
PEER REVIEWED
Management of Adult Unilateral Esotropia
Jacqueline Dang, OD, FAAO, Ida Chung, OD, FAAO, FOVDR
Abstract
Unilateral esotropia in an adult patient with diplopia as the primary symptom presents a challenging case for eyecare practitioners due to the numerous potential etiologies. A thorough medical and ocular history, along with a comprehensive eye examination and appropriate adjunct testing is essential to determine the underlying cause of the strabismus. This teaching case report outlines the evaluation process for esotropia in an adult patient and explores various treatment modalities and techniques to enhance the patient’s quality of life.
Keywords
Background
Strabismus is a well-known diagnostic challenge for eyecare practitioners, and diagnosing it in an adult patient is particularly demanding due to the potential etiologies, including neurological dysfunction, orbital disease, binocular vision disorders or central nervous system injury.¹ An observational study analyzed the prevalence of binocular diplopia and its associated causes, identifying vasculopathy (28%), trauma (24.6%), decompensating heterophorias (11.25%), tumors (4%), and inflammatory conditions (4%) as common contributors.² A thorough ocular examination with targeted ancillary testing is essential to accurately diagnose and manage strabismus, determine the need for immediate referral, and assess whether the condition poses a vision- or life-threatening risk. Long-standing phorias may present with intermittent diplopia due to decompensation triggered by factors such as fever, trauma or stress.² In this case, the patient’s history and symptom timeline suggest a decompensated phoria following a stressful event. Recognizing the distinguishing features of pathological vs benign strabismus is critical for establishing an accurate and effective treatment plan.
This case report is intended for third- and fourth-year optometry students and eyecare clinicians.
Case Description
On August 15, 2023, a 39-year-old female presented with a chief complaint of intermittent, binocular diplopia at distance, particularly when driving. She described the diplopia as horizontal without vertical disparity, noticing it in both left and right peripheral gazes, with resolution upon closing one eye. Her symptoms worsened at the end of the day or when she was fatigued.
The patient reported that her symptoms began in her teenage years and believed her eye turn was undiagnosed in childhood. The diplopia remained manageable until her pregnancy in 2020, which she described as an intense, stressful event, leading to a noticeable increase in the frequency of her diplopia.
In 2020, at the age of 36, she was officially diagnosed with strabismus by her primary optometrist. She was prescribed her first pair of prism glasses, which alleviated the distance diplopia. She had received her first glasses for myopia at age 14 and had since preferred wearing contact lenses full-time, as she disliked wearing glasses. Her current contact lens prescription was right eye -4.00 diopter sphere (DS) and -3.50 in the left. Her prism glasses had a total of eight prism diopters base out, which she wore over her contact lenses as needed for driving.
The patient’s medical history was unremarkable for disease or significant conditions. However, she was involved in a car accident at age nine, going through the back of a car window. There was no reported diagnosis of concussion, eye injury or overnight hospital stay.
On examination, her corrected visual acuities at both distance and near were 20/20 in both eyes with contact lenses alone. Extraocular movements were full in both eyes. Pupils and confrontation fields were unremarkable. A cover test without prism glasses revealed a constant 12 prism diopter left esotropia in all nine gazes, demonstrating comitancy.
Randot stereopsis testing showed no global stereopsis and local stereopsis of 200 arc seconds, with no improvement when wearing her prism glasses. Worth 4 Dot testing without her prism glasses demonstrated uncrossed diplopia at 40 cm. With the prism glasses, she achieved fusion at 20 cm but experienced intermittent alternating suppression at 4-5 feet. Bagolini lens testing indicated normal correspondence, and visuoscopy showed no eccentric fixation in either eye. See Appendix A for Worth 4 Dot and Bagolini test procedures and interpretation guidelines.
Step vergence ranges, performed with her prism glasses, produced the following results:
- Distance: base out (BO): 16/18/16, base in (BI): X/4/2
- Near: base out (BO): X/35/30, base in (BI): X/6/2
Anterior and posterior segment examinations were unremarkable.
Treatment options were discussed, and the patient opted to begin in-office vision therapy as soon as possible.
Due to her strong aversion to wearing glasses, she was highly motivated to reduce her dependence on prism glasses. The initial vision therapy protocol focused on monocular ocular motor and accommodative activities to equalize visual skills between both eyes. By Week 4, anti-suppression activities were introduced, with an emphasis on peripheral fusion and binocular skills.
At Week 9, the patient underwent an exercise using an optokinetic drum in both left and right gazes, which triggered diplopia while the patient maintained primary gaze. The drum was placed on the patient’s right and left fields, while maintaining fixation in primary gaze. To address this peripheral trigger, binasal occlusion taping was applied to her habitual spectacle prescription without prism. This method was intended to alleviate the onset of diplopia, offering an alternative to wearing prism glasses over her contact lenses. After the application of the binasal taping, the optokinetic drum was spun again, and the patient no longer experienced diplopia in primary gaze. Table 1 provides the pre- and post-examination findings after 12 sessions of vision therapy. See Appendix B for details of the in-office vision therapy activities for the first 12 weeks.
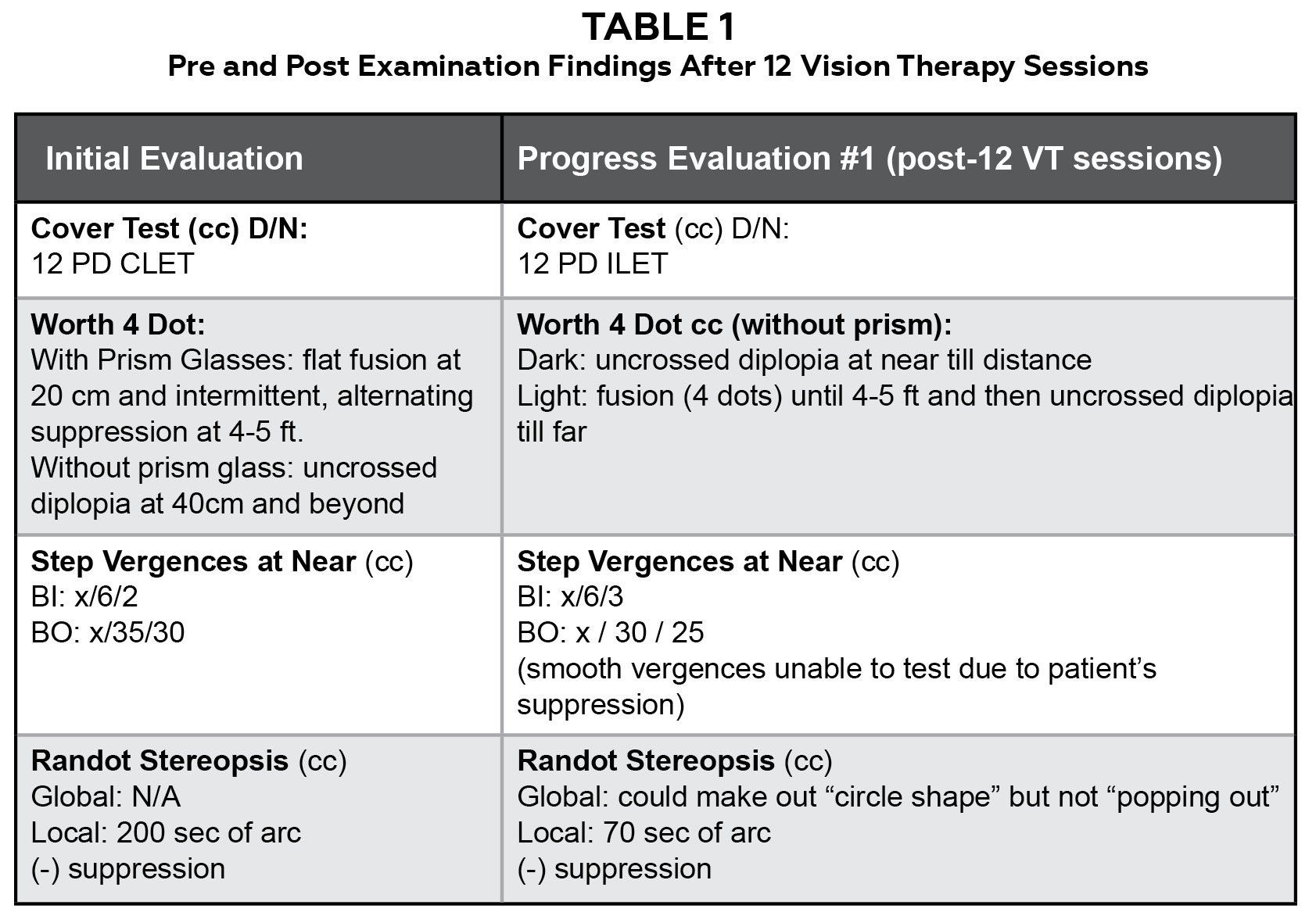
Table 1. Pre- and Post-Examination findings After 12 Vision Therapy Sessions. Click to enlarge
Around Week 19, the patient started experiencing constant, distance blur with her habitual contact lenses and an updated refraction showed a decrease in her myopia: right eye: -2.50 -1.00 x 015 DS, left eye: -3.00 DS with 20/20 acuities at distance and near.
After Week 21, the patient was due for a comprehensive annual examination. She mentioned that her current habitual contact lenses and spectacle glasses were making her distance vision constantly blurry. The patient wore the glasses while driving when necessary.
Dry refraction with primary optometrist before vision therapy was the following:
- Right Eye: -4.00 – 1.00 x 010
- Left Eye: -3.75 DS
Dry subjective refraction with us after 21 weeks of vision therapy was the following:
- Right Eye: -2.50 – 1.00 x 015, 20/20
- Left Eye: -3.00 DS, 20/20
- Add: +1.25, 20/20
The add power was determined based on the fused cross cylinder and subjective findings during the refraction.
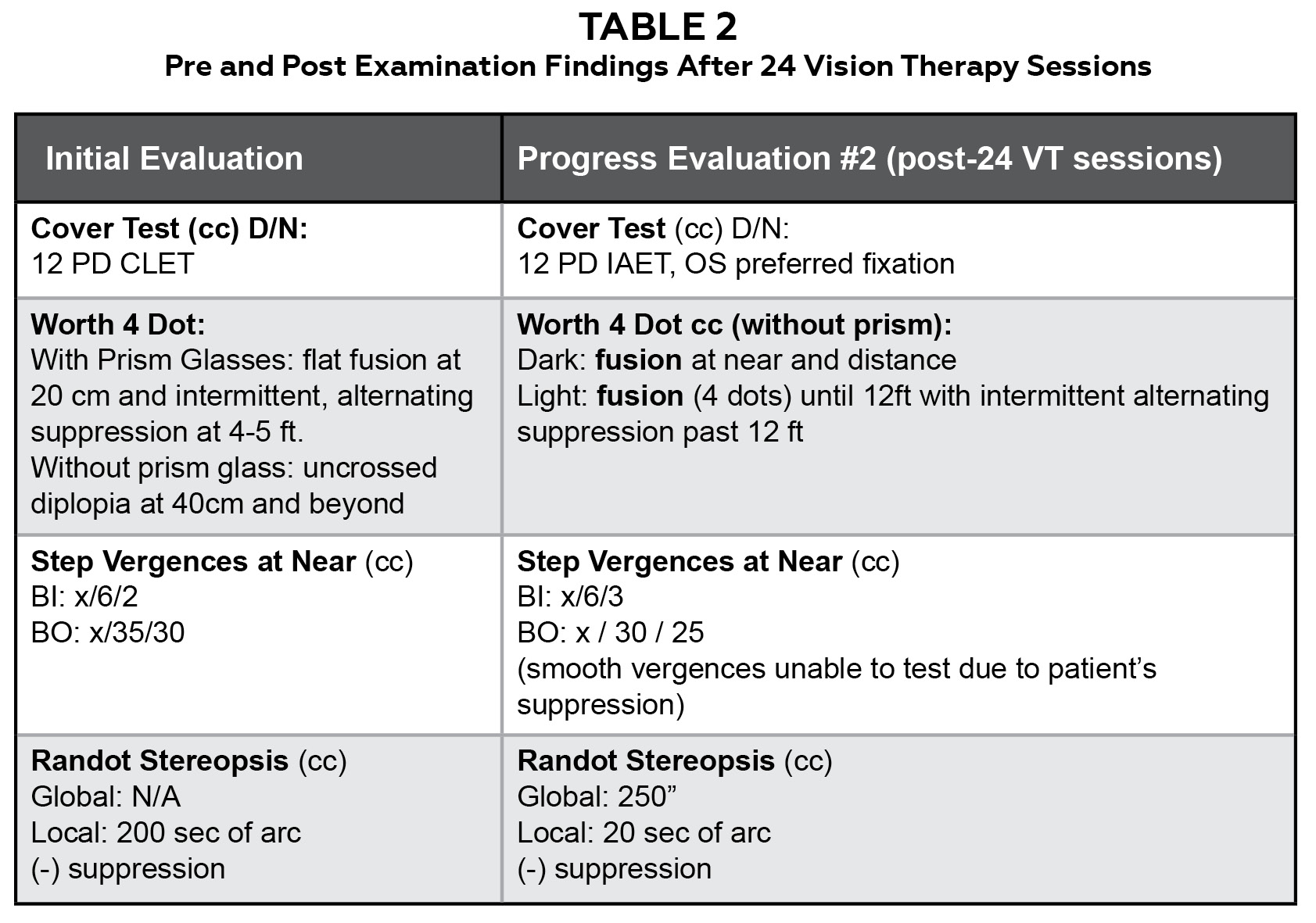
Table 2. Pre- and Post-Examination findings After 24 Vision Therapy Sessions. Click to enlarge
After 24 weeks of in-office vision therapy, the patient graduated from the program, having successfully achieved her therapy goals. The patient was able to control her diplopia and did not have to wear the prism glasses nor the binasal occlusion taping while driving. She was able to drive with only her contact lens prescription. The patient’s main primary goal was to not have to wear glasses, and she has been able to drive without her prism glasses since completing vision therapy. She does still note diplopia onset when she is tired at the end of a long day, but she is able to control it and it is much more manageable. Table 2 provides the examination findings after 24 therapy sessions. See Appendix C for details of the in-office vision therapy activities by week for the remaining 12 sessions. She was advised to continue maintenance home therapy 2-3 times per week to preserve her visual skills. She was given two exercises to practice at home: Clear and Opaque Eccentric Circles and Brock String in nine gazes. The patient was to taper the home maintenance exercises to 1-2 times per week after 6 months. A 6-month progress evaluation was scheduled to monitor her symptom resolution and overall progress.
Education Guidelines
Key Concepts
-
- Possible causes of unilateral esotropia in adults
- Special ancillary testing in sensorimotor evaluations
- Management and treatment strategies for strabismus in adults
- Individualized Vision Therapy programming with specific goals
Learning Objectives
After this case discussion, participants should be able to:
-
- Differentiate unilateral esotropia from other types of strabismus based on ocular alignment and associated features.
- Explore the various etiological factors contributing to esotropia, such as refractive errors, accommodative factors, neurological dysfunctions, vasculopathies and space-occupying lesions.
- Demonstrate proficiency in using diagnostic techniques and special ancillary testing to assess and diagnose the different types of esotropia.
- Develop effective communication skills to counsel patients about the diagnosis, treatment options and expected outcomes associated with esotropia.
- Explain the impact of an individualized in-office vision therapy program for strabismic patients and its significance in improving their quality of life.
Discussion Questions
Knowledge and Concepts
-
- How is esotropia classified?
- What is the difference between adult esotropia and pediatric esotropia?
- What tests are used to evaluate esotropia?
Differential Diagnosis
-
- What are the differential diagnoses for adult onset esotropia?
- What are the key history questions to ask?
- What are the key diagnostic tests for evaluation?
Management
-
- How do you determine if prism is indicated?
- How do you determine the amount of prism to prescribe?
- What is the role of binasal occlusion?
- How do you determine if vision therapy is indicated?
- How do you determine when a surgical consult is warranted?
- How do you assess the prognosis for success?
Creating an Individualized In-Office Therapy Program
-
- How do you determine the duration of treatment?
- What is the sequence of therapy?
- How do you select therapy activities?
- What is the role of home therapy?
- How do you determine when to graduate the patient?
Assessment of learning objectives
-
- Students can be asked to classify the types of esotropia in both a classroom and clinical setting.
- Facilitate case discussions to conduct components of patient history and pertinent questions relative to the significance of the case, in addition to creating a management strategy.
- Evaluate students on how to rule out each differential diagnosis for adult esotropia by listing correlating ancillary testing.
Discussion
Teaching Methodology
The clinician and students can facilitate a case discussion in either a small-group clinical setting or a classroom setting, with students divided into small groups of two to four. To enhance understanding, provide students with case findings and ask them to formulate the likely diagnosis. Have students create a table listing the differential diagnoses of esotropia, including major symptoms, signs and key diagnostic findings for each type.
To facilitate history-taking skills, students can role-play as clinicians asking pertinent history questions for a patient with adult-onset esotropia. For developing ancillary testing skills, students can alternate between being the student clinician and the simulated patient, with simulated responses provided by the instructor. Student clinicians should be asked to explain the reasons for selecting specific tests and to interpret the simulated findings.
Based on the provided test findings and patient goals, students can write a 12-week individualized therapy plan that appropriately addresses the patient’s needs. To enhance communication skills, student clinicians can practice providing patient education, explaining the diagnosis, elements of the prescribed treatment plan and anticipated treatment outcomes.
History Questions and Key Findings to Differentiate Between Adult-Onset vs Childhood Esotropia
When conducting a strabismus evaluation on a patient with the chief complaint of diplopia, the first step is a detailed, comprehensive ocular and medical history. A thorough assessment of the patient’s current diplopia symptoms will assist the clinician in developing a systematic approach to determine the nature of the strabismus throughout the evaluation. Gathering answers to as many history-of-present-illness (HPI) questions related to the diplopia will help rule out differential diagnoses.
The patient characterized her diplopia as binocular, since it was resolved by monocular occlusion. Since the deviation was only horizontal without a vertical disparity, involvement of certain ocular muscles responsible for elevation or depression of the eye (e.g., superior rectus, superior oblique) was ruled out. Importantly, the patient noted that the onset of her diplopia occurred during her childhood years, though she experienced double vision infrequently at that time. Given the childhood onset of the diplopia, pathological etiologies such as neurological dysfunction, space-occupying lesions and vasculopathies are less likely, moving them toward the bottom of the differential diagnosis list.
Significantly, the patient reported that the diplopia was intermittent and worsened toward the end of the day, with fatigue as a common trigger. This variability in symptoms suggests a potential decompensated phoria, myasthenia gravis or any condition that worsens with exhaustion.
There are several categories of esotropia, including infantile, accommodative, non-accommodative, mechanical, decompensated phoria and microesotropia. Since the patient’s eso-deviation is greater than 10 prism diopters, it does not qualify as micro-esotropia. Infantile esotropia typically presents around 6 months of age, with characteristics such as a large (greater than 40 prism diopters) angle, dissociated vertical deviation, amblyopia and latent or manifest nystagmus—none of which were present during testing in this patient.
The patient did not report any other symptoms associated with her diplopia, which supports a diagnosis of decompensating phoria. Her ocular history revealed myopia during her teenage years, which rules out any accommodative component to her esotropia. Additionally, her medical history was unremarkable for signs of vascular or thyroid issues.
Sensorimotor Evaluation with Ancillary Testing: Key Diagnostic Tests to Evaluate Esotropia
A comprehensive testing protocol is essential to fully assess the nature of esotropia. Extraocular movements will help determine if there is any restriction in the ocular muscles. The cover test in all nine gazes will assess the comitancy of the eye posture and its magnitude. A cranial nerve palsy would typically show a higher magnitude of deviation in the direction of the affected ocular muscle, while a decompensated phoria will generally demonstrate comitancy and no abnormal head posture.
Visuoscopy is used to evaluate eccentric fixation, which is often associated with decreased visual acuity and deep amblyopia. Bagolini testing allows clinicians to test for anomalous retinal correspondence (ARC), a brain issue in which one eye uses an extra-foveal location and the other eye uses its foveal location; it is a sensory maladaptation to avoid diplopia. The development of eccentric fixation, anomalous retinal correspondence or amblyopia suggests that the strabismus has been long-standing.
Randot stereopsis and Worth 4 Dot testing assess the patient’s sensory fusion ability and its range. Understanding the distance at which the patient can achieve fusion is crucial for therapy, as binocular activities are typically initiated at the distance where the patient can fuse the images correctly. Motor fusion testing through step vergence ranges evaluates the patient’s response to prism. Step vergences are performed over smooth vergence ranges because this testing method is conducted in free space, allowing the patient to perform in a more natural setting as opposed to being behind a phoropter, which can block peripheral vision and alter the testing environment.
Differential Diagnoses for Adult-Onset Esotropia
After completing the necessary testing protocol and obtaining a comprehensive history, the clinician can begin ruling out certain pathologic etiologies. Since the patient did not exhibit any ocular muscle restrictions, a cranial nerve palsy or mechanical dysfunction is unlikely. Additionally, the patient’s unremarkable medical history and absence of neurological symptoms help rule out a space-occupying lesion, vasculopathy-related deficits or inflammatory causes.
One differential diagnosis to consider is Sagging Eye Syndrome (SES), which involves deterioration of the band tissue of the superior rectus and lateral rectus muscles, leading to an inability to diverge when looking at distant objects.6 This condition is typically associated with specific facial features, such as a deep superior sulcus and upper eyelid ptosis, and generally has an average onset age of 70 years. However, this patient did not present with any abnormal facial features nor fit the demographic criteria for SES.
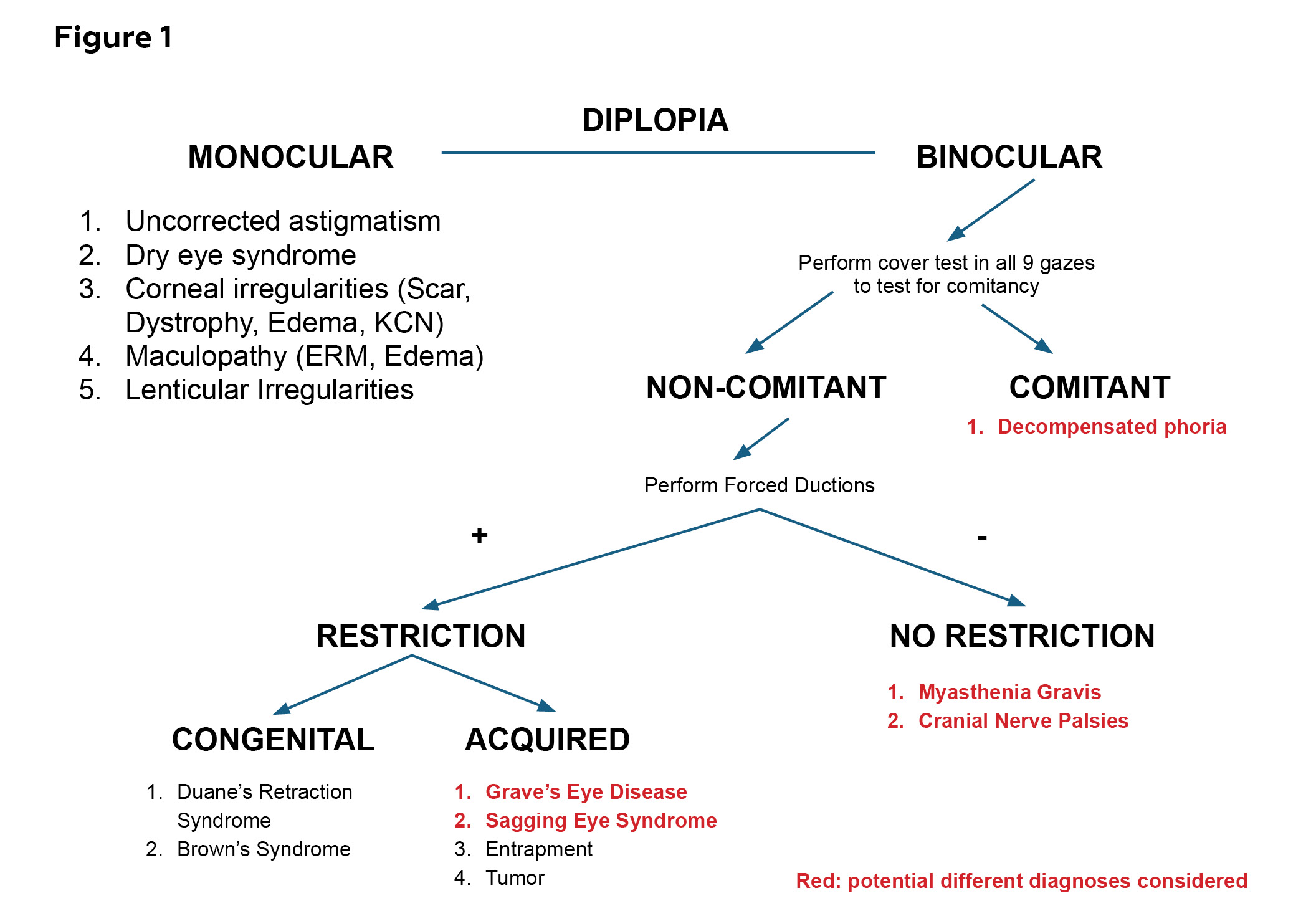
Figure 1. Algorithm for the Assessment of Diplopia in a Patient with Esotropia and Differential Diagnoses. Click to enlarge
Another potential diagnosis is myasthenia gravis, as diplopia is a common initial symptom in adult patients with ocular myasthenia gravis, particularly when it affects the lateral rectus muscle.7 Ocular myasthenia gravis is reported to affect Caucasian patients with frequent symptoms of fluctuating ptosis, diplopia and fatigability with sustained upgaze.8 While the patient is Caucasian, she did not demonstrate any fluctuating ptosis or twitching during the assessment of extraocular motilities, making myasthenia gravis less likely in this case. Figure 1 provides a summary of the differential diagnoses based on test findings.
Treatment Options
Determination of Vision Therapy vs Surgery
The decision to pursue in-office vision therapy depends on the type of strabismus and the patient’s sensorimotor fusional capabilities.14 The prognosis is generally more favorable when the strabismus is intermittent, and when the patient has first or second-degree fusion ability. In this patient’s case, although her strabismus was constant, she demonstrated second-degree fusion with Worth 4 Dot testing and showed local stereopsis on Random Dot testing. These findings indicated that vision therapy was a viable option despite the absence of global stereopsis initially.
In contrast, a surgical consultation is recommended for patients with a cosmetically significant strabismus, particularly if the esotropia deviation exceeds 15 prism diopters at both distance and near, even when the patient is fully corrected with glasses.14 Since the patient’s deviation was 12 prism diopters, surgery was not recommended at that time. Specifically, patients with constant diplopia that exceeds 15 prism diopters may warrant a surgical consultation due to the magnitude of the strabismus.
Determination of Prism Correction
Prism glasses were recommended due to the patient’s intermittent horizontal diplopia, which occurred while driving and significantly impacted her functionality and daily life. If the diplopia had been rare and only occurred due to fatigue at the end of her day, prism glasses would not have been recommended, as it would not have affected her daily routine.
The prescribed prism amount is based on the patient’s subjective responses and fusional ability. The goal is to resolve the patient’s diplopia while enhancing binocularity at all distances, using the lowest amount of prism that satisfies both criteria. However, there is a potential for prism adaptation—a phenomenon in which the patient’s eye alignment shifts in response to the prism. In such cases, the initial adaptation can result in a recurrence of the original strabismic deviation, effectively negating the corrective effect of the prism. Consider performing a prism adaptation test if the patient has suppression to assess for the presence of prism adaptation. For these patients, prism would not be beneficial. The patient had already been using prism glasses provided by her primary optometrist, which resolved her diplopia and improved her binocular fusion ability from 40 cm to around 4 ft, indicating progress.
To determine the optimal prism prescription, the patient focused on a single letter in the distance while the examiner used a prism bar and gradually increased the compensatory prism until the patient reported fusion. If suppression is suspected, a similar method could be used but with a Worth 4 Dot target while the patient wears red/green glasses as the compensatory prism is used. Ideally, the required prism amount is confirmed across different tests before prescribing it. After determining the appropriate prism, the patient’s random dot stereopsis should be re-tested. Since there was no improvement in either local or global stereopsis for this patient, the prism glasses were recommended only when diplopia occurred while driving, rather than full-time.
Determination of the Prognosis for Treatment Success
Given that the strabismus likely stemmed from a decompensated phoria, in-office vision therapy was recommended as the primary treatment. The patient’s ultimate goal was to avoid wearing glasses throughout the day and to regain depth perception. The patient understood that the length of the therapy program would depend on weekly progress, but it was estimated to take approximately 24 weeks, consisting of 2 units of therapy with both in-office and home-based exercises.
Since the patient did not exhibit eccentric fixation or anomalous retinal correspondence, the prognosis for improvement was optimistic. At the beginning of vision therapy, the recommendation was for the patient to continue wearing her contact lenses for full correction and to use the prism glasses only as needed while driving.
Vision therapy sessions were scheduled for 1 hour per week, with homework assignments provided to be completed at home for at least 15 minutes each day. After 12 office sessions, progress was evaluated by repeating previously abnormal tests for comparison. Case reports have demonstrated that adult patients undergoing vision therapy can develop an appreciation for global stereopsis.9 These patients were highly motivated and compliant with in-office therapy supported by home exercises.
Although there are limited studies showing the efficacy of in-office vision therapy for long-standing strabismus, due to the belief that neuroplasticity only has a significant effect during the critical period, there is growing evidence suggesting that binocularity improvement is possible even outside the critical period.9 Additionally, the adult visual system has been shown to retain residual plasticity beyond this critical period through sight restoration therapies.10,11 The patient in this case was highly motivated to begin vision therapy and expressed a strong desire to regain control over her eyes to alleviate the binocular diplopia she experienced, especially toward the end of the day.
The Role of Binasal Occlusion
Binasal occlusion (BNO), a passive vision therapy technique, involves placing opaque tape or similar material on the inner third of eyeglass lenses to reduce visual stress and improve binocular vision, particularly for conditions like esotropia or following mild traumatic brain injury (mTBI). While the patient was never officially diagnosed with a traumatic brain injury, she experienced a severe car accident during childhood in which she fell out of the back of a car window. Although the details of the incident are vague, it is likely that the event resulted in a mild traumatic brain injury. Studies have shown that patients with a history of TBI may have a decreased ability to process and organize spatial information, which in turn reduces the focal system’s processing capability. Binasal occlusion aims to reduce visual stress and improve binocular vision by blocking parts of the image seen by both eyes. This taping method provides an opportunity for the brain to process visual information in a different way, thereby improving eye coordination and reducing visual motion sensitivity.¹² Appendix D provides instructions for the application of binasal occlusion.
Individualized Vision Therapy Programming: Treatment Duration, Therapy Sequencing and the Role of Home Therapy
The approach to programming this particular therapy protocol was designed to be as efficient as the patient would allow. In other words, the patient’s improvement in visual skills each week determined the pace of the therapy program. Since the patient was an adult with remarkable motivation, the pace of therapy was enhanced and centered around the patient’s visual goals. Additionally, activities performed in the office were provided as home exercises, requiring at least 15 minutes per day of practice. The patient practiced exercises every day for at least 20 minutes. Home vision therapy is a crucial component of the patient’s progress and success in the program. Performing the activities daily at home provided the necessary repetition of the preferred sensorimotor pathways with specific, directed attention. The more consistent the repetition, the more likely the correct habit would be formed and utilized subconsciously, without additional mental effort.
Initially, monocular visual efficiency skills, including accommodation, saccades and pursuits, were emphasized. However, by Week 4, the patient demonstrated equal visual skills between both eyes and was able to begin peripheral fusion activities and anti-suppression techniques. After the first progress evaluation, the patient experienced global stereopsis for the first time, meaning that she was finally bi-foveal and using both eyes simultaneously. The anti-suppression phase was particularly lengthy but necessary for the patient to advance to binocular skill-building. As the anti-suppression phase showed limited progression each week, the therapy schedule was adjusted to bi-weekly visits instead of weekly. The patient needed additional time to practice anti-suppression activities at home before returning for another in-office session.
Understanding the patient’s motivation and the likelihood of compliance with home therapy can help the clinician design a therapy protocol that allows for efficiency and progress at a comfortable pace. An individualized therapy program enhances efficacy and productivity in reaching the patient’s visual objectives. A patient is essentially ready to graduate from vision therapy when all visual goals have been met and the patient is satisfied with their progress. While there is always potential for further improvement in the visual system, understanding and acknowledging the patient’s visual goals and initial purpose for vision therapy will guide the clinician in determining the appropriate time to conclude the therapy program.
Conclusion
When evaluating or diagnosing a patient with strabismus, clinicians and students must understand the significance of the patient’s medical and ocular history, as well as the nature of the diplopia onset. A thorough sensorimotor evaluation, supplemented by pertinent ancillary testing, can help determine the cause of the strabismus presentation and provide essential information for constructing an effective treatment and management plan.
Appendices
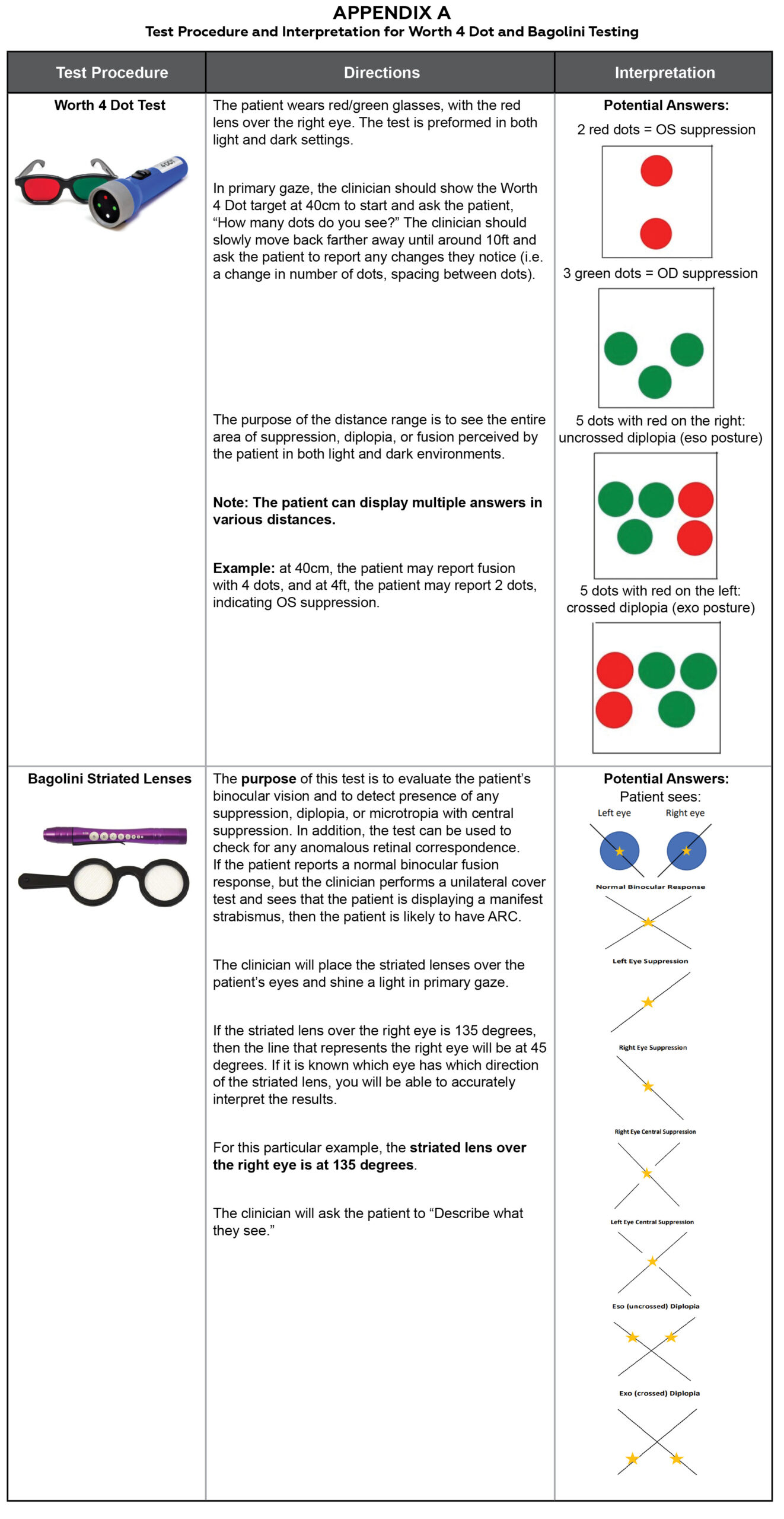
Appendix A. Test Procedure and Interpretation for Worth 4 Dot and Bagolini Testing. Click to enlarge
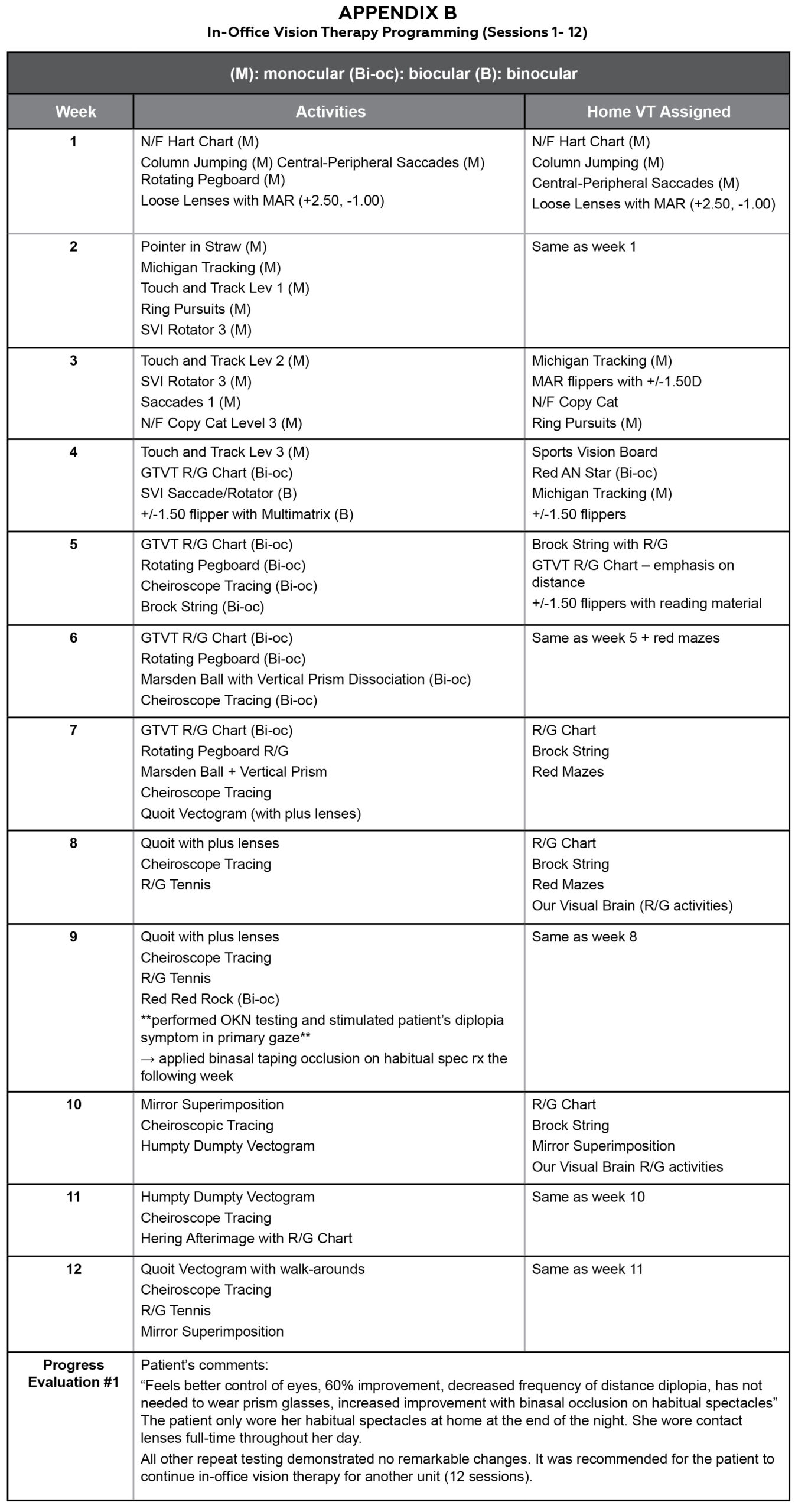
Appendix B. In-Office Vision Therapy Programming (Sessions 1-12). Click to enlarge
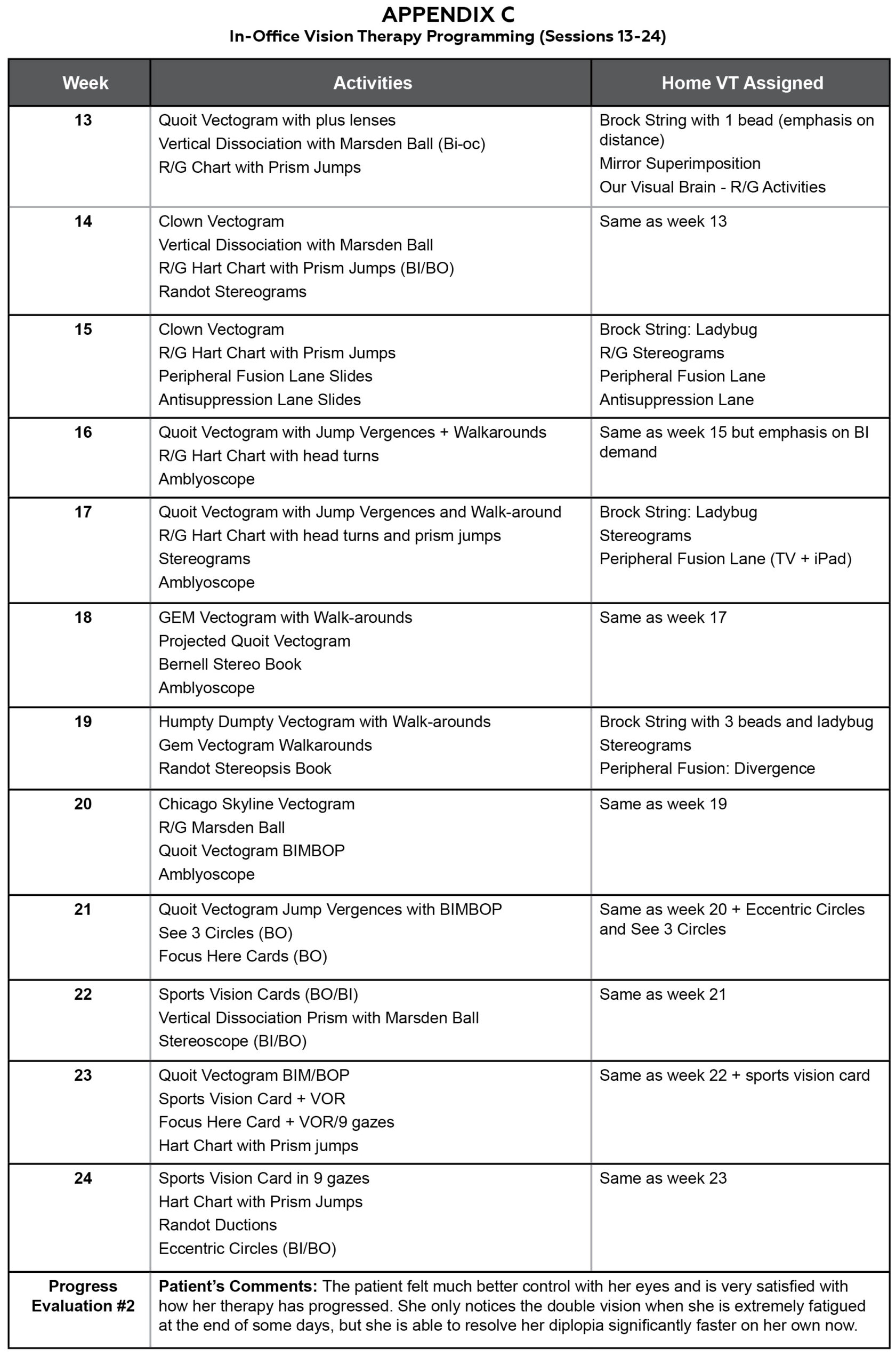
Appendix C. In-Office Vision Therapy Programming (Sessions 13-24). Click to enlarge
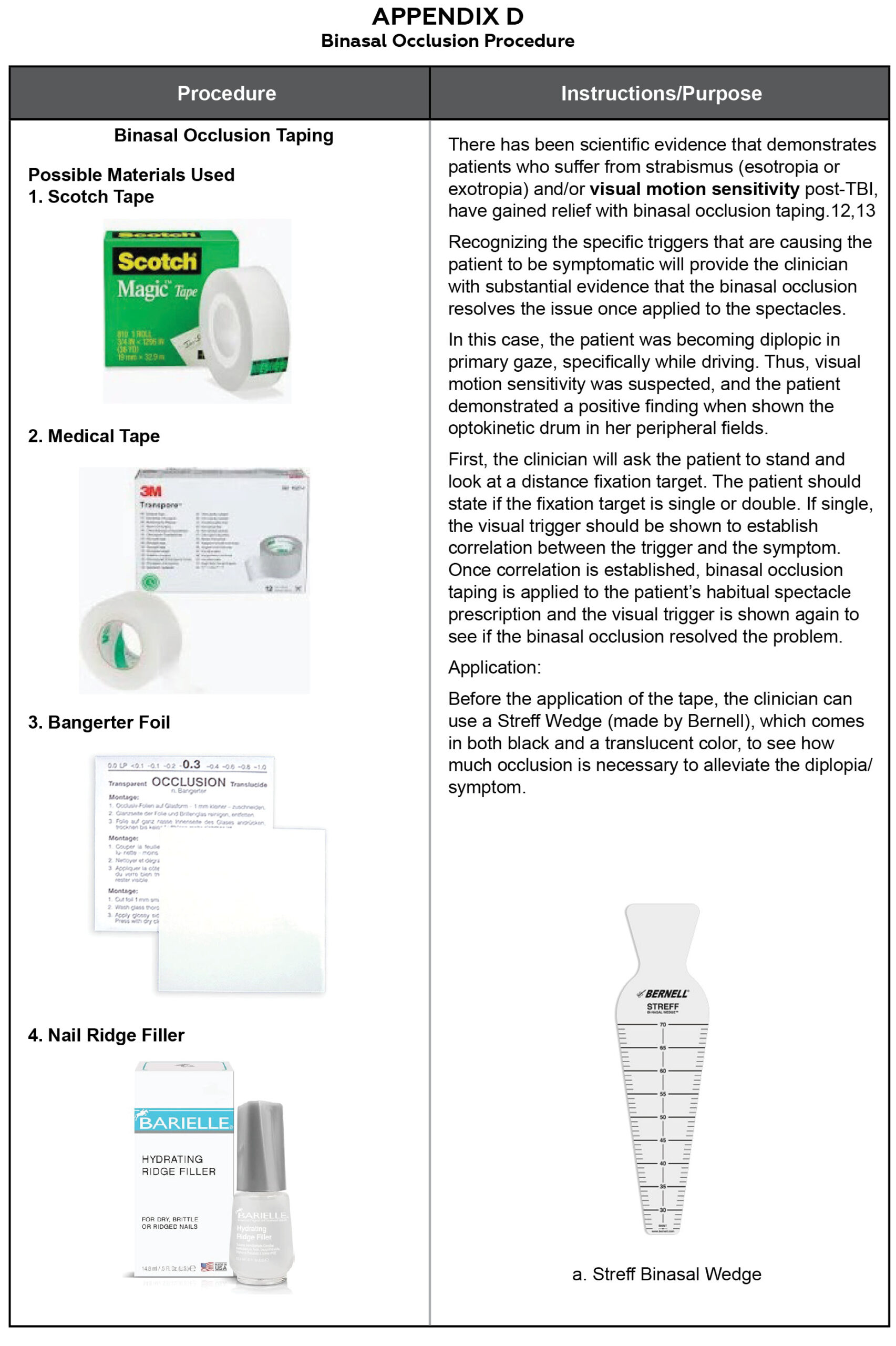
Appendix D. Binasal Occlusion Procedure. Click to enlarge
References
- Suhr CL. Top causes of double vision [Internet]. Review of Optometry; 2019 Aug 15 [cited 2025 Oct 4]. Available from: https://www.reviewofoptometry.com/article/top-causes-of-double-vision
- Kumar N, Kaur S, Raj S, Lal V, Sukhia J. Causes and outcomes of patients presenting with diplopia: a hospital-based study. Neuroophthalmology. 2021 Mar 2;45(5):238-45. DOI: 10.1080/01658107.2020.1860091
- Abducens nerve palsy [Internet]. Treasure Island (FL): StatPearls Publishing LLC; c2023 [cited 2025 Oct 4]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482177/
- Urist MJ. Eccentric fixation in amblyopia ex anopsia. AMA Arch Ophthalmol. 1955 Sep;54(3):345-50. DOI: 10.1001/archopht.1955.00930020351003
- Wong AM, Lueder GT, Burkhalter A, Tychsen L. Anomalous retinal correspondence: neuroanatomic mechanism in strabismic monkeys and clinical findings in strabismic children. J AAPOS. 2000 Jun;4(3):168-74.
- Denny P. Diplopia at distance in older patients: is it sagging eye syndrome? EyeNet Magazine [Internet]. American Academy of Ophthalmology; 2022 Mar 1 [cited 2025 Oct 4]. Available from: https://www.aao.org/eyenet/article/diplopia-at-distance-in-older-patients
- Ophthalmologic manifestations of myasthenia gravis [Internet]. New York (NY): WebMD LLC; c2023 [cited 2025 Oct 4]. Available from: https://emedicine.medscape.com/article/1216417
- Behbehani R. Ocular myasthenia gravis: a current overview. Eye Brain. 2023 Feb 5;15:1-13. DOI: 10.2147/EB.S389629
- Han S, Baker J, Jenewein E. Case series: neuroplasticity and vision therapy in adults with unilateral small-angle esotropia. Clin Insights Eyecare. 2024;2(2). Available from: https://clinicalinsightsineyecare.scholasticahq.com/article/94928
- Castaldi E, Lunghi C, Morrone MC. Neuroplasticity in adult human visual cortex. Neurosci Biobehav Rev. 2020 May;112:542-52. DOI: 10.1016/j.neubiorev.2020.02.028
- Thompson B, Concetta MM, Bex P, Lozama A, Sabel BA. Harnessing brain plasticity to improve binocular vision in amblyopia: an evidence-based update. Eur J Ophthalmol. 2024 Jul;34(4):901-12. DOI: 10.1177/11206721231187426
- Proctor A. Traumatic brain injury and binasal occlusion. Optom Vis Dev. 2009;40(1):45-50.
- Barton JJS, Ranalli PJ. Vision therapy: occlusion, prisms, filters, and vestibular exercises for mild traumatic brain injury. Surv Ophthalmol. 2021 Mar-Apr;66(2):346-53. DOI: 10.1016/j.survophthal.2020.08.001
- Care of the patient with strabismus: esotropia and exotropia. Optometric clinical practice guideline [Internet]. St Louis (MO): American Optometric Association; c2010 [cited 2025 Oct 4]. Available from: https://www.aoa.org/AOA/Documents/Practice%20Management/Clinical%20Guidelines/Consensus-based%20guidelines/Care%20of%20Patient%20with%20Strabismus%20Esotropia%20and%20Exotropia.pdf
- Adult strabismus preferred practice pattern [Internet]. San Francisco (CA): American Academy of Ophthalmology; c2023 [cited 2025 Oct 4]. Available from: https://www.aaojournal.org/article/S0161-6420(24)00013-7/pdf

