559-570. doi: 10.1111/medu.14154. PMID: 32170881.
- Edmondson AC. Psychological safety and learning behavior in work teams. Adm Sci Q. 1999;44(2):350-383. doi:2307/2666999.
Appendix


