
Cerebral Venous Sinus Thrombosis Signaled by Bilateral Optic Disc Edema and Unilateral Pre-retinal Hemorrhage
Mayra Rullán, OD, FAAO, Eva Wu, OD, and Jose M. De Jesus, OD, MD, MA, FAAO
Abstract
Cerebral venous sinus thrombosis (CVST) is a rare and potentially life-threatening condition. It has no age predilection and its presentation may be acute, sub-acute or chronic. Although clinical signs and symptoms are variable, headaches along with papilledema, dizziness and focal neurological deficits are commonly seen. The patient presented in this case developed bilateral disc edema and unilateral pre-retinal hemorrhage as a result of this condition. All aspects of patient care are discussed in detail. In addition, features of CVST including etiology, epidemiology, pathogenesis, clinical manifestations and treatment modalities are thoroughly reviewed and integrated into the discussion.
Key Words: cerebral venous sinus thrombosis, venous sinuses, cerebral spinal fluid headache, papilledema, pre-retinal hemorrhage
Background
Cerebral venous sinus thrombosis (CVST) is a rare, life-threatening condition. It has no age predilection and its presentation may be acute, sub-acute or chronic.1 Variability in the clinical manifestation of this disease often leads to the misdiagnosis of other neurological conditions such as idiopathic intracranial hypertension (IIH).2 Notwithstanding, a significant portion of patients with this condition present with optic nerve head swelling associated with headaches, dizziness and focal neurological deficits.3 Magnetic resonance venography (MRV) is the most efficient test for the diagnosis of cerebral venous sinus abnormalities. Thus, it has become the gold standard for confirming the diagnosis of CVST.4,5
This case report focuses on the proper approach to diagnosing, treating and managing CVST. A thorough review of the clinical aspects of CVST is presented to facilitate the understanding of the course of action taken to treat this patient. In addition, anatomy and physiology concepts of the central nervous system are integrated in the discussion to cultivate critical thinking. For third- and fourth-year students and optometry residents, the case report can reinforce clinical competence in neuro-ophthalmic care. In addition, first- and second-year students may acquire a better understanding of how to incorporate basic science concepts into their clinical training.
Student Discussion Guide
Case description
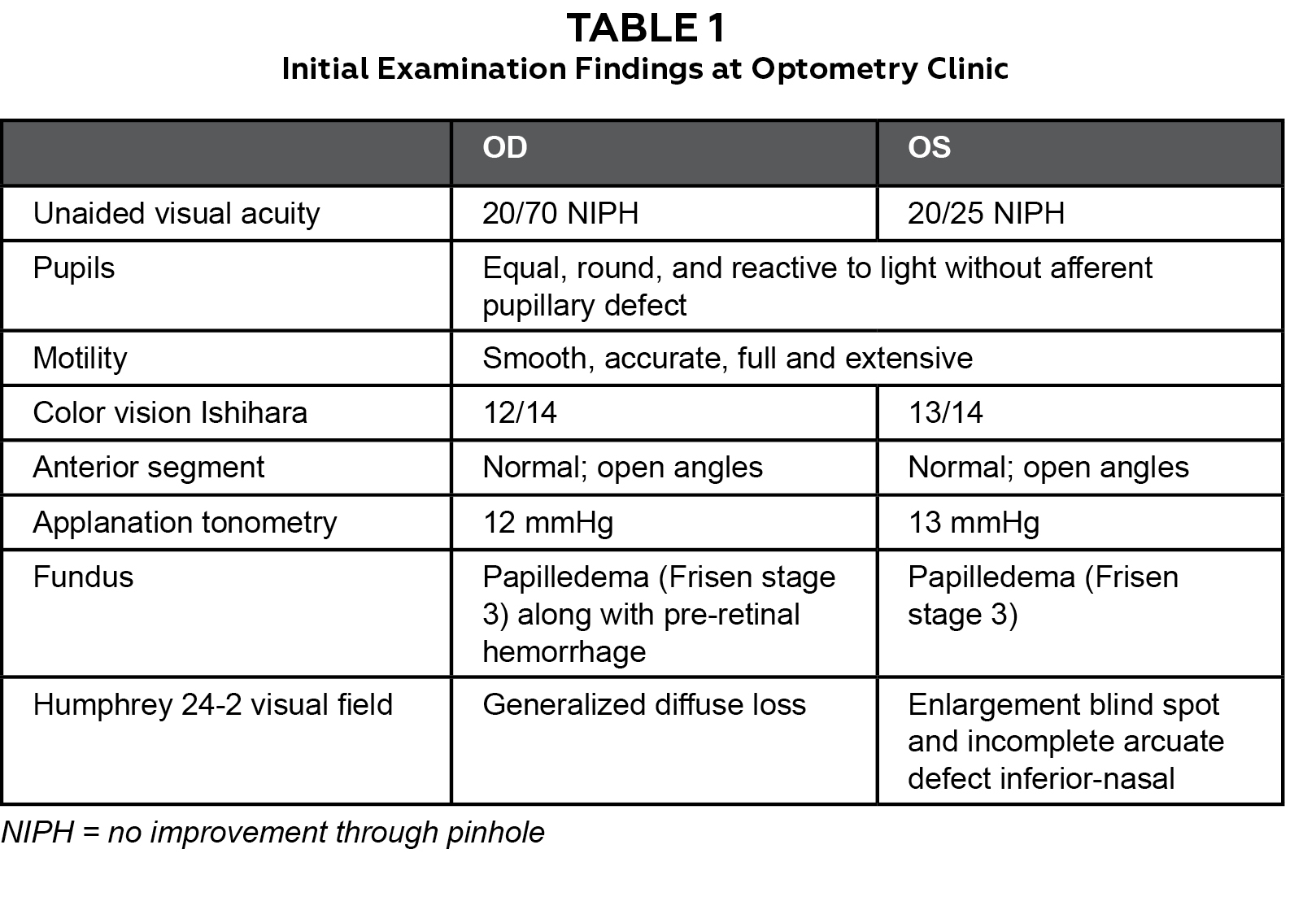
Table 1: Click to enlarge
A 22-year-old Hispanic male was referred urgently by a primary care physician concerning pain in the superior temporal side of his right eye that started eight days earlier. The pain was described as severe, sharp in quality and accompanied by photophobia. A few days after the onset of pain, the patient visited an ophthalmologist. The ophthalmologist diagnosed sinusitis, ordered a sinus X-ray and prescribed oral antibiotics. Per the patient, the result of the sinus X-ray was unremarkable. One day prior to visiting our clinic, the patient noted an acute drop in visual acuity in the right eye associated with the development of a “red central shadow.” No other visual symptoms were noted.
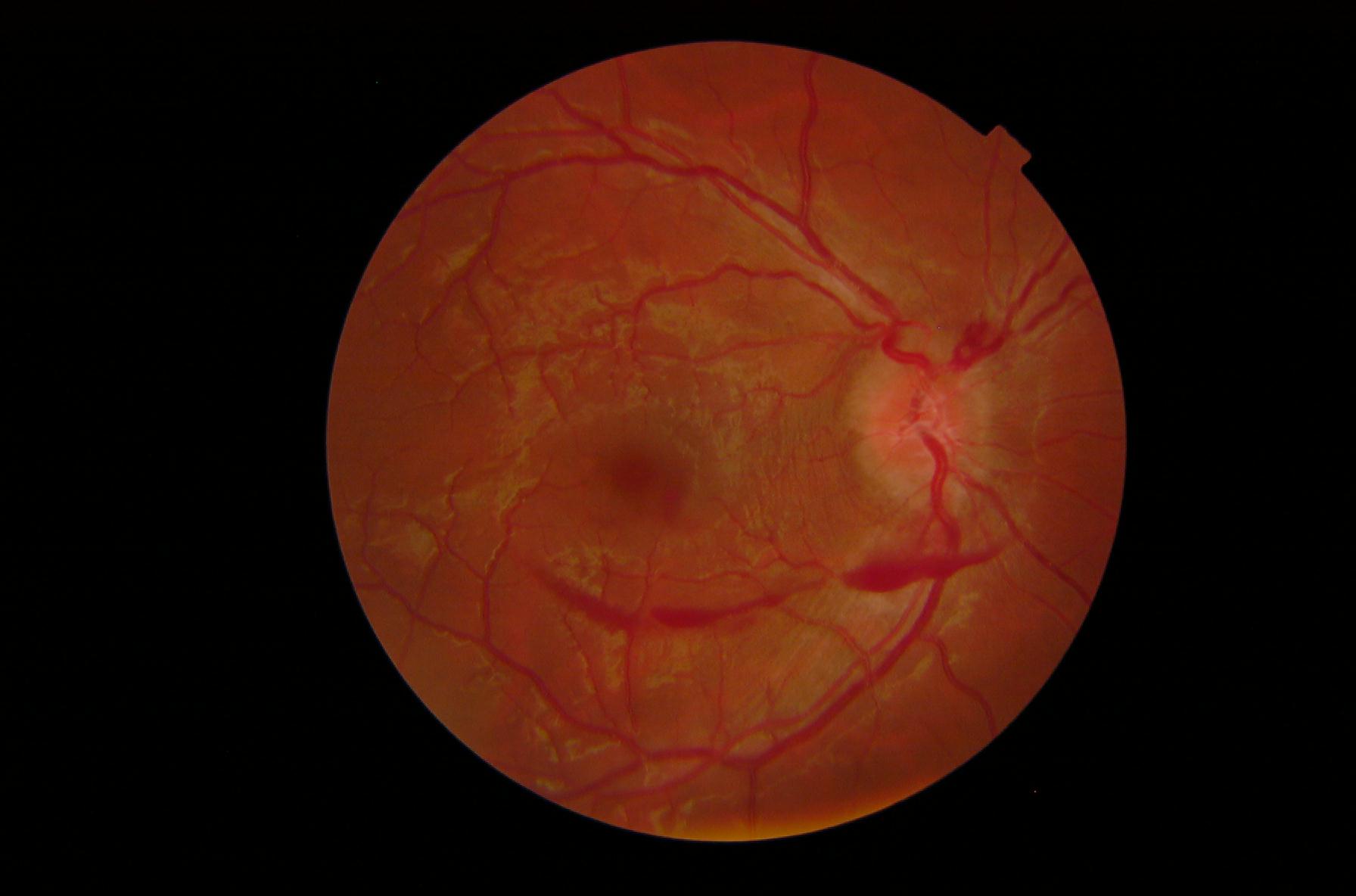
Figure 1A. Initial optometric examination revealed a pre-retinal hemorrhage OD.
Click to enlarge

Figure 1B. Initial optometric examination revealed papilledema OU.
Click to enlarge
Medical history reported was positive for bronchial asthma and sinusitis. The patient had been taking a 50-mg tablet of tramadol hydrochloride daily for pain until one day prior to visiting our clinic. He had no allergies to medications. Family history was positive for diabetes mellitus and hypertension. Social history revealed occasional alcohol consumption.
Entering unaided visual acuity in the right eye was decreased without improvement through pinhole (Table 1). Dilated fundus examination showed stage 3 (Frisen Scale) papilledema in both eyes along with a pre-retinal hemorrhage in the right eye (Figure 1A and 1B). Differential diagnosis of papilledema based on initial presentation included intracranial mass and cerebral/subarachnoid hemorrhage. The patient was immediately referred to the emergency department of a nearby medical center.
Emergency department visit
Computed tomography (CT) scans of the head without contrast were negative for intracranial mass and/or cerebral hemorrhage. Later the same day, the patient was transferred to a tertiary care hospital facility for a neuro-ophthalmology consult.
Tertiary care hospital facility

Table 2: Click to enlarge
By this time, visual acuity in the right eye had deteriorated dramatically (Table 2). The consultant neuro-ophthalmologist ordered magnetic resonance imaging (MRI) of the brain with and without contrast, which revealed subtle signs of sinus thrombosis of the transverse and sigmoid sinuses of the left hemisphere. The patient was then moved to the neurology ward with the recommendation for a lumbar puncture (LP) procedure. At the neurology ward, thrombosis of the transverse and sigmoid sinuses of the left hemisphere was confirmed. In addition, evidence of a cerebral mass, hemorrhage or herniation was ruled out. LP revealed an opening pressure of 350 mmH2O. The patient was started on acetazolamide 250 mg intravenously (IV) every six hours, and a MRV was ordered.
Follow-up care
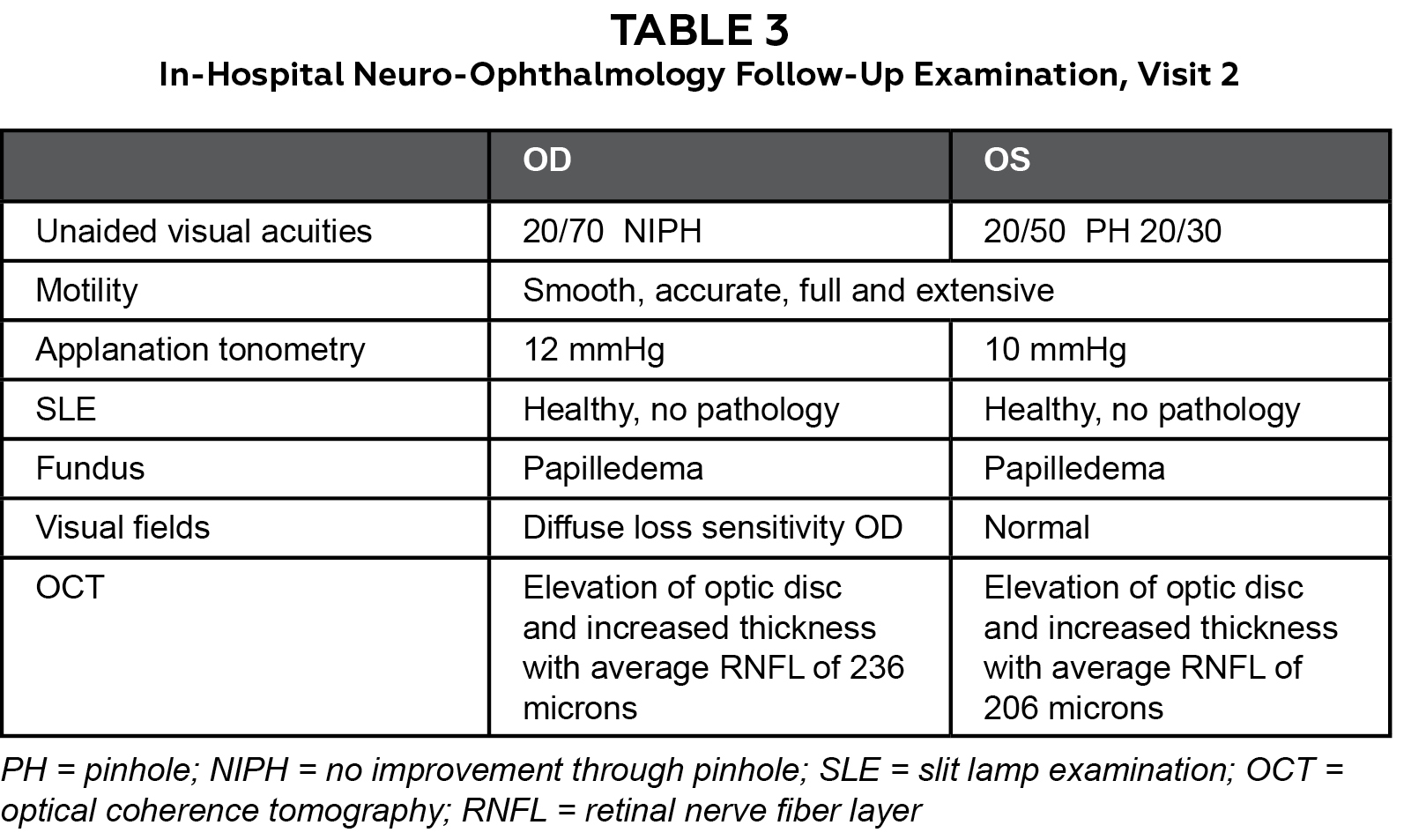
Table 3: Click to enlarge
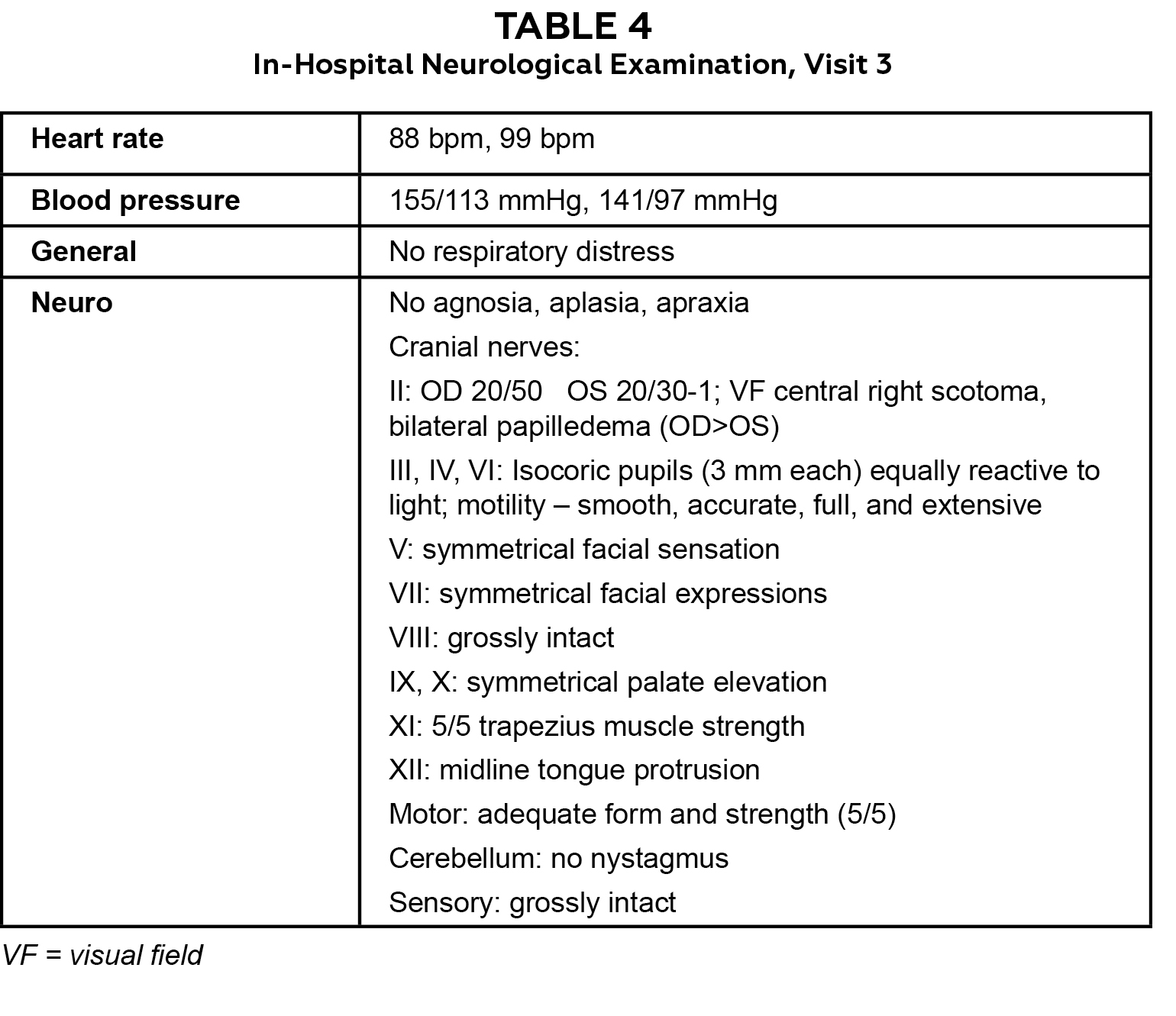
Table 4: Click to enlarge
One day after treatment, the patient showed significant improvement in vision in the right eye, despite optical coherence tomography (OCT) revealing substantial bilateral optic disc elevation (Table 3). The patient reported feeling better systemically. His headaches had subsided and he noted no other associated symptoms. Gross neurological examination was unremarkable (Table 4).
Coronal view on the MRV confirmed an acute transverse and sigmoid sinus thrombosis in the left hemisphere (Figure 2). IV acetazolamide 250 mg every six hours was continued, and the patient was started on enoxaparin (low molecular weight anticoagulant) 110 mg subcutaneously every 12 hours and warfarin sodium 5 mg orally once a day.

Table 5: Click to enlarge
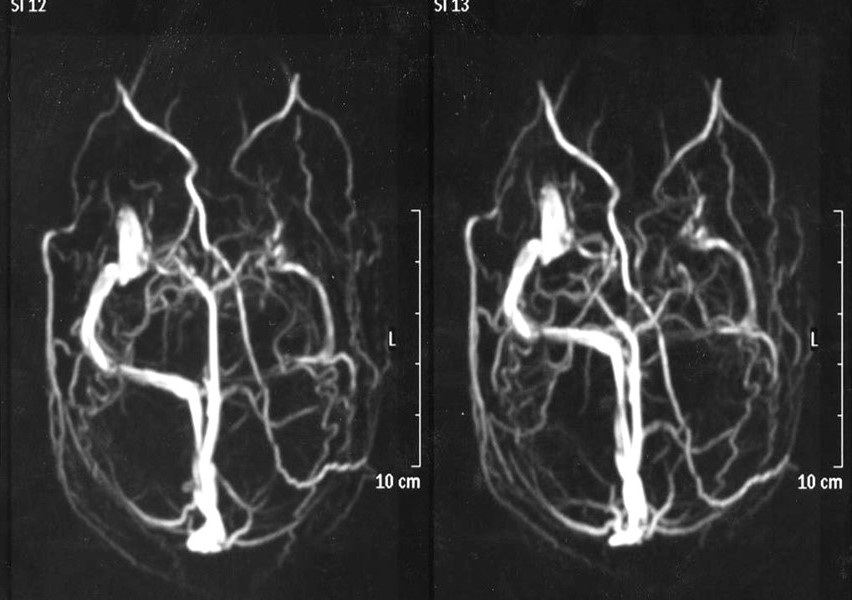
Figure 2. Magnetic resonance venography images showing acute thrombosis of the left transverse and sigmoid sinuses.
Click to enlarge
Results of a laboratory workup concerning possible etiologies of CVST were all unremarkable (Table 5). One week later, the patient was discharged from the hospital and a new treatment plan consisting of acetazolamide 250 mg orally every six hours and warfarin sodium 5 mg orally once a day was given.
One-month neurology follow-up visit
At the one-month neurology follow-up visit, papilledema had dramatically improved. Partial thromboplastin time, prothrombin time and international normalized ratio were re-evaluated. Treatment was kept the same.
Three-month neurology follow-up visit
Papilledema continued to improve. Acetazolamide dosage was reduced to 250 mg daily and warfarin was kept at 5 mg per day.
Six-month follow-up visit at eye clinic
At this visit, the patient reported dramatic improvement in vision and no symptoms. Treatment with oral acetazolamide had been discontinued but he was still taking 5 mg of warfarin daily. Vision examination showed 20/20 best-corrected visual acuity in both eyes (Table 6). Dilated fundus examination showed significant reduction of optic nerve head edema in both eyes and complete resolution of the pre-retinal hemorrhage in the right eye (Figure 3A and 3B).
 Table 6: Click to enlarge |
 Figure 3A. Dilated fundus photography at the six-month follow-up visit at the eye clinic showed complete resolution of the pre-retinal hemorrhage in the right eye. Click to enlarge |
 Figure 3B. Dilated fundus photography at the six-month follow-up visit at the eye clinic showed significant reduction of bilateral disc edema. |
Educator’s Guide
Key concepts
- Critical thinking in diagnosis and clinical approach in primary eye care
- The pathophysiology of the venous sinus system of the brain, and its impact on the eyes
- The importance of ensuring that patients understand their current situation and the seriousness of the matter at hand
Learning objectives
- Learn the importance of optic nerve head evaluation
- Gain basic knowledge of CVST, including signs, symptoms and basic testing
- Learn to differentiate life-threatening situations based on patient presentation
- Have a basic understanding of the types of headaches associated with papilledema and CVST, as well as the differential diagnosis of pain
- Understand the concept of papilledema vs. pseudopapilledema
- Gain knowledge on the differential diagnosis of true papilledema
- Be able to identify the different stages of papilledema according to the Frisen scale
- Understand the clinical significance of a pre-retinal hemorrhage in the presence of papilledema
- Gain expertise in patient education and management when urgent care is required
Discussion questions
1. Basic knowledge and concepts related to the case:
a. Describe the anatomy of the venous sinus system of the brain and its correlation with the optic nerve head anatomy
b. Describe the flow pathway of the cerebrospinal fluid and its impact on increased intracranial pressure
c. Discuss the different stages of papilledema according to the Frisen scale
d. Describe CVST and include risk factors
e. What is the pathophysiology of CVST?
f. What is the pathophysiology of the headache associated with CVST?
g. What indicates poor prognosis in CVST cases?
2. Differential diagnosis:
a. What are the likely diagnoses and differentials based on a patient’s presenting signs, symptoms and chief complaint?
b. What is the differential diagnosis of headaches based on the description of the headache and associated symptoms?
c. Determine the differential diagnosis based on the patient’s retinal findings
d. Mention the differential diagnosis for papilledema
e. Discuss the differentiating factors between true papilledema and pseudopapilledema
3. Critical-thinking concepts:
a. What could be the consequences if treatment is delayed?
b. Should the primary care optometrist follow up with the patient while the patient is under the care of the hospital facility?
c. Did the optometrist do the right thing by sending the patient to the ER immediately?
d. How important is it for the optometrist to ensure the patient understands his or her current eye health situation?
Literature Review
CVST is an uncommon condition that has gained recognition in recent years. This is primarily due to advancements in neuro-imaging technology. Although the outcome of the condition is relatively uneventful with proper treatment, it can be life-threatening if it is misdiagnosed or left untreated. It is more common in young adult women between 20 and 35 years of age. Associated risk factors include pregnancy, puerperium and the use of oral contraceptives.6 Diagnosis can be challenging because the condition can present with a wide variety of signs and symptoms that are seen in other neuro-ophthalmic disorders such as IIH. Foroozan et al. concluded in their retrospective study that the rate of occurrence of CVST in patients with presumed IIH was 9.4% (10 of 106 patients).7 However, more characteristically, patients with CVST present with a recent onset of an unusual headache or stroke-like symptoms without the usual vascular risk factors.7
Pathogenesis
The veins of the brain lie within the subarachnoid space and drain into the cerebral venous sinuses.8 The venous system is divided into the superficial and the deep venous system. The two structures belonging to the superficial venous system are the sagittal sinus and the more superficial cortical veins.8 The transverse sinus, straight sinus, sigmoid sinus, and the deeper cortical veins belong to the deep venous system.8 Venous blood from the cerebral sinuses ultimately reaches the heart via the internal jugular vein. An alteration in the normal blood flow, injury to the vascular wall, or hypercoagulability state can cause a venous blood clot.8 A venous clot in the brain may lead to a cerebral infarction. Consequently, this can cause a cerebral hemorrhage and/or increase intracranial pressure (IIP) due to the formation of a thrombotic vein occlusion or thrombotic sinus occlusion, respectively.9 Increased vascular permeability from a thrombotic vein occlusion results in extravascular fluid leakage along with coalescence of small hemorrhages ultimately producing a cerebral hematoma.9 In contrast, IIP is the most common sign seen in thrombotic sinus occlusions.9 This occurs when the cerebrospinal fluid (CSF) is not readily absorbed from the cerebral ventricles through the subarachnoid spaces and drained into the venous sinuses.9 As a consequence, the retrobulbar aspect of the optic nerve may begin to swell because of the accumulation of CSF in the proximal subarachnoid space. As the swollen nerve fibers pass through the optic foramen and enter the globe they get compressed and engorge, thus provoking decreased axoplasmic flow. Axoplasmic stasis ultimately results in optic disc edema. Retinal hemorrhaging with vitreous spill may also result from IIP.10 This occurs when the retinal venous vasculature collapses as a result of an increase in venous pressure relative to the retinal arterial pressure.11
Epidemiology, etiology and risk factors

Table 7: Click to enlarge
The incidence of CVST in the general population is approximately three to four cases per million and seven cases per million among children of which 50% are younger than three months.9 Although it can occur at any of the sinuses, the sagittal sinus and the lateral (transverse) sinuses are the most commonly affected (70-85% incidence).1,6 Multiple conditions and risk factors are associated with CVST (Table 7). Nonetheless, direct involvement, such as mechanical trauma during surgery or a consequential injury after a lumbar puncture, has been identified as the cause in approximately 85% of patients. Prothrombotic effects associated with the use of oral contraceptives have also been linked to the disease.9 Approximately 75% of the adult population with CSVT are females. This statistic has a positive association with the increased prevalence of young adult women using oral contraceptives.1 Pregnancy and genetic predisposing mutations such as factor V Leiden may also be influencing factors. Cases of CVST in pregnant women during their last trimester and postpartum period have been documented. Moreover, Allroggen et al. concluded in their study that the chances of developing CVST in a genetically predisposed female of childbearing age taking oral contraceptives is much higher than the normal female counterpart.6
Clinical manifestations
The onset of CVST may be acute (1-3 days), sub-acute (4-14 days) or chronic (more than 14 days).1,12 This variability in initial presentation can create a dilemma regarding the appropriate diagnostic approach. Hence, a proper assessment of signs and symptoms is of utmost importance. Headache is the most repeatable clinical manifestation of CVST. It is present in more than 90% of the cases.5 In their retrospective study, Wasay et al. found that 68% of the patients with CVST had a headache accompanied by a neurological deficit on initial presentation, while in the remaining 32% of the patients headache was the only symptom.12 Notwithstanding, headaches in CVST can present in a variety of forms. They may mimic a thunderclap type headache like is seen in patients with a subarachnoid hemorrhage as well as a throbbing headache that may occur during a migraine attack. Therefore, it is imperative to include CVST in the differential diagnosis when headaches accompany a neurological deficit(s) as well as in headaches that may suggest an impending neurological injury.13 Localization of headache may also be a good indicator of CVST. A correlation has been seen between localized headaches and thrombosis of the transverse and sigmoid sinuses.12 In addition, neurological deficit is observed in the majority of patients with CVST. Usual symptoms include local and generalized seizures, hemiparesthesia, hemiparesis, ataxia and cranial nerve VI palsy.5

Table 8: Click to enlarge
Ocular manifestations occur in approximately half of the patients with CVST.14 Papilledema is the most common ocular sign observed. IIP causes axoplasmic stasis leading to accumulation of cellular waste products and subsequent optic nerve edema. Optic nerve head (ONH) elevation due to papilledema, as well other conditions, may be observed on binocular fundus examination. However, accompanying peripapillary signs such as obscuration of retinal vessels, nerve fiber layer hemorrhages and retinal folds (Paton’s lines) are characteristic of papilledema (Table 8). Extra-retinal hemorrhaging may also be observed in CVST as a result of capillary collapse provoked by increased retinal venous pressure at other layers of the retina. Depending on the layer involved, blood spill can be found adjacent to the vitreous parenchyma (between the posterior vitreous base and the internal limiting membrane (ILM) and/or at the pre-retinal interphase (posterior to the ILM and anterior to the nerve fiber layer).15
Diagnostic tools
MRI and MRV of the brain are the most sensitive tests for diagnosing CVST.4 If CVST is suspected, the initial standard approach is to order an MRI of the brain. A positive test is interpreted by the presence of a hyperintense signal from the thrombosed sinus(es). Following, due to its specificity, an MRV should be obtained to rule out CVST.16 A confirming positive result will demonstrate an absence of flow in the corresponding thrombosed region.17,18 Despite the effectiveness and non-invasive modality of this approach, other anatomical abnormalities such as septation of the venous sinuses can be incorrectly identified as CVST.19 Thus, a more invasive approach such as a cerebral angiography (CA) may be warranted in cases where the diagnosis of CVST through magnetic resonance is uncertain.
Alternatively, CT scan may be employed to diagnosis CVST if the use of magnetic resonance technology is contraindicated. It will also show a hyperintense signal on the suspected thrombosed area, which should be further confirmed through a computed tomographic venography (CVT). However, this approach is far less sensitive and specific than magnetic resonance technology.20 Hence, CA must be performed if the diagnosis of CVST is doubtful.
Treatment
The management of CVST involves anticoagulation therapy and the reduction of IIP. For the initial anticoagulation treatment, the patient is usually hospitalized, requiring intravenous or subcutaneous administration of low molecular weight heparin. After stabilization, the patient is usually dismissed from the hospital and treated with oral anticoagulants for months to years.9 An acute thrombotic event may be treated with intravenous administration of thrombolytic agents within three hours of the initial presentation. Tissue plasminogen activator (TPA) is usually the preferred agent. However, this treatment approach does not necessarily improve the usual outcome. Approximately 30% of patients treated with TPA during an acute stage have a better outcome in comparison to patients not receiving thrombolytic treatment during the same period.21 IIP reduction requires in-hospital intravenous administration of acetazolamide. This is followed by oral acetazolamide treatment for weeks to months. In refractory cases, a lumbar puncture and/or a lumboperitoneal shunt is usually performed.1 In addition, intractable IIP leading to papilledematous optic nerve atrophy may require an optic nerve head fenestration procedure to decrease ONH swelling.22 With appropriate treatment the prognosis of CVST is favorable. Prospective studies reveal that the great majority of patients who are properly treated fully recover.9 A poor outcome is usually a result of severe clinical features manifested at the time of initial presentation.23,24 These may include extensive thrombopathy, deep sinus involvement and altered levels of consciousness.
Discussion
CVST is a neurological treatable disease that has good prognosis if diagnosed early. In the case presented, the optometrist immediately recognized the significance of neurological signs and symptoms and ensured that the patient received prompt evaluation and treatment, resulting in a good outcome. The patient’s presentation of severe unilateral headache in association with bilateral optic nerve swelling, as detected through fundus examination, are what incited the clinician’s suspicion of a cranial pathology that needed immediate attention. Aside from CVST, other diagnostic considerations with this type of presentation should include subarachnoid hemorrhage, intracranial aneurysm, cervical artery dissection, stroke, intracranial hemorrhage, reversible cerebral vasoconstriction syndrome, and posterior reversible leukoencephalopathy.25
As in other neuro-ophthalmic conditions, the clinical distinction between papilledema and pseudopapilledema in the presence of an elevated optic disc must be addressed when CVST is suspected. Clinical signs that prompt the suggestion of papilledema in the presence of an elevated optic disc include blurred disc margins, peripapapillary nerve fiber layer splinter-type hemorrhages with exudation and peripapillary retinal folds known as Paton’s lines. Pseudopapilledema is often seen secondary to optic nerve head drusen, where the nerve looks elevated due to the presence of “buried” hyaline bodies. OCT is an excellent imaging test to help differentiate true disc edema from pseudopapilledema.16,26 In pseudopapilledema secondary to optic nerve drusen, OCT will show a lumpy and bumpy internal contour of the optic nerve head, while in papilledema a sideways “lazy V” pattern of the subretinal hyporeflective space is typically observed.27 Fundus autofluorescence (FAF) imaging and B scan ultrasonography are other diagnostic instruments that can be employed to rule out optic nerve drusen. It is also essential to consider all potential causes of optic nerve head swelling aside from papilledema. Optic nerve head swelling due to other etiologies may include malignant hypertension, diabetic papillitis, anemia, central retinal vein occlusion, neuroretinitis, uveopapillitis, optic neuritis, anterior ischemic optic neuropathy, Leber’s optic neuropathy and retrobulbar optic nerve mass, among others. Functional ocular deficits may also occur in CVST. Eso-binocular diplopia may develop due to IIP compression on the abducens nerve. This cranial nerve is the most commonly affected due to its long trajectory through the subarachnoid space. In addition, static automated perimetry as well as Goldmann dynamic perimetry may reveal an enlargement of the blind spot. Ischemic optic nerve head damage seldom occurs, thus afferent pupillary defects and dyschromatopsia are usually absent.
Discerning urgency and prompt referral
It is important for primary eyecare physicians to be receptive to patients’ concerns as well as their signs and symptoms and to have the ability to discern the necessity of urgent care. In this case, for example, the patient presented with a severe unilateral headache accompanied by visual disturbances associated with bilateral papilledema and a pre-retinal hemorrhage in the right eye. Initially, this clinical scenario suggested the possibility of IIH; however, the patient did not fit the typical profile for IIH (overweight female of childbearing age).10 It is important to remember that IIH is a diagnosis of exclusion and does not necessarily require urgent action. Therefore, other conditions that may require prompt management must be ruled out. CVST must be high in the list of differentials when bilateral papilledema presents with retinal hemorrhages.28 In addition, other conditions such as tumors, infections, occlusions and trauma must be excluded. Assurance of reaching the proper personnel is imperative in urgent care management. Therefore, the primary eyecare physician should contact the referring facility to ensure that the patient is attended promptly by the appropriate personnel.
Patient education
Proper patient education is especially vital in urgent care management. The primary eyecare physician must ensure that the patient acknowledges the status of his/her condition and the subsequent care that may be required. This provides patients with the opportunity to ask concerning questions and helps them to be mentally prepared for the forthcoming process. In addition, it helps to ensure patient compliance with seeking care.
Conclusion
CVST should be included in the differential diagnosis of patients presenting with bilateral disc edema or papilledema and headaches. The great “mimicker” would be IIH, especially if patients are young women. The patient in this case was a young male with headaches, bilateral disc edema and a preretinal hemorrhage in the right eye. A CT scan did not reveal any abnormalities, and the preliminary diagnosis was IIH. Results of the MRI and MRV that were ordered showed the presence of a venous sinus occlusion. CVST can result in permanent vision loss and death if it is not treated promptly. Hence, an urgent approach to the care of these patients can prevent visual function loss and save their lives.
References
- Kimber J. Cerebral venous sinus thrombosis. QJM. 2002;95(3):137-142.
- Biousse V, Ameri A, Bousser MG. Isolated intracranial hypertension as the only sign of cerebral venous thrombosis. Am Acad Neurology. 1999;53:1537-1542.
- Crassard I, Bousser MG. Cerebral venous thrombosis. J Neurophthalmol. 2004;24(2):156-163.
- Connor S, Jarosz J. Magnetic resonance imaging of cerebral venous sinus thrombosis. Clin Radiol. 2002;57:449-461.
- Masuhr F, Mehraein S, Einhaupl K. Cerebral venous and sinus thrombosis. J Neurol. 2004;251:11-23.
- Allroggen H, Abbott RJ. Cerebral venous sinus thrombosis. Postgrad Med J. 2000;76:12-15.
- Lin A, Foroozan R, Danesh-Meyer HV, De Salvo G, Savino PJ, Sergott RC. Occurrence of cerebral venous sinus thrombosis in patients with presumed idiopathic intracranial hypertension. Ophthalmology. 2006;113(12):2281-2284.
- Kilic T, Akakin A. Anatomy of cerebral veins and sinuses. Front Neurol Neurosci. 2008;23:4-15.
- Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791-1798.
- Hauser D, Barzilai N, Zalish M, Oliver M, Pollack A. Bilateral papilledema with retinal hemorrhages in association with cerebral venous sinus thrombosis and paroxysmal nocturnal hemoglobinuria. Am J Ophthalmol. 1996;122(4):592-593.
- Ganesan P, He S, Xu H. Modelling of pulsatile blood flow in arterial trees of retinal vasculature. Med Eng Phys. 2011 Sep;33(7):810-23.
- Wasay M, Kojan S, Dai AI, Bobustuc G, Sheikh Z. Headache in cerebral venous thrombosis: incidence, pattern and location in 200 consecutive patients. J Headache Pain. 2010;11:137-139.
- Cumurciuc R, Crassard I, Valade D, Bousser MG. Headache as the only neurological sign of cerebral venous thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatry. 2005;76(8):1084-1087.
- Wang D, Fang B, Wei S. Analysis of clinical features of ocular presentation in cranial venous sinus thrombosis. Eur J Med Res. 2011;16(7):324-327.
- Berdahl JP, Mruthyunjaya P. Vitreous hemorrhage: diagnosis and treatment. EyeNet Magazine (American Academy of Ophthalmology). March 2007. Available from: https://www.aao.org/publications/eyenet/200703/pearls.cfm.
- Lee AG, Brazis PW. Magnetic resonance venography in idiopathic pseudotumor cerebri. J Neuroophthalmol. 2000;20(1):12-13.
- Parmar H, Gandhi D, Mukherji S, Trobe JD. Restricted diffusion in the superior ophthalmic vein and cavernous sinus in a case of cavernous sinus thrombosis. J Neuroophthalmol. 2009;29:16-20.
- Gandhi D. Computed tomography and magnetic resonance angiography in cervicocranial vascular disease. J Clin Neuroophthalmol. 2004;24(4):306-314.
- White JB, Kaufmann TJ, Kallmes DF. Venous sinus thrombosis: a misdiagnosis using MR angiography. Neurocrit Care. 2008;8(2):290-2.
- Lee AG, Johnson MC, Policeni BA, Smoker W. Imaging for neuro-ophthalmic and orbital disease-a review. Clinl Expl Ophthalmol. 2009;37:30-53.
- The National Institute of Neurological Disorders and Stroke rt-PA Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333:1581-1588.
- Purvin VA, Trobe JD, Kosmorsky G. Neuro-ophthalmic features of cerebral venous obstruction. Arch Neurol. 1995;52:880-885.
- De Bruijn SFTM, de Haan RJ, Stam J. Clinical features and prognostic factors of cerebral venous sinus thrombosis in a prospective series of 59 patients. J Neurol Neurosurg Psychiatry. 2001;70:105-108.
- Scott CJ, Kardon RH, Lee AG, Frisen L, Wall M. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010;128(6):705-711.
- Ju YE, Schwedt TJ. Abrupt-onset severe headaches. Semin Neurol. 2010 Apr;30(2): 192-200.
- Karam EZ, Hedges TR. Optical coherence tomography of the retinal nerve fiber layer in mild papilledema and pseudopapilledema. Br J Ophthalmol. 2005;89(3):294-298.
- Johnson LN, Diehl ML, Hamm CW, Sommerville DN, Petroski GF. Differentiating optic disc edema from optic nerve head drusen on optical coherence tomography. Arch Ophthalmol. 2009;127(1):45-49.
- Cohen SM, Keltner JL. Thrombosis of the lateral transverse sinus with papilledema. Arch Ophthalmol. 1993;111(2):274-5.
- Masuhr F, Mehraein S, Einhaupl K. Cerebral venous and sinus thrombosis. J Neurol. 2004 Jan;251(1):11-23.
- Lemke DM, Hacein-Bey L. Cerebral venous sinus thrombosis. J Neurosci Nurs. 2005;37(5):258-264.
- Tait C, Baglin T, Watson H, et al. Guidelines on the investigation and management of venous thrombosis at unusual sites. Br J Haematol. 2012;159:28-38.
- Wall M. Idiopathic intracranial hypertension. Neurol Clin. 2010 August;28(3):593-617.
- Scott CJ, Kardon RH, Lee AG, Frisén L, Wall M. Diagnosis and grading of papilledema in patients with raised intracranial pressure using optical coherence tomography vs clinical expert assessment using a clinical staging scale. Arch Ophthalmol. 2010;128(6):705-711.
- 34. Nguyen HS, Haider KM, Ackerman LL. Unusual causes of papilledema: two illustrative cases. Surg Neurol Int. 2013;4:60.

