
PEER REVIEWED
Scleral Lens for Vision Correction Following Pseudomonas Aeruginosa Keratitis Associated with Prior Contact Lens Over Wear
Thuy-Lan Nguyen, OD, FAAO, FSLS, Stacy Zubkousky, OD, FAAO, FSLS
Abstract
Contact lens wear is healthier than ever due to daily disposable and high oxygen permeable, silicone hydrogel lenses. Unfortunately, microbial keratitis (MK) is still a potentially sight threatening complication of contact lens over wear. Pseudomonas aeruginosa is the most frequently isolated microorganism associated with MK in contact lens wearers. Central corneal scars following a P. aeruginosa keratitis can cause significantly decreased vision. This case will discuss the benefits of scleral lenses in a young, active, myopic female with a large, visually significant corneal scar following a contact lens-related ulcer (CLRU) due to P. aeruginosa.
Keywords
Background
Microbial keratitis (MK) is an infectious corneal condition which can lead to corneal scarring and potentially serious visual impairment.1 Overnight contact lens wear is a leading cause for MK, especially in younger patients. In 1989, Poggio et al introduced the first large scale study of contact lens ulcers which revealed that ulcerative keratitis was five times more likely among extended wear soft contact lens users compared to daily wear soft contact lens users (20.9/10,000 patients and 4.1/10,000 patients, respectively.)2 Pseudomonas aeruginosa is an aerobic gram-negative, rod-shaped bacterium, which accounts for approximately 63% of contact lens-related ulcers (CLRUs), making it the most common cause.3,4 The hallmark of P. aeruginosa keratitis is a ring abscess, a ring-shaped accumulation of polymorphonuclear leukocytes surrounding a central corneal lesion.5 P. aeruginosa keratitis can ultimately lead to suppurative infiltration, corneal perforation, corneal melt or endophthalmitis.5 Even when properly treated, a central corneal ulcer can leave patients with visually significant corneal scarring.
Patients with a previous history of MK may want to return to contact lens wear once their infection has resolved. However, soft contact lenses may not provide functional vision if the MK has resulted in central corneal scarring. Scleral gas permeable contact lenses can be used as a visual correction of refractive errors in normal eyes as well as patients with irregular corneas such as keratoconus, pellucid marginal degeneration, post-LASIK ectasia, corneal scarring and ocular surface diseases. Benefits of scleral lenses include improved comfort and stable vision compared to corneal gas permeable and other contact lenses.6
Case Description
History
A 19-year-old African American female was referred for a “hard” contact lens fit. She was previously diagnosed and treated for a corneal infection of the right eye secondary to “Pseudomonas” that left permanent scarring in the center of the visual axis. The patient had a prior history of wearing unknown soft contact lenses overnight. Her previous contact lenses were ordered from an online vendor. The patient’s medical history is otherwise unremarkable. She reported taking no medications and she had no known drug allergies. The patient was a college student and enjoyed track and field as well as basketball.
Previous records revealed that a year before her examination, she presented with irritation and light sensitivity in the right eye for 4 days that was first thought to be iritis by her previous eyecare provider. However, her symptoms were worsening even with the prescribed eye drops. She was diagnosed with a corneal ulcer in her right eye, severe inflammatory reaction with a 1 mm hypopyon and a 7×8 mm region of corneal edema, likely bacterial in nature. Cultures were ordered and treatment was initiated with fortified vancomycin, tobramycin, ciprofloxacin every hour in the right eye, topical Cyclogyl 3 times a day and oral minocycline and vitamin C.
Records showed at the 1-day follow-up, the hypopyon had resolved and the epithelial defect was slightly smaller. The area of edema and infiltrate was stable, so all medications were continued.
Records showed at the 4-day follow-up, final cultures and sensitivities were received. Gram stain showed no white blood cells seen, with many Gram-negative rods. Culture showed “many pseudomonas aeruginosa”. Sensitivities were positive for amikacin, aztreonam, cefepime, ciprofloxacin, gentamicin, imipenem, levofloxacin, meropenem, piperacillin, piperacillin /tazobactam and tobramycin. Evaluation revealed no hypopyon and decreased density of infiltrate with symptomatic improvement. Vancomycin was discontinued. Fortified tobramycin and ciprofloxacin were tapered to every 2 hours. Cyclogyl was continued. Oral minocycline and ciprofloxacin were continued for the 10-day course.
Records show at the 7-day follow-up, there was continued symptomatic improvement, no hypopyon and decreased density of infiltrate. Topical Cyclogyl was discontinued. Topical Pred Forte was added every 4 hours. Topical fortified tobramycin and ciprofloxacin were tapered to every 4 hours.
Records show at the 8-day follow-up, the patient was diagnosed as a resolved pseudomonas keratitis with a large central scar. The patient was advised to continue topical ciprofloxacin 4 times daily for 3 days, then discontinue. Pred Forte was continued 4 times daily for 1 week then tapered over 3 weeks. At the 1-year evaluation, patient was diagnosed with resolved pseudomonas keratitis in the right eye with large central scar. Patient was highly interested in surgery for cosmetics; however, she was advised against penetrating keratoplasty surgery due to the thinned cornea, her young age and the extent of the surgery. Following that ophthalmology visit, she presented to Nova Southeastern University for a specialty contact lens examination.
Examination findings
Unaided acuities were Count Fingers at 6 feet for the right eye and 20/400 in the left eye. Corrected acuities with her current glasses were 20/80 for the right eye and 20/20 for the left. Manifest refraction in the right eye was: -5.00 sphere and left eye: -5.00 sphere with best-corrected visual acuities of 20/80 (right) and 20/20 (left). Pinhole offered no improvement in the right eye. The right pupil was partially obstructed by a white central corneal scar. The left pupil was round and reactive. There was no afferent pupillary defect using reverse method. Confrontation visual fields and extraocular motilities were full in each eye. Slit lamp examination revealed clear lids and lashes in both eyes. Bulbar conjunctiva were white and quiet in both eyes as well. The right cornea had a 4-5 mm central, opaque white scar (Figure 1). The left cornea was clear (Figure 2). Corneal topography revealed an irregular anterior corneal surface (Figure 3). Corneal topography in the left eye revealed no irregularities (Figure 4).
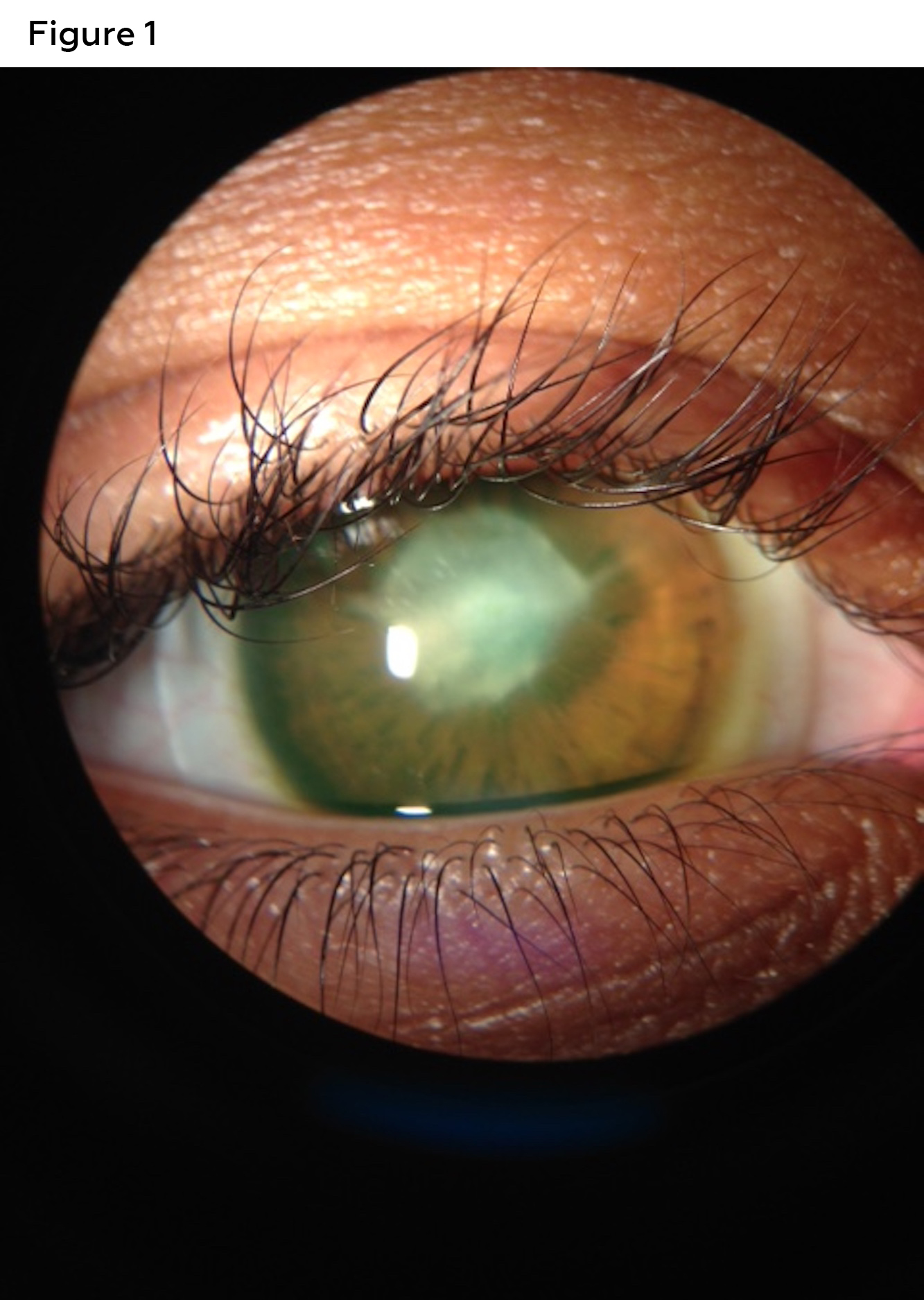 Figure 1. Corneal evaluation revealed a 4-5 mm central, opaque white corneal scar in the right eye. Click to enlarge |
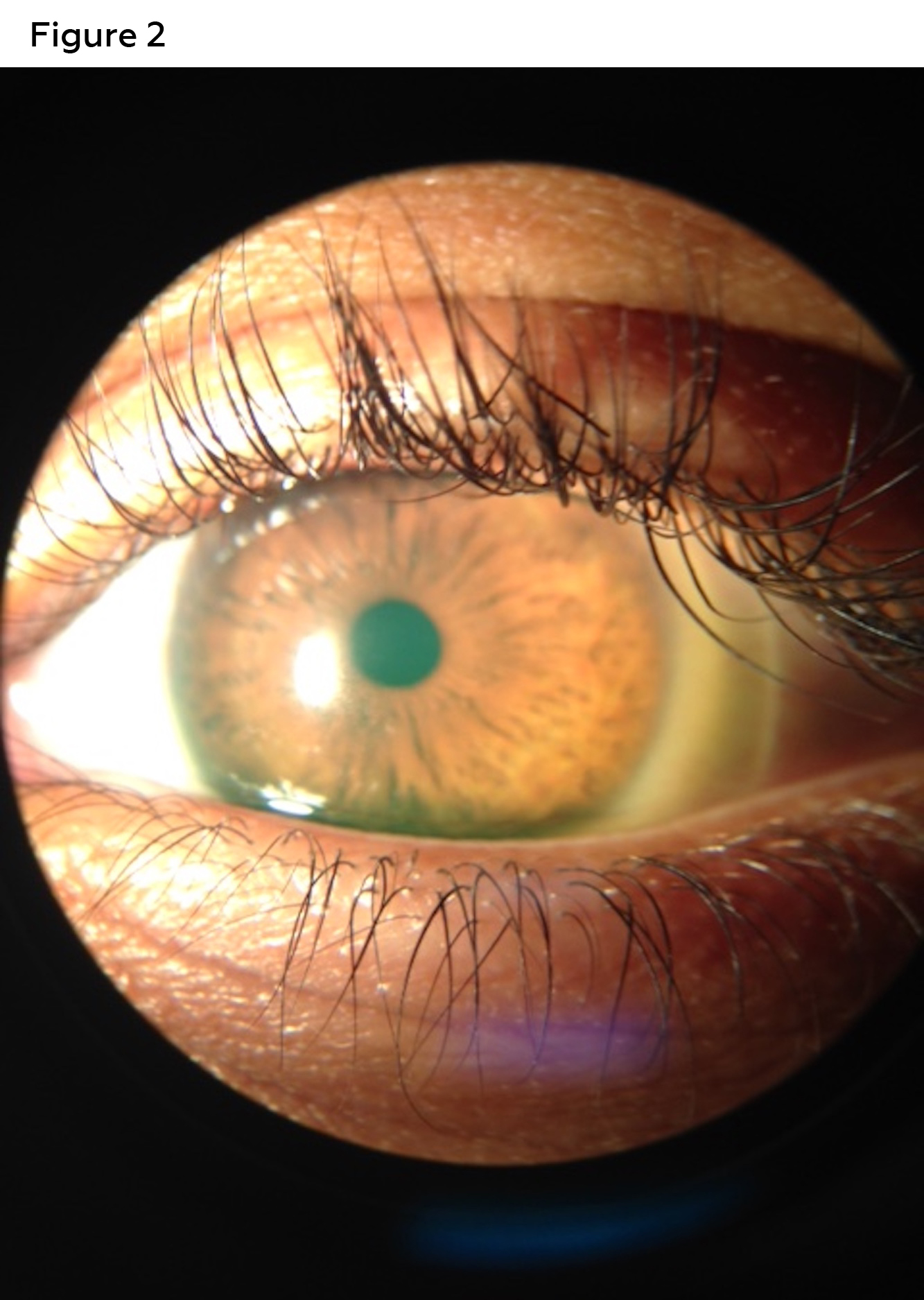 Figure 2. Cornea was clear in the left eye. Click to enlarge |
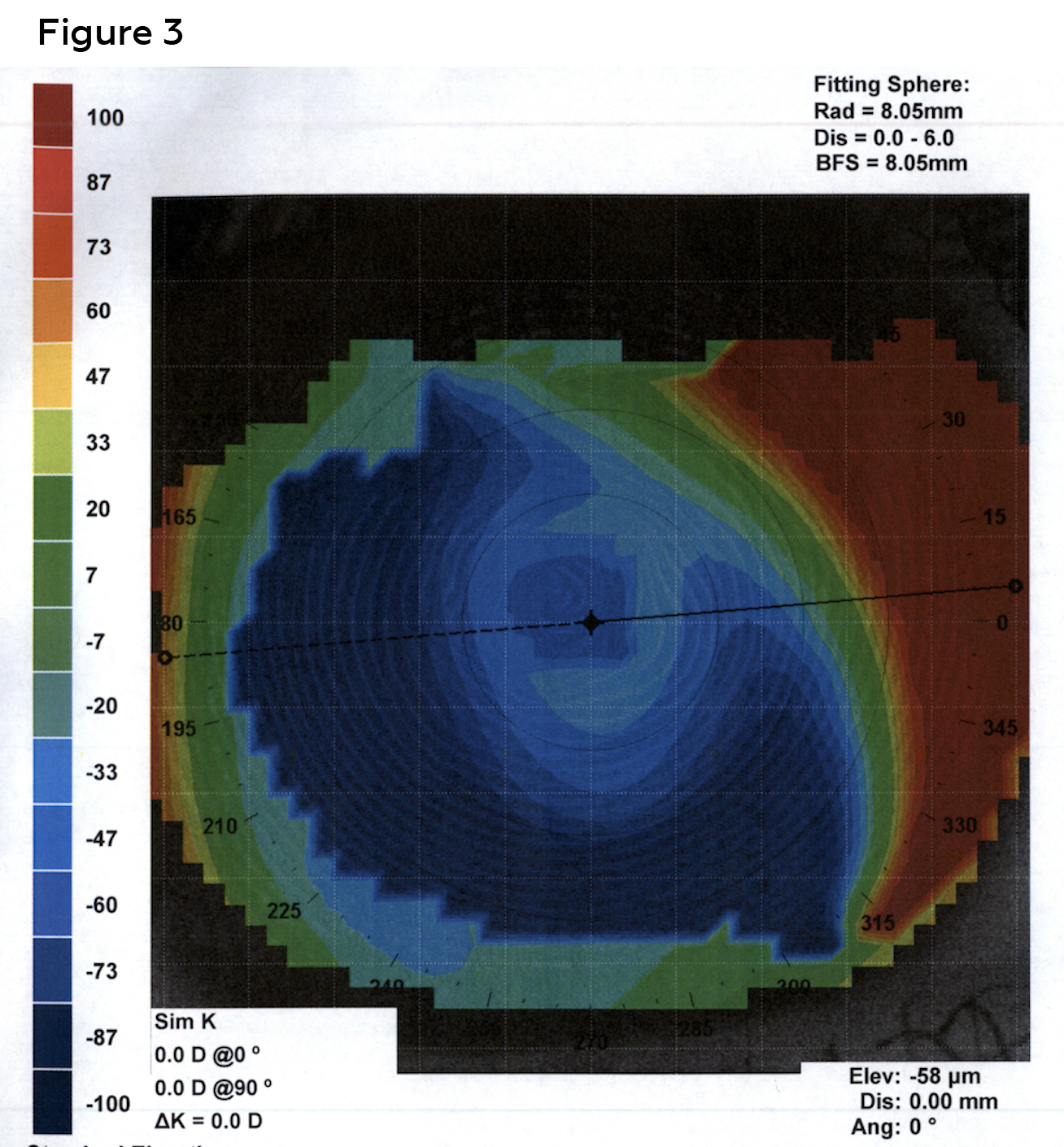 Figure 3. Corneal topography revealed an irregular anterior corneal surface caused by the central corneal scar in the right eye. Reliable keratometry readings could not be measured due to distorted mires. Click to enlarge |
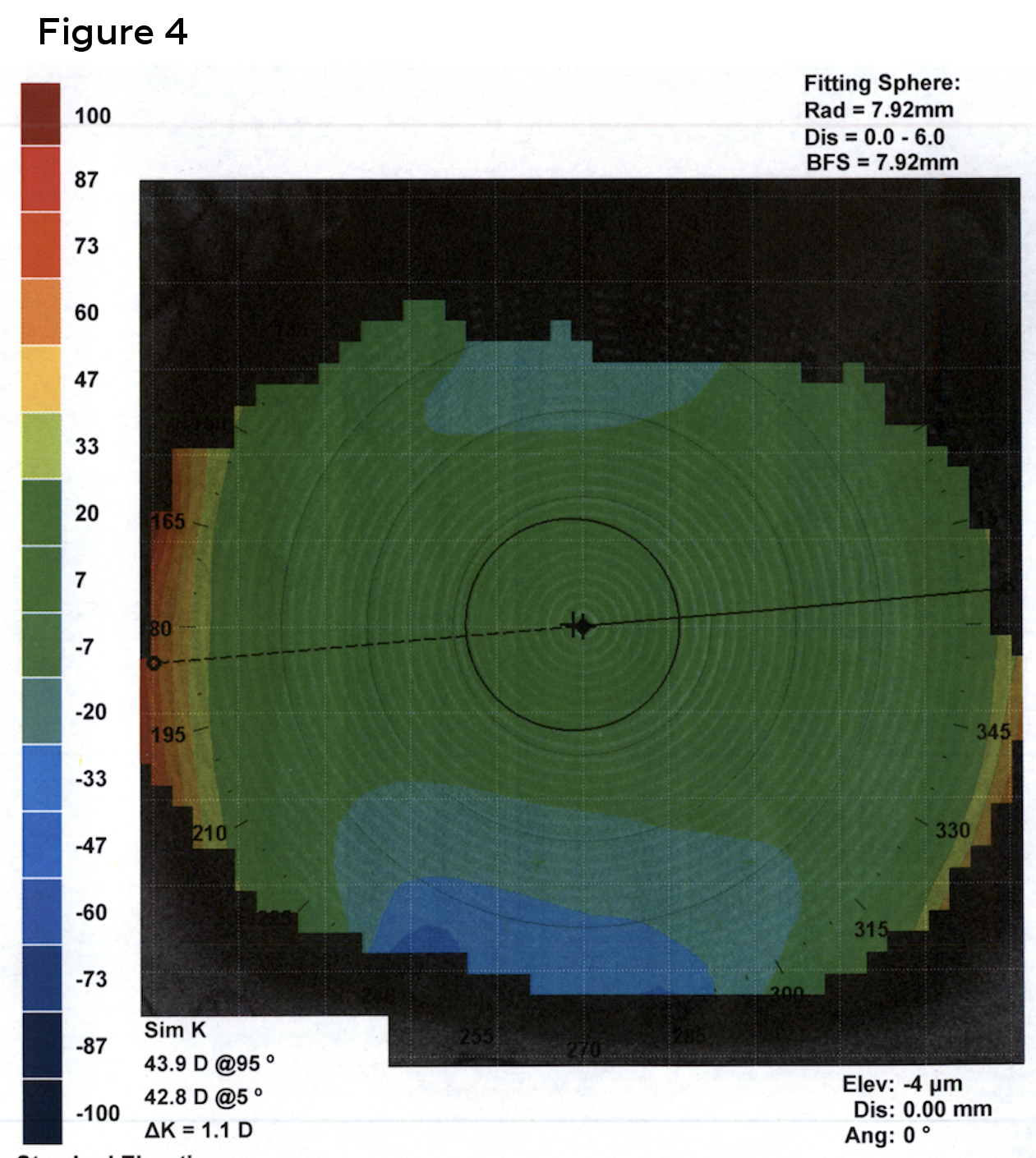 Figure 4. In contrast to the right eye, corneal topography of the left eye revealed no irregularities. Keratometry readings left eye were 43.9/42.8@005. Click to enlarge |
The patient was diagnosed with decreased vision in the right eye due to central corneal opacity associated with history of infectious corneal ulcer from P. aeruginosa and prior contact lens over wear as well as myopia in both eyes. The patient was extensively counseled on the increased risk of complication associated with contact lens over wear. Based on the patient’s motivation and successful diagnostic evaluation, contact lenses were ordered.
Art Optical Ampleye Scleral lens in Optimum Extra Material with plasma:
- Right Eye: -5.50 Power / 4200 Sag / 8.04 BC / 16.5 OAD / 150 micron toric haptic / clear
- Left Eye: -5.50 Power / 4000 Sag / 8.44 BC / 16.5 OAD / 150 micron toric haptic / clear
Follow-up #1
The patient presented for contact lens dispensing as well as insertion and removal training for new scleral lenses. She reported no changes in ocular or medical history since the last examination. Entering acuities with her current glasses were 20/80 in right eye and 20/20 in the left. Pinhole offered no improvement in the right eye. Pupils, extraocular motilities and confrontation visual fields was unchanged. Slit lamp examination revealed stable findings in both eyes with a large central corneal scar in the right eye and clear cornea in the left. Both corneas were free of sodium fluorescein staining.
Best corrected visual acuities with scleral lenses were 20/30 (right) and 20/20 (left). Lens evaluation revealed well centered, complete corneal vaulting with no limbal conjunctival compression and no conjunctival vessel impingement in both right eye (Figures 5 and 7) and left eye (Figures 6 and 8). Patient was trained on proper insertion and removal techniques as well as proper handling and disinfection systems. The patient successfully performed insertion and removal of the contact lenses in office. The patient was instructed on overnight cleaning and disinfection of lenses using a hydrogen peroxide-based solution. The lenses were dispensed, and the patient was advised to return to clinic for a 1-week follow up.
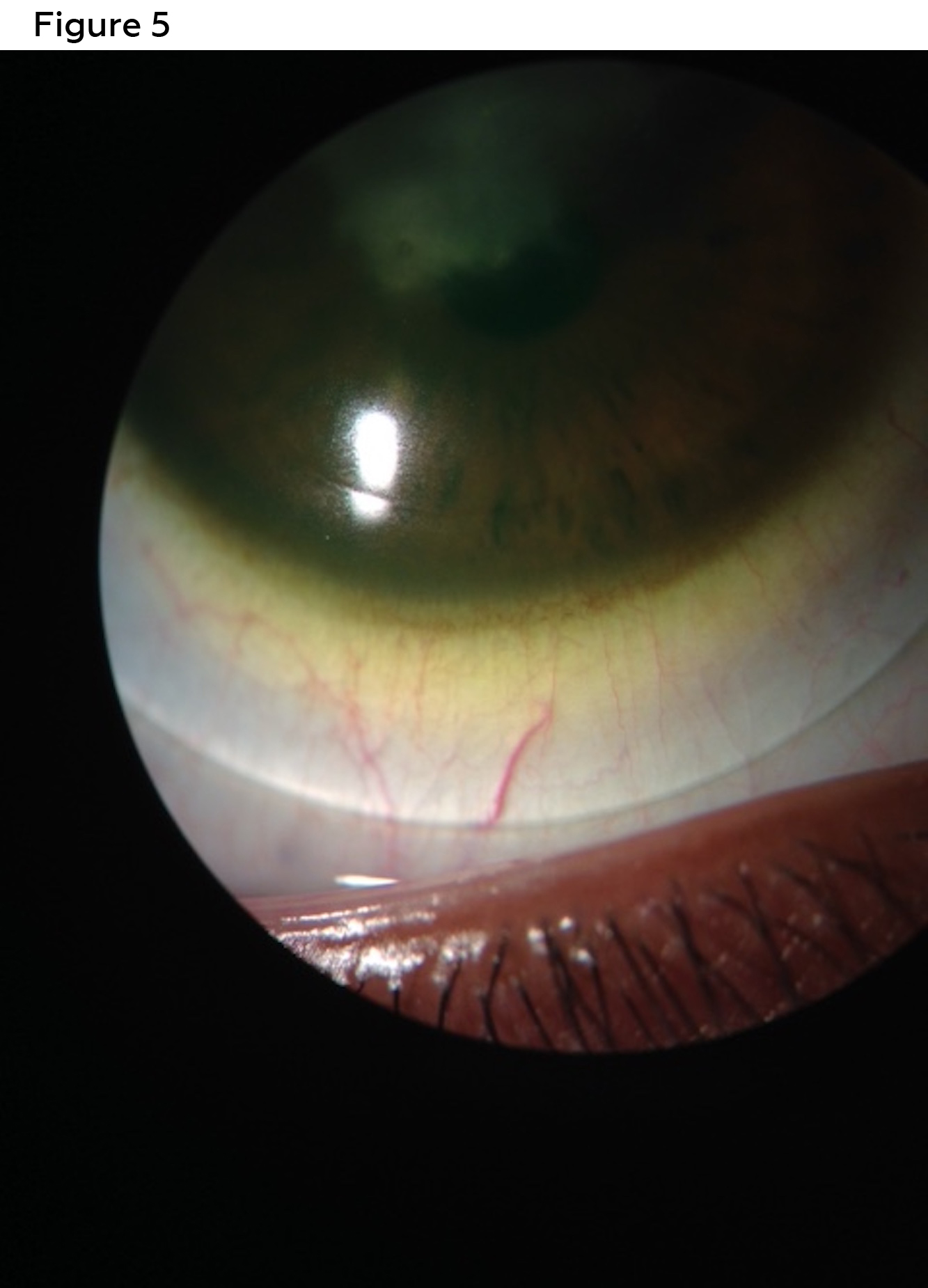 Figure 5. Diagnostic contact lens evaluation with a scleral lens was performed with a trial lens reveals no conjunctival compression and no conjunctival vessel impingement in the inferior quadrant. Over-refraction of -2.50 sphere in the right eye resulted in best corrected visual acuity of 20/300. Click to enlarge |
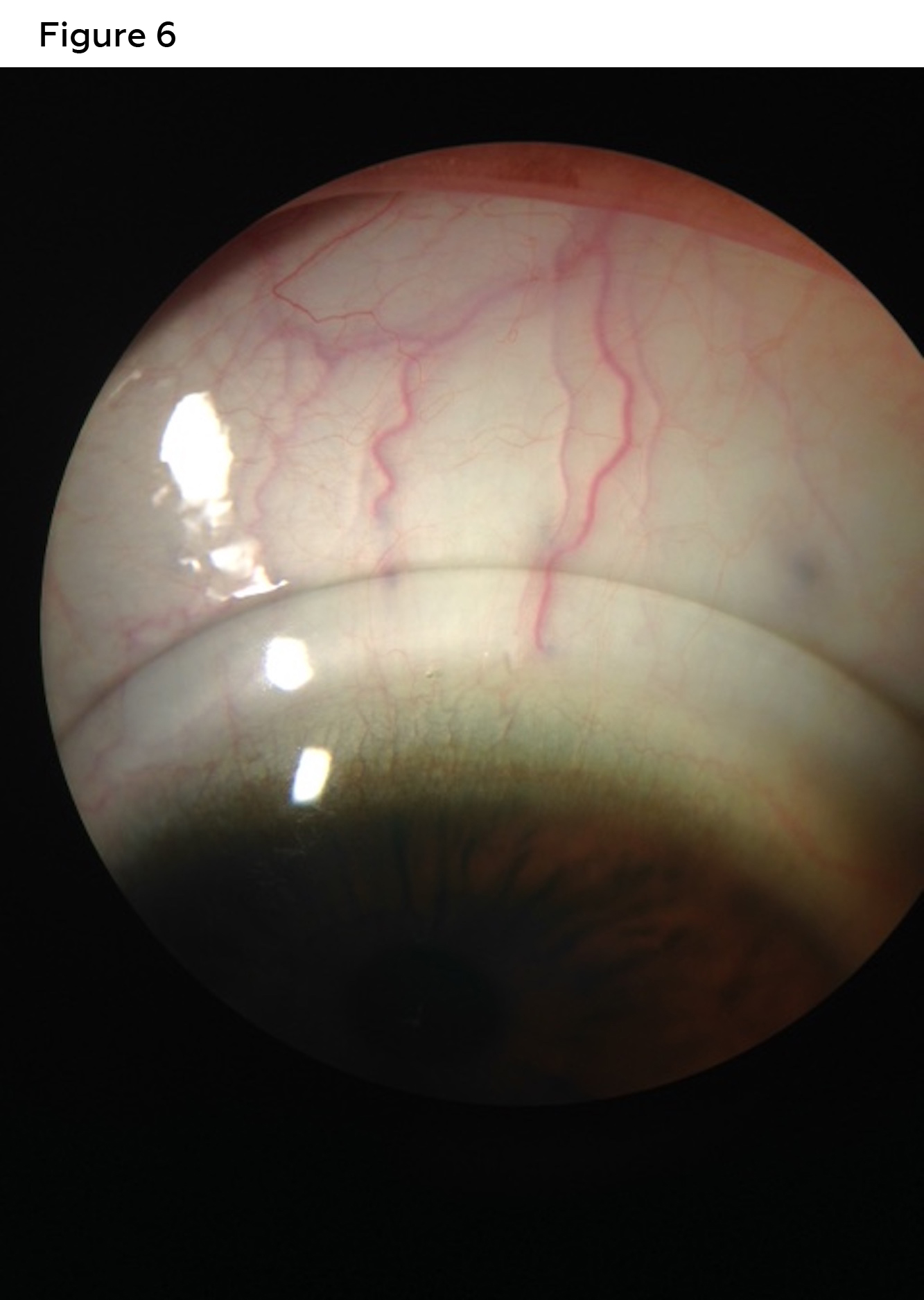 Figure 6. Diagnostic contact lens evaluation with a scleral lens was performed with a trial lens reveals no conjunctival compression and no conjunctival vessel impingement in the superior quadrant. Over-refraction of -2.50 sphere in the left eye resulted in best corrected of visual acuities of 20/20. Click to enlarge |
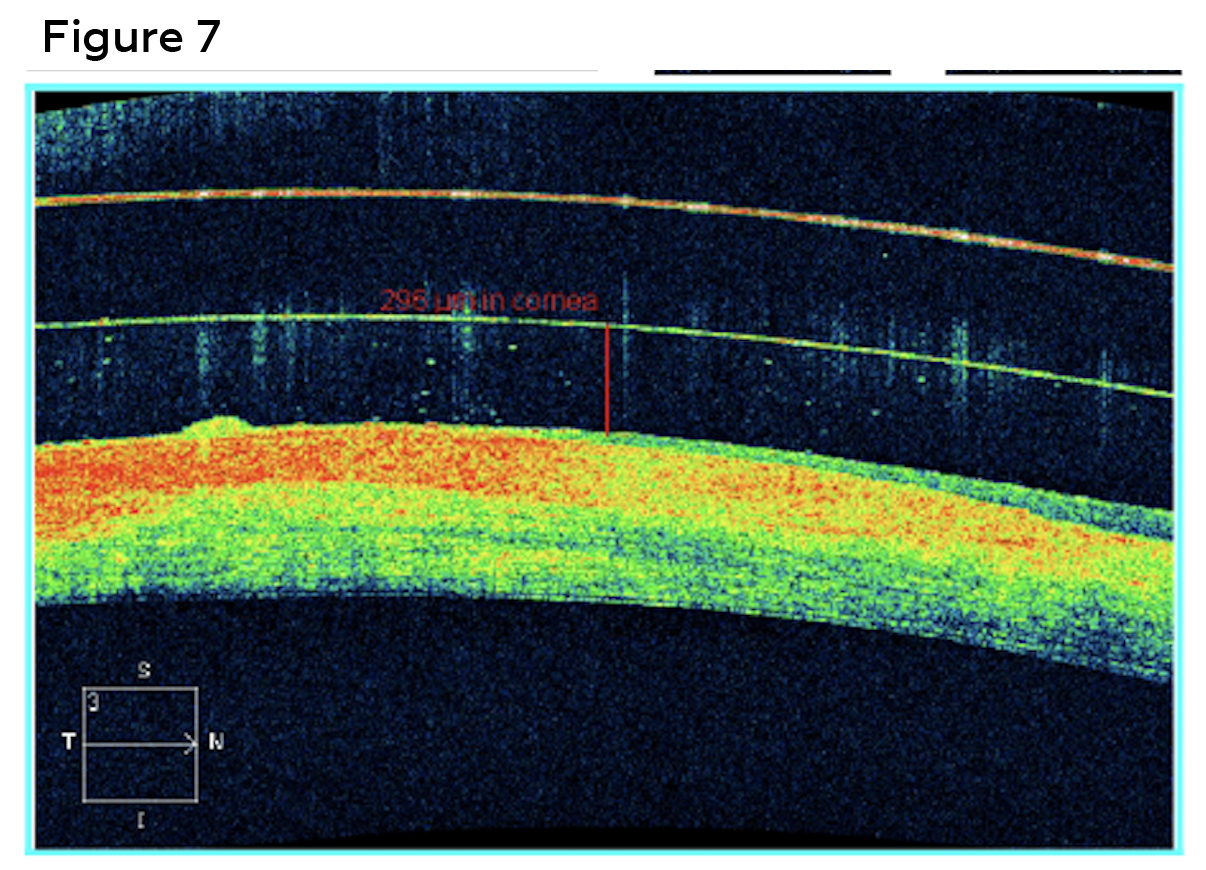 Figure 7. Anterior segment optical coherence tomography measured the diagnostic scleral contact lens with 296 microns of central clearance after approximately 20 minutes of settling in the right eye. Central scarring of the cornea caused thinning and compression of stromal tissue. Click to enlarge |
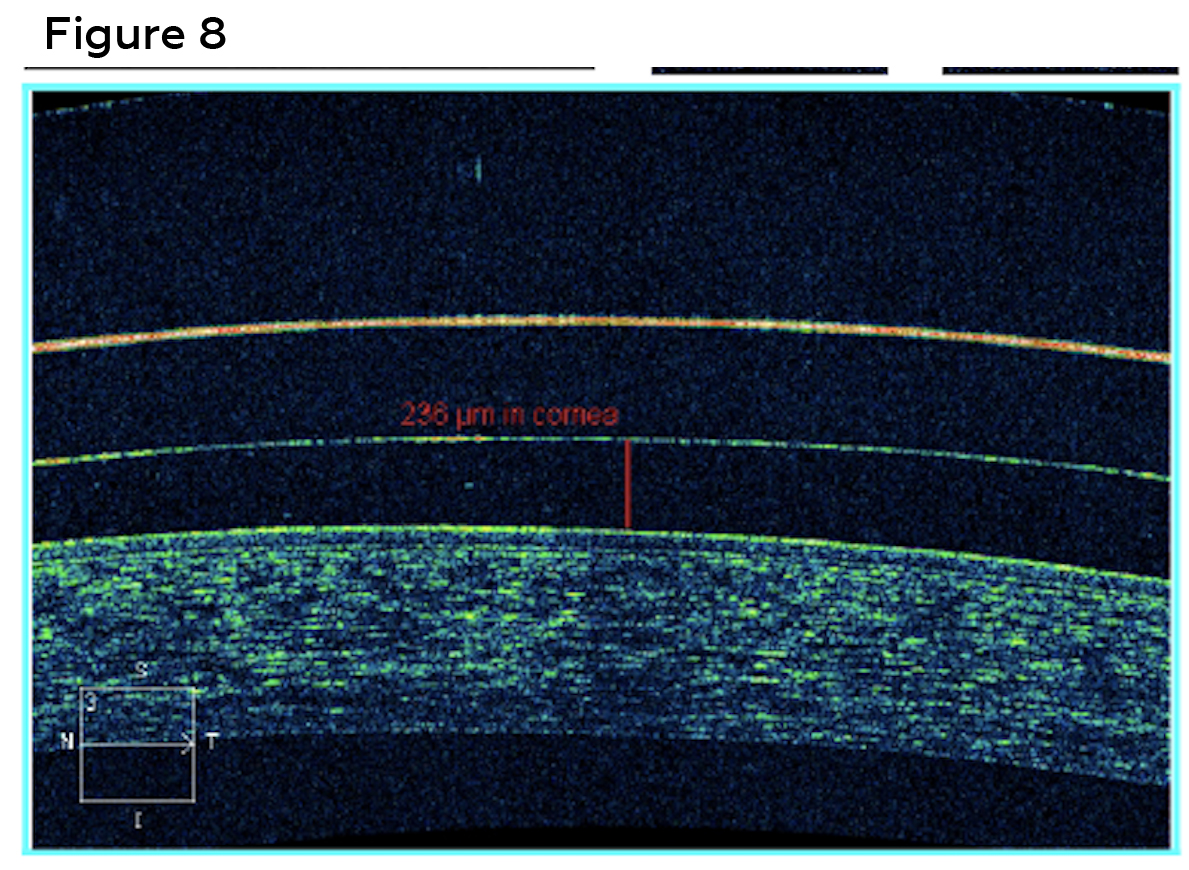 Figure 8. Anterior segment optical coherence tomography measured the diagnostic scleral contact lens with 236 microns of central clearance after approximately 20 minutes of settling in the left eye. Click to enlarge |
Follow-up #2
The patient presented for a 1-week contact lens follow-up. Patient reported good comfort and vision with lenses dispensed at the last visit. She reported proper use of contact lens care product since the last visit. She reported no other changes in ocular or medical history and denied any symptoms of ocular redness, pain or discharge. Visual acuities with contact lenses were stable at 20/30 (right) and 20/20 (left). Contact lens evaluation revealed well-fitting lenses. Slit lamp examination revealed a stable, central corneal scar in the right eye and was unremarkable in the left. No changes were made to the contact lenses. The patient was again advised on the increased risk of complication associated with contact lens over wear as well as proper wearing and handling techniques.
Follow-up #3
The patient presented for a 6-month contact lens follow-up. She reported good comfort, vision and compliance to wearing and handling schedule. She reported no changes in ocular or medical history since the last examination. She was applying to the Navy and requested a letter of support. Best-corrected visual acuities with scleral lenses remained stable at 20/30 (right) and 20/20 (left). Contact lens evaluation revealed well-fitting lenses for both eyes. Slit lamp examination revealed a stable central corneal scar in the right eye and was unremarkable for the left. The patient was again advised on the increased risk of complication associated with contact lens over wear as well as the importance of continued care and compliance to a wearing, handling and replacement schedule. The patient was advised to return to clinic in 6 months for an annual comprehensive eye examination, dilated fundus examination, contact lens evaluation and new lenses.
Education Guidelines
Learning Objectives
At the end of the case discussion, participants should be able to:
- Recognize the hallmark diagnostic signs of aeruginosa keratitis.
- Discuss the visual consequences of central corneal scars.
- Recognize the benefits of scleral gas permeable contact lenses for irregular corneas.
- List the risk factors associated with microbial keratitis due to contact lens wear.
- Differentiate between aeruginosa the other organisms that can cause microbial keratitis.
Key Concepts
- Identifying signs and symptoms of aeruginosa keratitis.
- Differential diagnoses for microbial keratitis associated with contact lens overwear.
- Scleral gas permeable fitting and evaluation.
Discussion points
Knowledge, understanding and facts regarding this case presentation
- Describe the hallmark diagnostic signs and treatment of aeruginosa.
- List the risk factors associated with microbial keratitis from contact lens overwear.
Differential diagnosis
- List various causative organisms of microbial keratitis associated with contact lens overwear.
- Describe the characteristic signs of each possible cause of microbial keratitis.
Patient management
- Detail the appropriate treatment for aeruginosa.
- Describe ideal fitting of scleral gas permeable contact lenses for irregular corneas.
- List discussion points for patient education to prevent contact lens complications.
Critical-thinking
- When a contact lens patient presents with a painful red eye, can you identify the most likely causative organism?
- When fitting a patient with an irregular cornea with scleral lenses, can you describe an ideal fit?
Teaching methodology
The purpose of this teaching case report is to discuss the benefits of scleral lenses for irregular corneas. This case presentation could be added to a specialty contact lens lecture or course. Additionally, this case presentation identifies the findings associated with P. aeruginosa keratitis. Management of microbial keratitis should be understood by optometric students, residents and clinicians. This case report can be utilized in a grand rounds lecture or small group journal review to discuss the differentials and treatment for microbial keratitis.
Assessment
- Assessing in a classroom or small group setting with comprehension style test questions to identify the hallmark sign of aeruginosa and other microbial keratitis.
- Demonstrate application of knowledge by actively discussing the benefits of scleral contact lenses and describing an appropriate scleral lens fitting for irregular corneas.
- Advanced grand round style presentation and discussion to identify and manage microbial keratitis associated with contact lens over wear.
Discussion
Microbial Keratitis is a relatively uncommon but potentially devastating consequence of contact lens over wear. Patients typically report symptoms of acute ocular pain, redness, light sensitivity and reduced vision. One out of five hospitalized cases ultimately lead to corneal transplantation.7 Even with advances in contact lens technology such as higher oxygen permeability materials and more frequent replacement modalities, the incidence of MK has remained consistent over the last few decades.8 Overnight wear continues to be the greatest risk factor for MK. Extended wear soft contact lenses (CLs) have been shown to increase the risk of MK by four to seven times compared to daily wear soft CLs.3 Contact lens-induced corneal hypoxia is the main contributing risk factor for microbial keratitis with overnight wear. Other risk factors include poor storage hygiene, infrequent case replacement, smoking, male gender, socioeconomic status, absence of hand washing, misuse of disinfection system, exposure to water and over wear of contact lenses.8
P. aeruginosa is the most common cause of contact lens related ulcers (CLRU), found in over 60% of cases.3 P. aeruginosa is a gram-negative rod-shaped bacterium with flagella that adhere and invade corneal epithelium.3 Cytotoxic protease and elastase activity also contribute to the pathogenesis and severity of the keratitis. P. aeruginosa keratitis is typically described as a MK with a ring abscess, or an accumulation of polymorphonuclear leukocytes in a ring shape surrounding a central corneal lesion.5 Satellite lesions and hypopyon are also commonly found in P. aeruginosa keratitis.3
Other potential causes of MK in contact lens wearers are Staphylococcus aureus, Fusarium and Acanthamoeba.
Staphylococcus aureus, a gram-positive cocci, is a leading cause of keratitis in non-contact lens wearers.13 It has become a public health concern due to the development of resistance to antibiotic therapy.13 Methicillin resistant S. aureus (MRSA) ocular infections can result in corneal perforations , cellulitis and endophthalmitis.13 Fortified vancomycin is regarded as the standard in treatment of MRSA keratitis.13
Fusarium is a filamentous-septated fungi, which is the most common cause of fungal keratitis associated with contact lens wear.10 Fungal keratitis can be difficult to diagnose and treat. The hallmark of a fungal keratitis is a corneal ulcer with a dull gray infiltrate and satellite lesions.10 The infiltrate associated with fungal keratitis typically presents with feathery, branching borders.10 But advanced cases can look similar to bacterial keratitis. The incidence of fungal keratitis in contact lens wearers has decreased in the recent years due to a recall of certain multipurpose solutions.9
Acanthamoeba, a ubiquitous amoeba, is an uncommon but extremely painful and challenging form of keratitis to treat.9 Corneal ulcers from Acanthamoeba typically appear as ring shaped with perineural infiltrates.11 However, Acanthameoba infections have actually risen. The main risk factor for developing Acanthamoeba keratitis with contact lens wearers is improper lens care, specifically using tap water to clean or store lenses.11
Most cases of MK are managed and resolve without culturing. Culturing is optional in cases of small, peripheral corneal ulcers without stromal involvement. However, culture and smears are indicated in cases of a large, central corneal infiltrate or ulcer, especially if it extends into the deep stroma. Culturing is also helpful in cases of suspected fungal or acanthamoeba keratitis. For example, cases of trauma with vegetable matter or history of storing contact lenses in tap water should be cultured. 14
Visual correction after any type of MK is challenging if the patient has an irregular cornea and visually significant corneal scarring. Scleral gas permeable contact lenses are becoming a widely used treatment for irregular corneas. Scleral gas permeable contact lenses mask corneal irregularity and reduce higher order aberrations by creating a tear layer between the lens and the cornea.15
The ideal scleral contact lens should be vault the cornea limbus to limbus and land on the bulbar conjunctiva.16 Central clearance upon on initial insertion should range between 200-300 microns.16 The ideal central clearance after 4-6 hours of settling should measure 150-250 microns, however 50-100 microns may still be acceptable.16 Limbus clearance should measure between 50-100 microns in all four quadrants.16 The edge of the scleral lens should lay tangent on the conjunctiva without any compression or vessel impingement in all four quadrants.16 Large diameter gas permeable lenses with toric haptics can improve lens stability, comfort and wearing time.16, 17, 18, Anterior segment ocular coherence tomography may be utilized to quantify central and limbal clearance as well as image the scleral lens edge profile.16
Corneal scarring, whether secondary to infectious or non-infectious causes, may be managed using medical or surgical approaches. Superficial keratectomy and phototherapeutic keratectomy (PTK) are appropriate for the management of superficial stromal haze and opacities.19 Lamellar or penetrating keratoplasty was discussed in consultation with a corneal specialist. Due to the patient’s young age, however, corneal transplantation was not considered first-line therapy. Penetrating keratoplasty typically demonstrates graft survival of 15-20 years, while lamellar techniques may achieve greater longevity.19 As the patient was in their teenage years, a repeat graft would likely be required during their lifetime. Consequently, specialty contact lens intervention was considered the preferred initial management.
Conclusion
Patients who develop a central corneal ulcer from P. aeruginosa associated with contact lens over wear often must discontinue contact lenses indefinitely. Many patients may need penetrating keratoplasty if they have a visually significant corneal scarring. However, many patients may still request contact lenses as a visual correction for sports and other activities when penetrating keratoplasty is not recommended. This case demonstrates that scleral gas permeable lenses can be prescribed when other forms of contact lenses may not be ideal. Scleral lenses may improve vision beyond glasses or soft contact lenses when the cornea is irregular. In this case, the patient can maintain and enjoy an active healthy lifestyle by wearing scleral gas permeable contact lenses.
References
- Hedayati H, Ghaderpanah M, Rasoulinejad SA, Montazeri M. Clinical Presentation and Antibiotic Susceptibility of Contact Lens Associated Microbial Keratitis. J Pathog. 2015;2015:152767. DOI: 10.1155/2015/152767
- Poggio EC, Glynn RJ, Schein OD, et al. The incidence of ulcerative keratitis among users of daily-wear and extended-wear soft contact lenses. N Engl J Med. 1989 Sep 21;321(12):779-83. DOI: 10.1056/NEJM198909213211202
- Yildiz EH, Airiani S, Hammersmith KM, et al. Trends in contact lens-related corneal ulcers at a tertiary referral center. Cornea. 2012 Oct;31(10):1097-102. DOI: 10.1097/ICO.0b013e318221cee0
- Supiyaphun C, Jongkhajornpong P. Contact Lens Use Patterns, Behavior and Knowledge Among University Students in Thailand. Clin Ophthalmol. 2021 Mar 23;15:1249-1258. DOI: 10.2147/OPTH.S304735
- Oka N, Suzuki T, Ishikawa E, et al. Relationship of Virulence Factors and Clinical Features in Keratitis Caused by Pseudomonas aeruginosa. Invest Ophthalmol Vis Sci. 2015 Oct;56(11):6892-8. DOI: 10.1167/iovs.15-17556
- Giasson CJ, Morency J, Melillo M, Michaud L. Oxygen Tension Beneath Scleral Lenses of Different Clearances. Optom Vis Sci. 2017 Apr;94(4):466-475. DOI: 10.1097/OPX.0000000000001038
- Hoddenbach JG, Boekhoorn SS, Wubbels R, Vreugdenhil W, Van Rooij J, Geerards AJ. Clinical presentation and morbidity of contact lens-associated microbial keratitis: a retrospective study. Graefes Arch Clin Exp Ophthalmol. 2014 Feb;252(2):299-306. DOI: 10.1007/s00417-013-2514-1
- Young G, Young AG, Lakkis C. Review of complications associated with contact lenses from unregulated sources of supply. Eye Contact Lens. 2014 Jan;40(1):58-64. DOI: 10.1097/ICL.0b013e3182a70ef7
- Cheung N, Nagra P, Hammersmith K. Emerging trends in contact lens-related infections. Curr Opin Ophthalmol. 2016 Jul;27(4):327-32. DOI: 10.1097/ICU. 0000000000000280
- Mela EK, Anastassiou ED, Gartaganis SP, Christofidou M. Fungal isolation from disinfectant solutions of contact lens storage cases among asymptomatic users. Eye Contact Lens. 2015 Mar;41(2):87-90. DOI: 10.1097/ICL.0000000000000069
- Lee JS, Hahn TW, Choi SH, Yu HS, Lee JE. Acanthamoeba keratitis related to cosmetic contact lenses. Clin Exp Ophthalmol. 2007 Nov;35(8):775-7. DOI: 10.1111/j.1442-9071.2007.01622.x
- Schornack MM, Peterson D. Staphylococcus aureus ulcer associated with continuous wear of silicone hydrogel contact lenses. Eye Contact Lens. 2006 Mar;32(2):72-4. DOI: 10.1097/01.icl.0000174754.45463.84
- Chang VS, Dhaliwal DK, Raju L, Kowalski RP. Antibiotic Resistance in the Treatment of Staphylococcus aureus Keratitis: a 20-Year Review. Cornea. 2015 Jun;34(6):698-703. DOI: 10.1097/ICO.0000000000000431
- Lin, A., Rhee, MK., Akpen, EK. et al. Bacterial Keratitis Preferred Practice Pattern®. Ophthalmology. 2019 Jan;126(1):1-55. DOI: 1016/j.ophtha.2018.10.018
- Romero-Jiménez M, Flores-Rodríguez P. Utility of a semi-scleral contact lens design in the management of the irregular cornea. Cont Lens Anterior Eye. 2013 Jun;36(3):146-50. DOI: 10.1016/j.clae.2012.12.006
- Barnett, M, Fadel D. Clinical Guide for Scleral Lens Success. 1st ed. Essex, England: Contamac; 2018
- Visser ES, Visser R, Van Lier HJ. Advantages of toric scleral lenses. Optom Vis Sci. 2006 Apr;83(4):233-6. DOI: 10.1097/01.opx.0000214297.38421.15
- Visser ES, Visser R, van Lier HJ, Otten HM. Modern scleral lenses part I: clinical features. Eye Contact Lens. 2007 Jan;33(1):13-20. DOI: 10.1097/01.icl.0000233217.68379.d5
- Kelly TL, Williams KA, Coster DJ; Australian Corneal Graft Registry. Corneal transplantation for keratoconus: a registry study. Arch Ophthalmol. 2011 Jun;129(6):691-7. DOI: 10.1001/archophthalmol.2011.7

