
PEER REVIEWED
Posterior Segment Findings of Ocular Syphilis
Danielle Piser, OD, FAAO, Raman Bhakhri, OD, FAAO, Shaun Ittiara, MD
Abstract
Syphilis, caused by the spirochete, Treponema pallidum, primarily spreads through unprotected sex, manifesting in various parts of the body, including the eyes. Ocular syphilis, a subset to neurosyphilis, can cause irreversible vision damage and severe neurological effects. The rise in unprotected sex and the infection’s subtle early symptoms have resulted in an increased incidence of syphilis cases in the United States and globally. Optometrists can play a key role in identifying and diagnosing the risk for ocular syphilis due to its diverse eye-related presentations, mimicking other eye diseases. This teaching case report explores the posterior segment findings of ocular syphilis, emphasizing the importance of differential diagnoses, further testing, and referrals to address potential visual and systemic impacts. The key learning benefits of this case presentation are to recognize the posterior segment findings of ocular syphilis for prompt, appropriate referrals, diagnosis and treatment. The importance being optometrists can play an important role identifying risks for syphilis and providing care to maintain good visual potential in a condition that can cause irreversible vision loss. Due to the complexity and acquired knowledge needed to understand this case, third- and fourth-year optometry students and optometry residents are best suited to learn from this case.
Keywords
Introduction
Syphilis is a sexually transmitted infection (STI) caused by the spirochete, Treponema pallidum. Although thought to be a rare infection, syphilis cases have been on the rise over the last 20 years in the US and globally. Per the Centers for Disease Control and Prevention (CDC), there were over 200,000 cases of syphilis in 2022, which was the greatest number of cases since 1950, with an increase of 17% since 2021.1 The World Health Organization (WHO) estimates globally, that 11 million new cases of syphilis occur in adults 15 to 49 years of age.2 This is considered to be due to an increase in HIV preventive medications, an increase in unprotected sex, especially in young men who have sex with men, and decreased public health initiatives. Although there has been an increase in documented cases of primary and secondary syphilis, neurosyphilis (including ocular syphilis) numbers have not been well documented.3
There are four categories of syphilis defined by the CDC, which are based on the stage of the infection and the tissues/organs affected: primary, secondary, latent and tertiary. The primary stage of syphilis occurs when the infection enters the body, presenting as a sore(s) or chancre(s) at the inoculation site. These sores most often affect the penis, vagina, anus, rectum, mouth and can last 3-6 weeks. These chancres are typically firm, red and painless, which may lead to them going unnoticed by patients and therefore remaining untreated. Untreated syphilis will progress to the secondary stage. Although the knowledge of pathogenesis in humans is unclear, animal models show the infection spreads from the inoculation site to the lymph nodes, spreading throughout the body in its early stages.3 In the secondary stage, a non-itchy rash will typically arise at the sore location or on the palms of the hands or bottom of the feet. Flu-like symptoms can also occur in this stage, as well as weight loss and hair loss. The infection can be fought off partially from the body’s adaptive immune response, but if left untreated, T. pallidum can persist for years by impacting immune-privileged sites, such as the eye, and the infection will enter the latent stage or tertiary stage.3 In the latent stage, the infection becomes asymptomatic and can persist in a patient’s body for years. Individuals in the latent stage remain contagious and will test positive in serological tests; increasing the spread of syphilis if not treated. The infection enters the tertiary stage years after being latent or can be a result of progression from the secondary stage. Although uncommon, the tertiary stage of untreated syphilis will start to affect major organs, such as the heart, blood vessels, brain and nervous system. When syphilis affects the neurological system, including the eye, it is termed neurosyphilis. Neurosyphilis can occur in any stage of syphilis but is most likely to occur in the secondary stage. Optometrists play a key role in the detection of syphilis risks as it may manifest in the eye, including the posterior segment. Therefore, it is essential for eyecare providers to recognize the signs and symptoms of ocular syphilis, understand appropriate diagnostic approaches, and be familiar with current treatment strategies to support optimal visual outcomes and overall patient health.
This teaching case report is valuable for third- and fourth-year optometry students and residents, as it underscores the diverse posterior segment manifestations of ocular syphilis and highlights the importance of prompt recognition, evaluation and treatment to preserve visual potential and prevent further systemic complications. Additionally, an overview of ocular syphilis is presented, covering its epidemiology, pathophysiology, potential ocular differential diagnoses, testing modalities and treatment options.
Case Description
A 71-year-old African-American male presented with complaints of pain in the left eye and on the left frontal side of the head that started 3 days prior. He also noticed an increase in flashes and floaters in the left eye and a “black blob” in the center of his vision with only mild improvement since the initial occurrence. His ocular history was positive for primary open angle glaucoma and posterior vitreous detachments in both eyes. The patient had a history of insulin-dependent type 2 diabetes, hypertension and hyperlipidemia. He stated his last hemoglobin A1C to be around 7% and his last blood sugar reading earlier that morning to be 97mg/dL. His current medications were ezetimibe, Lantus, lisinopril, 81mg aspirin, preservative free artificial tears, and latanoprostene bunod 0.025% (Vyzulta 0.025%). He reported good compliance with all systemic and ocular medications.
The entering best-corrected visual acuity in the right eye was 20/20, whereas the left eye demonstrated a reduction to 20/600 with no improvement upon pinhole testing, compared with a documented acuity of 20/20 at his glaucoma follow-up examination 1 month earlier. Confrontational visual fields, extraocular motility and pupils were unremarkable in both eyes. His slit lamp findings were remarkable for grade 1 nuclear cataract in both eyes with no evidence of anterior chamber cell or flare in either eye. His intraocular pressure (IOP) was stable at 12 mmHg in both right and left eyes, measured by Goldmann Applanation Tonometry. A dilated fundus exam was performed on both eyes. Glaucomatous cupping of .8/.8 in the right eye was noted with a stable posterior vitreous detachment (PVD) but was otherwise unremarkable. A dilated fundus examination of the left eye was limited by significant vitreous haze and the presence of pigmented vitreous cells versus vitreous hemorrhage (Figure 1).

Figure 1. Presenting wide field imaging of the poster segment clinical findings day one. Blue arrow: Posterior vitreous detachment. Red Arrow: Pre-retinal hemorrhage. Yellow Arrow: Vitreous hemorrhage/cells obscuring views to underlying retina and the optic nerve, which appears edematous and pale. Click to enlarge
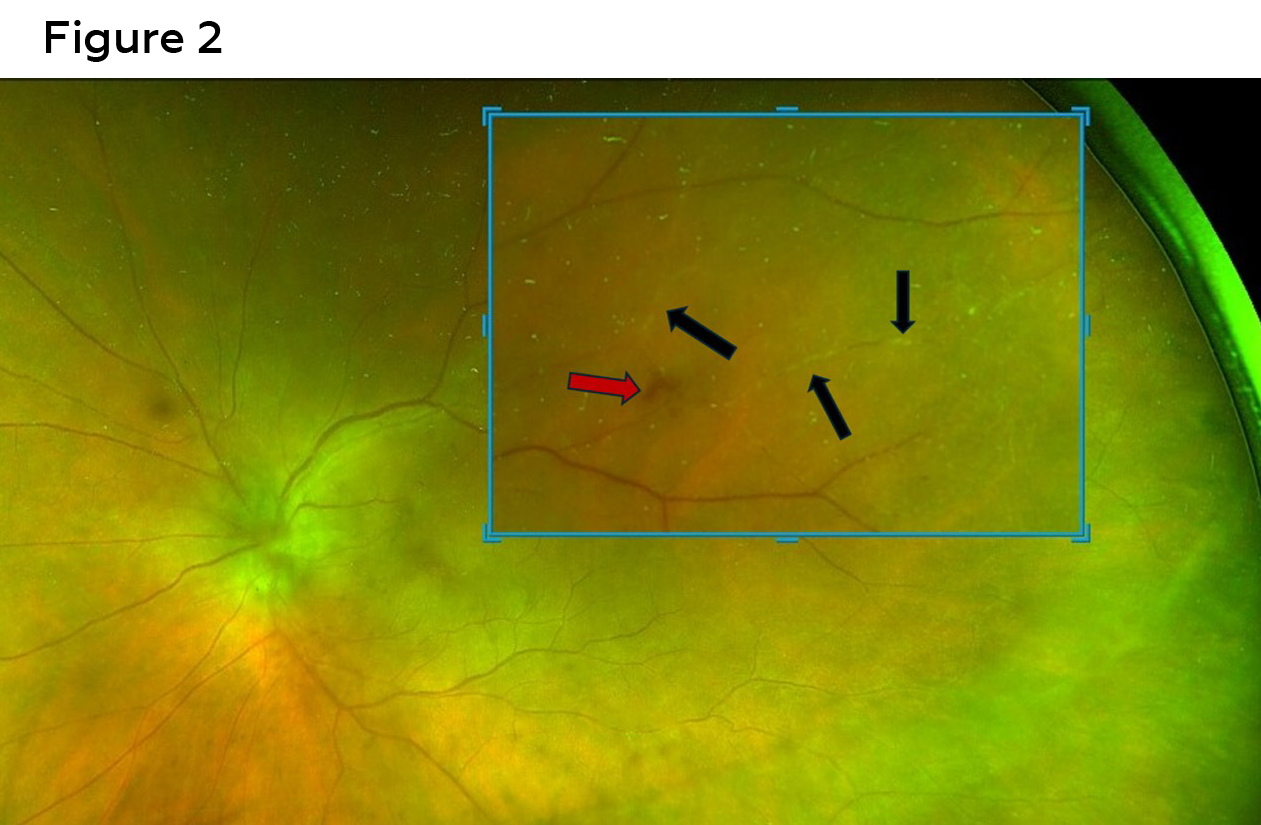
Figure 2. Magnified imaging of Figure 1 (day 1) demonstrating retinal periarteritis plaques (black Arrows) and preretinal hemorrhage (red arrow). Click to enlarge
The optic nerve was also obscured but appeared to have disc edema and pallor (Figure 2). The patient declined symptoms of scalp tenderness, jaw claudication, fever, malaise or muscle pain or weakness. As mentioned in above entrance testing, no APD was present declaring that the optic nerve head edema was mild and optic nerve function still preserved. The superior temporal mid-peripheral retina showed retinal hemorrhages, sclerotic vessels and vessel plaques with hazy views (Figures 1 and 2).
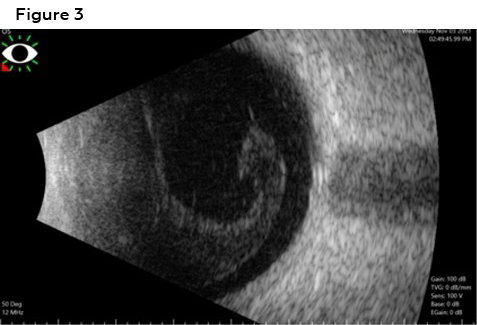
Figure 3. B-scan ultrasound obtained on day 1 confirming large vitreous debris (vitreous hemorrhage vs vitreal cells). Click to enlarge
As views were limited, a B-scan ultrasound was ordered and confirmed no retinal detachment. However, a large vitreous body (vitritis vs vitreous hemorrhage) was visualized (Figure 3). A spectral domain optical coherence tomography (SD-OCT) macular scan of the left eye was ordered due to decreased vision, poor views upon dilation, as well as retinal and vascular findings that could point to macular edema. The macular SD-OCT showed a loss of foveal contour with internal limiting membrane (ILM) traction, retinal pigment epithelium (RPE) disruption, and a loss of the ellipsoid zone (EZ) nasal to the fovea (Figure 4).
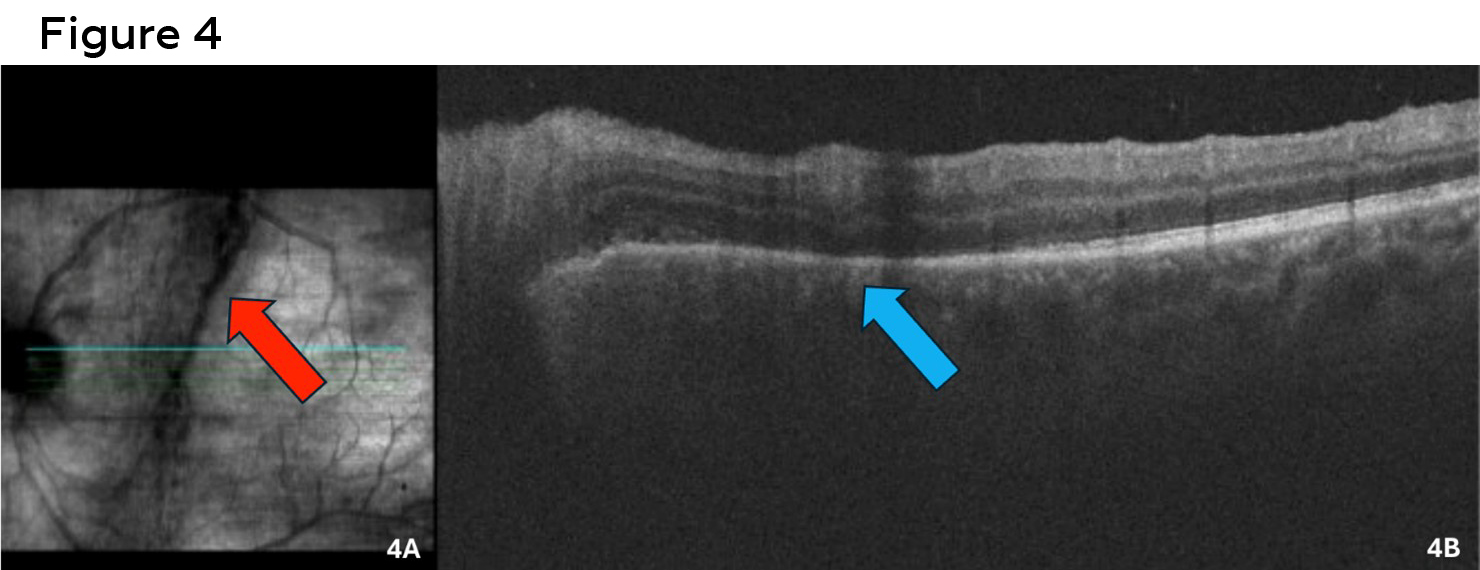
Figure 4. Day 1 Cirrus SD-OCT 5-line raster scan. 4A: Vitreal cells/heme are noted on the infra-red scan as a pre-retinal black shadow (red arrow). 4B: OCT of the macula revealing nasal disruption to the ellipsoid zone (light blue arrow). Click to enlarge
Differential Diagnoses at this time were:
Anterior ischemic optic neuropathy4
Non-atretic anterior ischemic optic neuropathy (NAAION): This condition occurs due to hypoperfusion of the short posterior ciliary arteries supplying the optic nerve that leads to acute ischemia, resulting in axonal swelling. This leads to compression of the optic nerve circulation, increasing optic nerve swelling and ischemia.
-
- Symptoms/Signs: Acute, monocular, painless loss of vision with diffuse or segmental optic disc edema with peripapillary flame hemorrhages.
- Etiologies: Vasculopathic diseases (diabetes, smoking, hypertension and hypercholesterolemia), use of phophodiesterase-5 inhibitors (i.e. sildenafil), small cup to disc ratio (aka “disc at risk”), or ocular surgeries (due to the rise of perioperative IOP leading to a decrease in optic nerve perfusion).
- This diagnosis was excluded based on the pallor of the affected optic nerve, the absence of flame hemorrhages and the vitreous presentation. Furthermore, comparison with the fellow eye revealed no evidence of a “disc at risk” appearance.
Arteritic anterior ischemic optic neuropathy (AAION): This results from endothelial cell inflammation secondary to giant cells, leading to thrombosis and occlusion in the posterior ciliary artery of the optic nerve head, leading to optic nerve head swelling.
-
- Symptoms/Signs: Acute vision loss with or without headache, scalp tenderness, jaw claudication, fever, malaise or muscle pain or weakness (symptoms related to giant cell arteritis (GCA)). Pale optic nerve edema typically without disc hemorrhages.
- Etiologies: GCA or systemic or ocular vasculitis caused by polyarteritis nodosa, systemic lupus erythematosus or herpes zoster.
- AAION was ruled out based on the presence of vitreal signs and lack of associated symptoms.
Optic Neuritis5
Definition: Inflammatory infiltration of the optic nerve head causing swelling of the optic nerve.
-
- Signs/Symptoms: Typical optic neuritis, often associated with demyelinating disease, presents as an acute, unilateral and painful loss of vision. In contrast, atypical optic neuritis—typically related to infectious or autoimmune etiologies—is less commonly associated with ocular pain.
- Etiologies: Infection (i.e., tuberculosis, syphilis, sarcoidosis, cat-scratch disease, herpes zoster), demyelination disorders (i.e. multiple sclerosis), or auto-immune conditions (i.e., lupus or Sjogren’s).
- This condition could not be excluded at this stage given the appearance of the patient’s optic nerve, and further evaluation and diagnostic testing were warranted.
Vitreous hemorrhage6
Definition: Blood in the vitreous due retinal vascular blood leakage.
-
- Symptoms/signs: Increase in floaters, hazy vision, shadowing of vision or cobwebs in vision. Blood or pigmented fibers floating in the vitreous, occluding retinal views.
- Etiologies (Limited to the likely differentials associated with the case presented): Proliferative vascular retinopathies (caused by diabetes), vein occlusions, vasculitis from infections such as HIV, CMV, syphilis, etc., sickle-cell, idiopathic polypoidal choroidal vasculopathy, trauma, retinal arterial macroaneurysm, posterior vitreous detachment, blood disorders (leukemia, anemia, thrombocytopenia or hemophilia), or Valsalva retinopathy.
- This differential could not be excluded based on the retinal presentation, the patient’s symptoms or systemic conditions such as diabetes and hypertension.
Posterior uveitis
Definition: A type of uveitis defined by Standardization of Uveitis Nomenclature (SUN) primarily affecting the choroid and the retina causing chorioretinal inflammatory lesions. This condition includes choroiditis, retinochoroiditis, retinitis or neuroretinitis.7 There are two classes in posterior uveitis; infectious and non-infectious, where non-infectious primarily affects the choroid.8
-
- Symptoms/signs:9 Sudden onset of floaters, blurred vision, loss of vision or distorted vision. Retinitis will appear as poorly defined, superficial white patches, while choroiditis lesions are yellow with regular borders, deeper to the retinal vessels.
- Etiologies:9 (Limited to the likely differentials associated with the case presented):
- Infectious: cytomegalovirus (CMV), toxoplasmosis, herpes, tuberculosis (TB), syphilis, fungal infections or histoplasmosis.
- Non-infectious with systemic association: sarcoidosis or Behcet’s disease.
- Non-infectious without systemic association: Multifocal chorioretinitis/panuveitis, multiple evanescent white dot syndrome/placoid retinitis.
- This differential couldn’t be excluded due to ocular findings, patient’s symptoms and need for further imaging and blood work.
Vitritis (intermediate uveitis)10
Definition: Inflammatory material (white blood cells) found in the vitreous from an infectious or inflammatory condition.
-
- Symptoms/signs: Unilateral or bilateral blurry vision with or without floaters. Will observe cells floating in the vitreous. Collections of inflammatory material seen at the inferior vitreous base, known as snowballs or if located at the pars plana or anterior retina, are referred to as snowbanks.
- Etiologies (Limited to those most risk associated with the case presented): Caused by conditions such as toxoplasmosis, cytomegalovirus, herpetic disease, syphilis, tuberculosis or Behcet disease.2 Other causes for vitreous cells include lymphoma, melanoma, rhegmatogenous retinal detachment, leukemia or amyloidosis.11
- This is a differential that can’t be excluded due to the patient’s posterior pole findings, symptoms and need for a further blood workup.
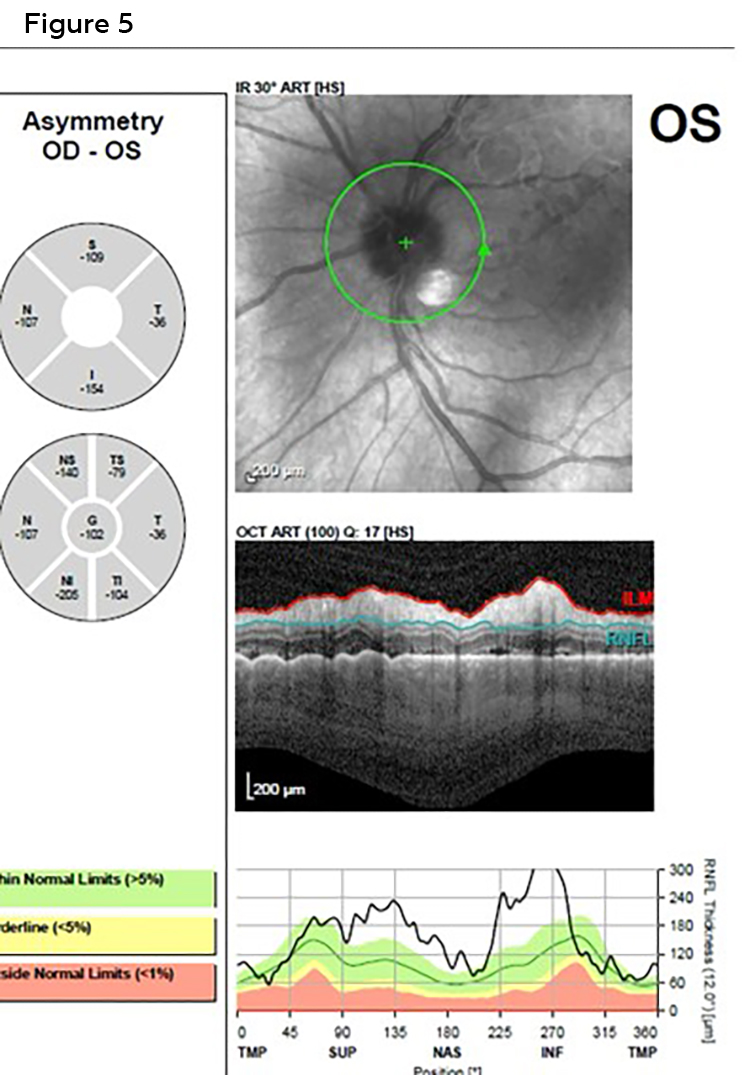
Figure 5. Spectralis OCT of the left optic nerve on day 2, with the retinal specialist. Optic nerve edema is appreciated based on indistinct disc margins on the infrared (IR) scan (green arrow) as well as the retinal nerve fiber layer scan, especially in the inferior quadrant (blue line). Click to enlarge
Based on the patient’s posterior segment findings and vitreous involvement, he was diagnosed with presumed posterior and intermediate uveitis of unknown etiology. Additional case history was obtained to assess new systemic conditions, recent changes in routine blood work (performed every 3 months), and symptoms such as fatigue, flu-like illness, chest pain, increased cough, dyspnea or features suggestive of GCA. He denied any of these changes or symptoms. Unfortunately, at this time, sexual history questions were not inquired about. He was referred immediately for a retinal consultation for further evaluation.
A retinal specialist saw the patient the next day (day 2) noting stable and unremarkable findings in the right eye with BCVA at 20/20. The left eye BCVA had improved to 20/200. Entrance testing was unremarkable, including pupils. Anterior segment examination via slit lamp remained stable with no changes or new findings. A grade 1+ vitreous hemorrhage was noted with vitreous cells indicating the likelihood of inflammatory driven vasculitis resulting in retinal ischemia and secondary retinal neovascularization. The optic nerve was visible and confirmed optic nerve head edema nasally with general congestion and hyperemia without hemorrhages (Figures 1, 5 and 6). A Spectralis SD-OCT of the optic nerve was performed as well to confirm the optic nerve swelling (Figures 5 and 6).
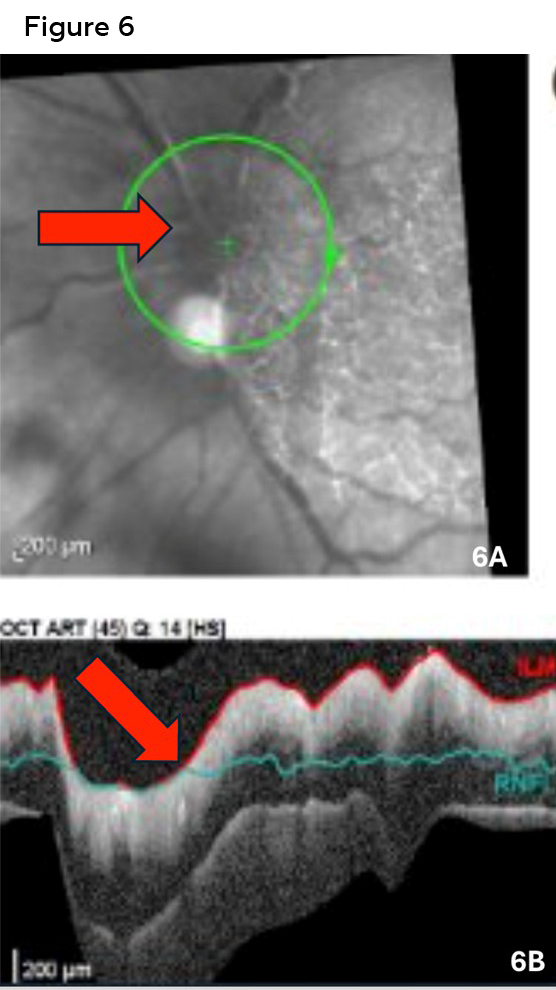
Figure 6. Spectralis OCT of the optic nerve at the 2 week follow-up visit. 6A: Infra-red (IR) scan showing obvious and worsening optic nerve head edema (red arrow) compared to the patients 2-day visit (Figure 5). 6B: Retinal nerve fiber layer scan showing worsening edema as compared to the initial scan (Figure 5). Click to enlarge
Sclerotic vessels and retinal periarteritis plaques consistent with retinal vasculitis (Figure 2), as well as pre-retinal hemorrhages in the left eye (Figure 1) were also evident. Because of these findings, the retinal specialist ordered an intravenous fluorescein angiogram, which demonstrated severe perfusion delay in the left eye with poor filling of the superior-temporal artery with noted plaques indicating retinal ischemia. Preauricular nodes (PAN) were palpated, and the left PAN was palpable, indicating a possible viral infection. He denied feelings of malaise, flu-like symptoms, dental issues, ear infections or cancer. He denied family or personal past history of sickle cell anemia. He also confirmed negative giant cell arteritis symptoms (scalp tenderness, fever, chills and jaw claudication).
Further questioning of the patient’s sexual history was asked at this visit and the patient disclosed he was sexually active with other men. Based on the posterior segment findings of optic nerve papillitis, retinal vasculitis, vitritis, and the patient’s history, posterior/intermediate uveitis of unknown inflammatory or infectious origin was suspected. To rule out infectious or inflammatory conditions, the patient was referred for comprehensive blood work including a CBC with differentials and a uveitis work up including rheumatoid factor, syphilis testing including Rapid Plasma Reagin (RPR) non-treponemal testing and Treponema pallidum particle agglutination-treponemal (TP-PA) testing, chest radiography, serum ACE and lysozyme, Lyme serology, QuantiFERON Gold for tuberculosis, ELISA Bartonella serology, viral polymerase chain reaction for herpes simplex, zoster, HIV and cytomegalovirus, and antibody titers for toxoplasmosis and toxocariasis. A magnetic resonance imaging (MRI), magnetic resonance angiography (MRA), magnetic resonance venography (MRV), computed tomography (CT) and computed tomography angiography (CTA) of the brain and orbits without contrast were ordered to rule out malignant or benign lesions, vascular abnormalities (i.e. aneurysms), as well as demyelinating diseases. Due to the lack of patient’s symptoms and presence of vitritis, GCA blood work including ESR and CRP was not ordered. Although ESR and CRP are commonly ordered in cases of uveitis, it was determined that these tests would not contribute meaningfully to the diagnosis, as they indicate only the presence of systemic inflammation and are not specific to any particular underlying etiology. Therefore, in this case, more specific testing was ordered to determine it was infectious.
The patient’s syphilis testing revealed a reactive Rapid Plasma Reagin (RPR) indicating the need for Treponema pallidum Particle Agglutination (TP-PA) treponemal testing, which concluded a reactive result, confirming the diagnosis of syphilis. The MRI of the brain and orbits without contrast confirmed active left optic nerve enhancement as well. All other test results and imaging were unremarkable. The patient was diagnosed with neurosyphilis based on ocular involvement (posterior uveitis), optic nerve involvement per the MRI and ocular exam findings and serological testing. Neurosyphilis (likely tertiary or late latent stage syphilis) was diagnosed based on the optic nerve and retinal findings, as well as no other primary or secondary stage findings of rash, chancres or anterior uveitis. He was immediately referred and admitted to the emergency department for IV antibiotics (penicillin G) to treat his neurosyphilis. At this time, he confirmed he was engaged in high-risk sexual behavior and educated to notify all sexual partners regarding his confirmed syphilis diagnosis.
The patient’s non-treponemal titers improved after a 14-day treatment of intravenous penicillin G. The patient followed up multiple times with a retinal specialist over the next 2 years with no signs of retinal necrosis, neurological manifestations or vision loss. The patient continued to follow up with an infectious disease specialist and presently his syphilis is non-detectable per his serological non-treponemal titers. The patient continues to show no further systemic manifestations related to syphilis. On his last visit, his visual acuity improved to 20/30 in the left eye. Current ocular findings of the posterior pole can be seen in Figure 7 showing optic nerve pallor with vitreal traction, retinal periarteritis plaques within the vessels, as well as sclerotic vessels and residual retinal hemorrhages. The patient continues to be seen by the retinal specialist every year. His glaucoma care is managed every 3 to 6 months by his optometrist. He continues to see his infectious disease specialist annually.
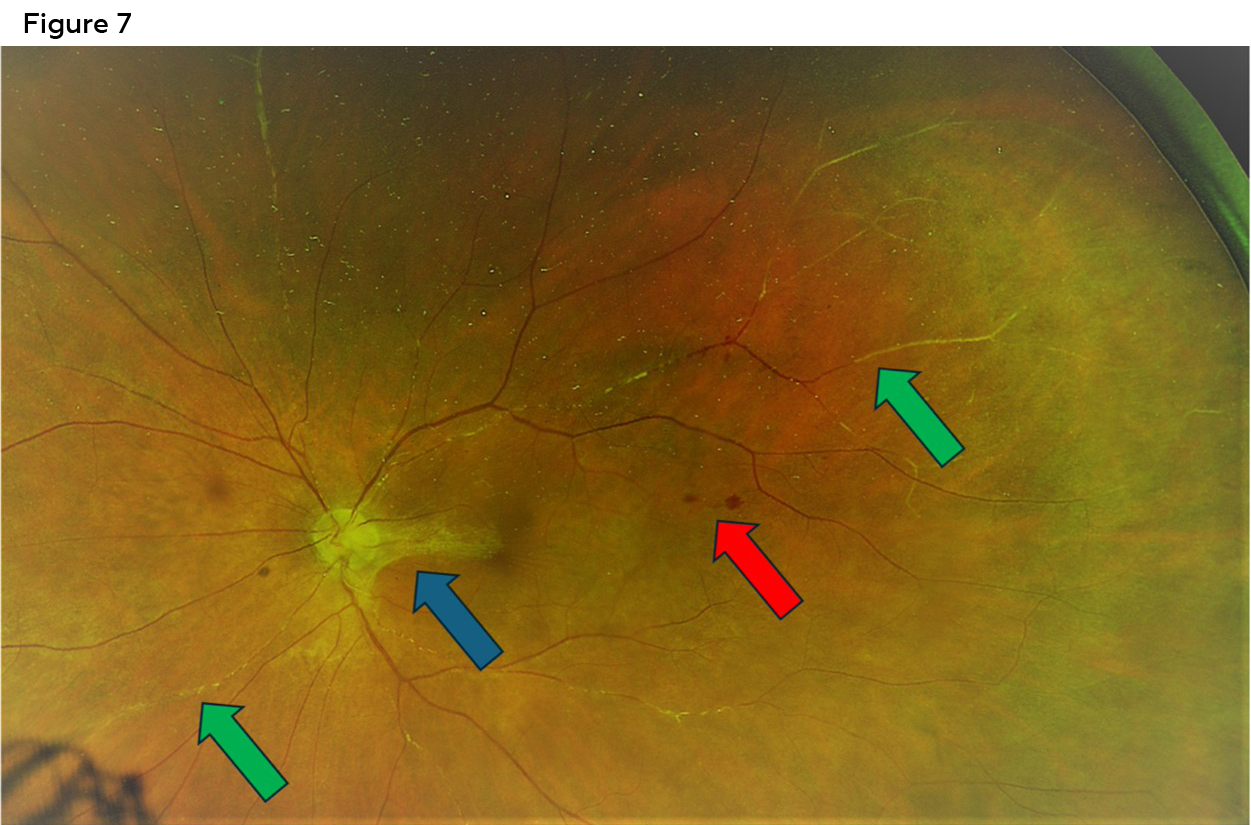
Figure 7. Optos wide field imaging 8 months after initial onset. Vision at this time was 20/30. Blue arrow: Traction and vitreal scarring from nerve to macula. The optic nerve appears pale due to the resolution of the initial optic nerve edema. Light green arrows: Sclerosed vessels from resolution of vasculitis. Red arrow: Residual intra retinal hemorrhages. Click to enlarge
Educational Guide
This educational guide can be utilized in a multitude of ways to teach students and/or residents’ knowledge about posterior segment findings that can be associated with syphilis. The learning objectives, key concepts and discussion questions provided below can be helpful for an educator to use the case to further expand student knowledge and understanding of ocular syphilis presentations in the posterior segment.
The case could be presented to students/residents in a grand rounds format after a PowerPoint lecture presentation using this case report’s findings as an example for posterior segment findings of syphilis. Followed by a multiple-choice test focusing on the discussion questions below. The case can also be presented in a clinical setting or a systemic/ocular disease course with one student/resident or a group of students/residents.
For example, instructors may present the specific case findings and prompt students to develop differential diagnoses, identify appropriate additional testing, determine necessary referrals and systemic evaluations, and formulate the final diagnosis. Subsequent discussion of treatment strategies and management considerations would further illustrate how this case and the accompanying educational guide can be effectively utilized.
Assessment of students’/residents’ analytical skills may be accomplished through case-based discussion lectures, guided verbal analysis of clinical decision-making or written case reports following the format outlined above.
Learning Objectives
-
- Recognize the importance of case history questioning and using specific questionnaires to identify the risks for syphilis with specific posterior segment presentations arise.
- Recognize posterior segment presentations caused by ocular syphilis.
- Identify appropriate ophthalmic testing, laboratory testing and neuroimaging required when suspecting ocular syphilis.
- Identify other professionals needed to collaborate with when managing a patient with ocular syphilis.
Key Concepts
-
- Understand/correlate the stages of syphilis and when posterior segment manifestations of ocular syphilis are likely observed.
- Development of appropriate case history questions for those suspected of ocular syphilis.
- Use of specific ocular and laboratory investigations to aid in diagnosing ocular syphilis.
- Treatment and management of ocular syphilis in the posterior segment.
Discussion Questions
-
- What is the epidemiology of ocular syphilis and why is there a growing concern?
- What is the pathophysiology of syphilis and ocular syphilis?
- What are the stages of syphilis and in what stage(s) do posterior segment manifestations occur?
- What are the signs and symptoms of ocular syphilis in the posterior pole?
- What signs and symptoms did the patient demonstrate in this case?
- What are the most likely differential diagnoses for posterior segment involvement of ocular syphilis based off chief complaints, systemic findings, personal medical and social history and ocular signs and symptoms?
- What are important ocular examination tests and systemic testing that need to be considered to make a prompt diagnosis of ocular syphilis?
- What tests were used to help diagnose the patient in this case?
- Were there other tests that should have been considered and why?
- What are the recommended treatment and management strategies for systemic neurosyphilis and ocular syphilis?
- What other healthcare providers should optometrists co-manage with when managing patients with ocular syphilis?
- What healthcare providers did the patient in this case obtain care from?
- Are there other healthcare providers that should have been involved in this case?
Discussion
Epidemiology and growing concern of ocular syphilis
Consequently, the resurgence of syphilis has been accompanied by an apparent increase in cases of ocular syphilis. However, because ocular involvement is often underreported, the true magnitude of this increase remains difficult to quantify. The CDC reported in 2016 that it received over 200 cases of ocular syphilis from 20 states over the years of 2014 to 2016.12 Multiple studies from US, Canada and China have shown that 0.50% to up to 2.6% of those diagnosed with syphilis had ocular syphilis.13 The incidence in ocular syphilis and its increase can also vary due to exam coding variability and cases without hospitalizations.12 Most of the incidences of ocular syphilis manifest in the form of uveitis. A study using the codes of “syphilis and uveitis” extracted from the National Inpatient Sample data records for hospitalized patients in the US from 1998 to 2009 reported the annual incidence 4 per million persons.2,7 A study in Baltimore reported that from 2013 to 2017 there were 5 cases of ocular syphilis reported per year versus 1.7 per year from 1984 to 2014 in academic and community clinical settings.13,14
Neurosyphilis, ocular syphilis and otic syphilis, also known as NOO syphilis, is not available as a single national rate, but a CDC report found that 1.5% of all syphilis cases in California and Chicago in 2023 were NOO syphilis.15 In that same 2023 Chicago report, 60% of those NOO cases were ocular syphilis cases.15
Pathophysiology
The only vector for the spread of syphilis is humans via sexual contact. The bacteria,Treponema palladium (T. pallidum), infects the human immune system quite easily due to the unrecognizable cell membrane of the bacteria making it difficult for the immune cells to identify and ward off quickly.16 The immune response is therefore slow and will allow the bacteria to incubate in the body for up to 3 months.16 This infection leads to chancre formation. Syphilis is spread through chancres, a primary or secondary stage of infection, found on the external genitals, vagina, anus/rectum and mouth. These chancres are often missed or are asymptomatic, and individuals go undiagnosed for years, leading to more transmission since individuals don’t seek care or treatment. Once the painless chancre blisters are exposed, the bacteria can spread via contact with another via mucosal exchange. This leads to lymphadenopathy, causing it to spread to other organs such as the eyes or brain where it can cross the blood-retinal and blood-brain barriers. The inflammation from the immune response created by T. pallidum over the years leads to further ocular findings. T. pallidum also is known to localize to immune-privileged sites, such as the eye, taking on a minimally metabolically active latent form allowing it to persist in the human body for years.13,17
Stages
The main stages of syphilis are primary, secondary, latent and tertiary. Syphilis most often spreads during the primary and secondary stages of the disease via sexual contact orally, vaginally or through the anus. Infectivity is high with an estimated per partner transmission up to 60% especially with men who have unprotected sex with other men.13,18 Ocular involvement can occur at any stage of syphilis, but commonly is found during the secondary stage of the infection presenting as anterior uveitis, however ocular syphilis involving the posterior segment is often associated with the tertiary or late latent stages of the infection.
The primary stage of the disease has an incubation period of 25 days, after which a chancre forms.13,19 The chancre tends to be painless, but ulcerated, with non-purulent discharge that spontaneously resolves even without treatment.20 Again, the chancre will occur at the inoculation site (vagina, penis, anus or mouth) as well regional lymphadenopathy.
The secondary stage occurs 1-2 months after the primary stage due to T. pallidum’s dissemination.20 In this stage the individual can appear to have a maculopapular rash, most commonly found on the palms of the hand or feet, fever and generalized lymphadenopathy that often will spontaneously resolve.21
If the secondary stage is left untreated, the patient can enter latent syphilis, an asymptomatic phase. Latent syphilis can recur within 1 year after exposure (early latent stage) or more (late latent stage), remaining infectious and still detectable on serological testing, allowing for further transmission.22 In the late latent stage, about 70% of patients maintain lifetime latency and 30% progress to the tertiary stage.23
The tertiary stage occurs 2-50 years after infection and has the most long-term complications including cardiovascular syphilis, ocular syphilis, otic syphilis, gummatous disease and late neurosyphilis.20 Late neurosyphilis occurs 5-12 years after the initial infection and can cause general paresis as well as damage to the meninges of the nervous system, which can eventually lead to death.20,24,25
Posterior Segment Presentations of Ocular Syphilis
Intermediate Uveitis25
- Vitritis: Vitreal cells appear in ocular syphilis to be have a round, white-like appearance and are multiple in numbers.16 The patient’s vitreal appearance in this case report presented differently with more diffuse haziness and a large coalescing of vitreous cells as seen in Figures 1 and 2. The difference in appearance may be attributable to a combination of inflammatory cells and vitreous hemorrhage secondary to the underlying vasculitis.
Posterior Segment findings (Often presenting as posterior uveitis)
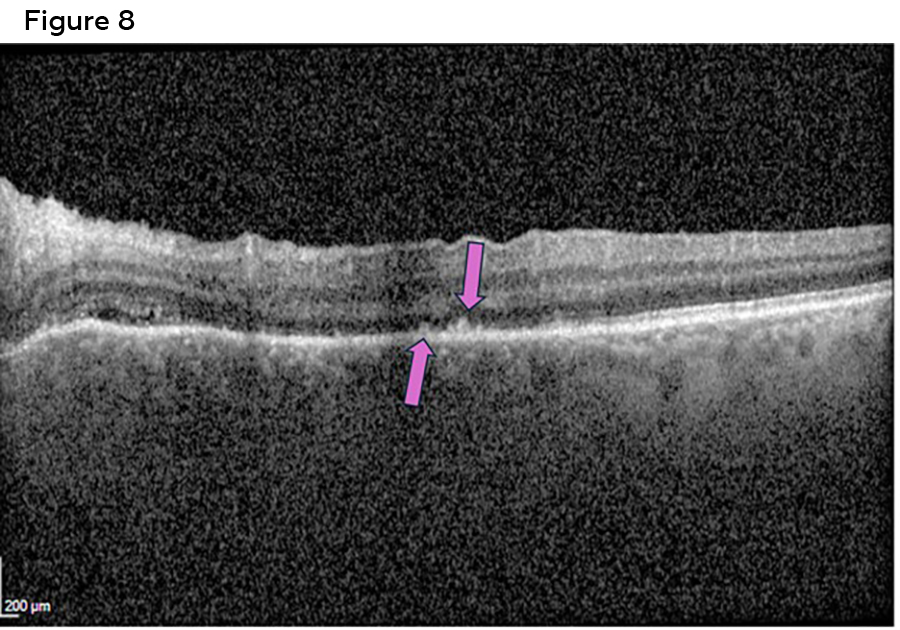
Figure 8. Spectralis OCT macula scan 1 week after initial presentation showing acute posterior placoid chorioretinopathy (purple arrows), often a distinguishing feature of ocular syphilis. Click to enlarge
- Posterior scleritis (rare): Global inflammation to the globe of the outer tunic of the eye affecting superficial and deep capillary networks.26
- Posterior Uveitis:
- Chorioretinitis/Acute posterior placoid chorioretinopathy (ASPPC) (a distinguishing feature of ocular syphilis): This finding appears as yellowish, poorly defined placoid lesion(s) that is often located in the mid-periphery or posterior pole of the fundus.20,27 These lesions are characterized by a faded center surrounded with hyperpigmentation of the retinal pigment epithelium (RPE).20 In this case, the patient’s foveal SD-OCT in Figure 8, shows early placoid chorioretinopathy within the posterior pole confirming chorioretinitis is present and the likelihood of a syphilis infection.
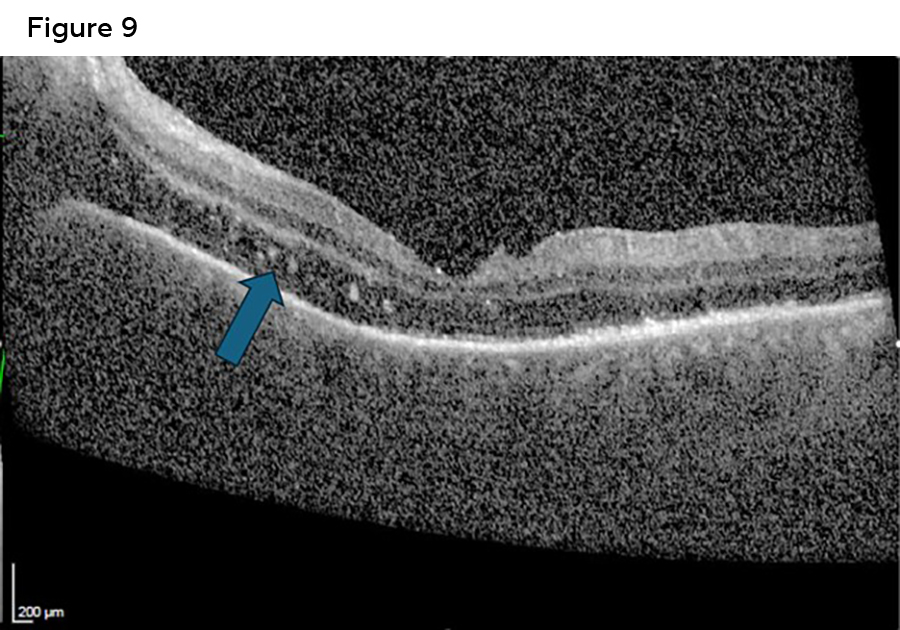
- Focal retinitis/syphilitic punctate inner retinitis (migrating superficial retinal precipitates): Multiple, small, white inflammatory pre-retinal or inner-retinal deposits that form in areas of active retinitis. They are associated with retinal vasculitis leading to retinal pigment epithelium damage. OCT findings will show hyper-reflective dots in the inner retina.28 These inflammatory precipitates were observed in this case report as seen in Figure 9.
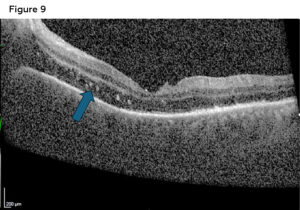
Figure 9. Spectralis OCT macula scan 1 week after initial presentation showing syphilitic punctate inner retinitis (blue arrow). Click to enlarge
- Retinal vasculitis (common): Inflammation of the retinal vessels (arteries, veins and/or capillary networks). This leads to sheathing, perivascular cuffing, perivascular exudation and vascular occlusions leading to pre-retinal hemorrhages, vitreous hemorrhage and neo-vascularization.28, 29 Retinal vasculitis findings of pre-retinal and vitreous hemorrhages , as well as vessel sheathing were observed in our patient as seen in Figures 1, 2 and 7.
- Necrotizing retinitis/syphilis retinal necrosis (SRN): Presents after severe inflammation of the retina that causes death of the retinal tissue leading to irreversible vision loss. It appears as coalescing multifocal lesions that start from the posterior pole and have a layer of exudative membrane obscuring the underlying retina, appearing more mottled.16, 28 Fortunately, in the case presented the patient never developed retinal necrosis.
- Exudative retinal detachment: Occurs when fluid leaks into the sub-retinal space due to disruption of the blood-retinal-barrier (BRB) from inflammation, which causes ischemia to the BRB cells.30 Fortunately, the patient in the case report didn’t experience a retinal detachment of any kind.
- Optic disc edema: The optic disc can be affected in one or both eyes. This can present as anterior or retrobulbar optic neuritis.16 Disc edema was a finding presented in this case as seen in Figure 1, as well as confirmed via the patient’s MRI.
Neurological findings25
- Argyl Roberston pupils: Bilateral, asymptomatic, mitotic, pupils, with anisocoria. Pupils don’t constrict in bright light but constrict with convergence/accommodation (light-near dissociation) and with poor dilation caused by tertiary syphilis.
Differentials for posterior ocular syphilis (Most common of the “Great Masquerader/Mimicker”)16, 31
- Diabetic retinopathy
- Retinal detachment
- White dot syndromes including but not limited to multiple evanescent white dot syndrome (MEWDS)
- Other infectious retinitis (i.e. toxoplasmosis, CMV, HSV)
- Other vasculitis causes (i.e. TB)
- Acute retinal necrosis (ARN)/Progressive outer retinal necrosis (PORN)
- Central serous chorioretinopathy
- Anterior/retrobulbar neuritis due to demyelinating diseases
- Ischemic optic neuropathies
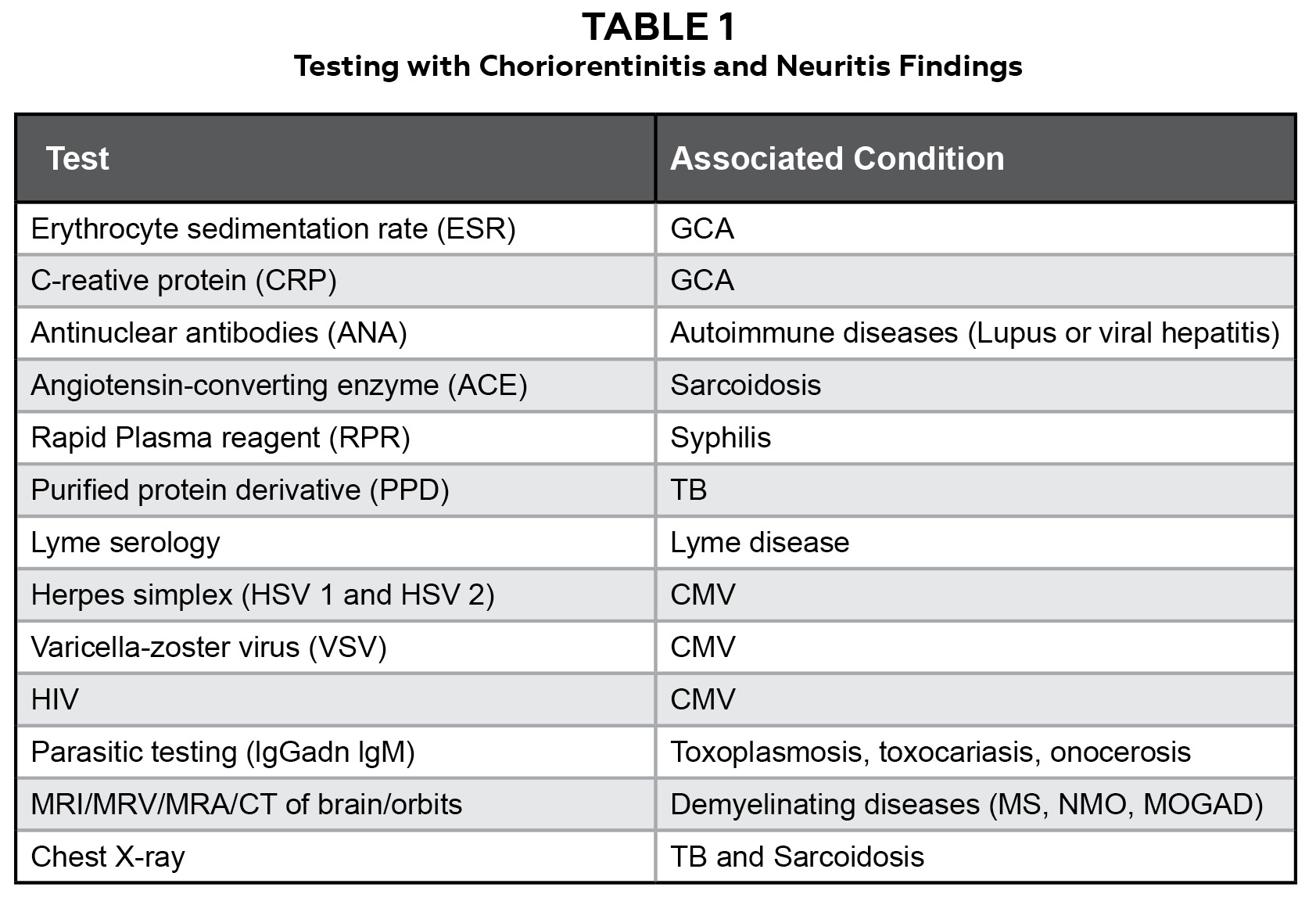
Table 1.51,52 Testing to be considered when attempting to differentiate syphilis from other underlying conditions that cause similar posterior segment findings. (GCA: Giant Cell Arteritis, TB: Tuberculosis, CMV: Cytomegalovirus, MS: Multiple Sclerosis, NMO: Neuromyelitis Optica, MOGAD: Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease). Click to enlarge
As with the presenting case, many of the patient’s ocular signs and symptoms could point to any of the above differentials. However, there were presenting and evolving findings pointing to the possibility of syphilis. For example, diabetic retinopathy could have been high on the differential list in this case, especially with the appearance of the vitreous hemorrhage. The unilateral appearance and sudden onset of his symptoms as well as his well-controlled blood sugars made this differential unlikely. Upon reviewing the b-scan (Figure 2), although a large vitreous opacity is observed, the retina itself was intact, therefore the likelihood of a retinal detachment was low. White dot syndromes can be ruled out in this patient due to the patient age and sex. While white dot syndromes present with symptoms of photopsia, blurred vision and involve the optic nerve, they also tend to affect young, healthy females. Per the OCT testing of the optic nerves and fovea (Figures 4-9) and fundus photos (Figures 1, 2 and 7), retinitis, vasculitis and optic nerve conditions associated with inflammatory or infectious conditions were highly suspected differentials, as well as optic neuritis and neuropathies. Therefore, proper blood tests, imaging and further case history questioning helped in differentiating likely diagnoses and confirming syphilis. Suggested testing can be found in Table 1.
Diagnosing Ocular Syphilis
Due to the diverse ocular presentations of syphilis, it can be difficult to diagnose. There are limited distinct clinical presentations, therefore it should always be included in the list of differential diagnoses when patients present with any of the following:
-
- Sexual activity and previous STI diagnosis: It is important to ask in the case history the patient’s sexual preference and past/recent sexual partners. Previous STI diagnoses can help determine the risk factor for syphilis, especially patients that have HIV/AIDs and/or a previous diagnosis and treatment for syphilis.
- Illicit drug use history: A case history inquiring about illicit drug use is pertinent, especially intravenous drug use which can help in determining risks for other infectious disease, such as HIV.
- Uveitis (anterior, intermediate and/or posterior): It is the most common manifestation of ocular syphilis.
- Patients undergoing treatment for other ocular infections or inflammatory conditions without resolution.
Further case history questioning can be a great way to help rule out other conditions mascaraed as syphilis. This case highlights the omission of pertinent sexual history, including sexual orientation and activity, during the initial case history. Inclusion of this information may have elevated syphilis as a primary diagnostic consideration earlier in the evaluation. Inquiring as mentioned above about IV drug use, sexual history/orientation and previous or current STIs is a great start, but further questioning regarding family history to rule out conditions like sickle cell, TB, diabetes, lung issues or neurological issues should be addressed. Obtaining a thorough environmental history is also essential, including inquiry about prior residence outside the country, exposure to animals (such as birds, cats or dogs), and consumption of raw or unpasteurized foods or beverages. Additionally, it is important to elicit any history of previous inflammatory or infectious conditions, such as lupus, sarcoidosis, Crohn’s disease, ulcerative colitis, Lyme disease, herpes zoster or herpes simplex. General systemic review is also warranted, including questions regarding recent overall health status and the presence of symptoms such as fever, unexplained weight loss, malaise, headache, recurrent infections, cough or dyspnea.
To further expand on case history questions to determine proper referrals or testing, it can be helpful to use a questionnaire, such as the Massachusetts Eye Research and Surgery Institution’s Ocular Inflammatory Disease Review of Systems Questionnaire that can be administered in the office. This questionnaire would have been a great tool for the optometrist in this teaching case to use in developing a proper diagnosis for the patient.
Appropriate ophthalmic exam testing when ocular syphilis is suspected (none of these tests are diagnostic for syphilis)
-
- Color fundus photography or ultra-wide field retinal imaging for general observation of the optic nerve, retinal vasculature, macula and retina (posterior pole to the periphery). In the case presented, syphilis related posterior segment findings can be seen in Figures 1, 2 and 7.
- Fundus autofluorescence photos (FAF), best with ultra-wide field cameras, shows greater extent of retinal involvement, specifically the RPE. Unfortunately, FAF was not performed in the presenting case. It would have likely outlined ASPPC, highlighting hyperautofluorescence with placoid lesions and RPE disruption.32
- Spectral domain optical coherence tomography (SD-OCT) is a diagnostic tool to observe disorders of the optic nerve, vitreous, retinal layers and the choroid. Specifically, allowing observation of the ellipsoid layer, RPE and the choroid when evaluating for syphilis involvement as seen in Figures 4-6, 8-9.
- Fluorescein angiography (FA) is utilized to evaluate retinal and choroidal circulation, with particular attention to vascular integrity and the function of the blood–retina barrier. In ocular syphilis, retinal vasculitis typically manifests as vascular leakage; optic neuritis presents with optic disc leakage; and chorioretinitis is characterized by early hypofluorescence followed by late hyperfluorescence.33 The patient’s FA presented in this case, demonstrated severe perfusion delay in the left eye with poor filling of the superior-temporal artery with noted plaques indicating retinal ischemia. An FA would also be used to monitor for the development of retinal necrosis.
Serological Testing
Serological testing remains the gold standard for diagnosing or ruling out syphilis. This testing can be ordered by the patient’s primary care doctor, an ophthalmologist, an infectious disease doctor, neuro-ophthalmologist/neurologist or an emergency medical provider. If an optometrist has lab privileges, they can order this testing, but positive testing would require a referral to an infectious disease provider for proper management. A biopsy of a lesion is the most definitive way to diagnose early syphilis, using polymerase chain reaction tests with darkfield microscopy.20 However, darkfield microscopy is hardly used due to is lack of availability in most clinical settings and the need for a lab to have the specific microscope and training for this specific test.34 Therefore, serological testing using non-treponemal test and a treponemal test is often done to diagnose syphilis.20,22,25,35 Both the serological testing and biopsy detect the presence of Treponema pallidum. Non-treponemal tests include Venereal Disease Research Laboratory (VDRL) and RPR. Both tests detect antibodies against the membrane phospholipids and are simple, rapid and inexpensive to obtain.20 Although they are not specific to detecting syphilis, they are good indicators of the disease activity for early syphilis, becoming positive within 1-3 weeks after the appearance of a primary lesion.20 The VDRL test is positive in 99% of patients with secondary syphilis, however in later stages of the disease, its sensitivity decreases and only about 70% of patients with tertiary syphilis test positive.16 VDRL stereological testing has a higher sensitivity in latent stages and CSF VDRL testing is better in detecting neurosyphilis.36 VDRL and RPR titers will decrease once treatment is administered and is determined successful when titers are non-reactive. However, it is important that only the VDRL or the RPR, not both, be used in diagnosing and monitoring progress of treatment because the quantitative results from the two tests are not directly comparable. In contrast, treponemal testing detects the antibodies that are specific for syphilis and will remain positive for life, confirming the diagnosis but not used to determine responses to treatment.20,23,25 Therefore, treponemal testing is highly specific for T. Pallidum and includes enzyme immunoassay (EIA), T. Pallidum hemagglutination tests (TP-HA or TP-PA), and the most commonly used fluorescent treponemal antibody absorption test (FTA-ABS). The FTA-ABS test is highly specific for syphilis but can show false positive results in patients with rheumatoid arthritis, biliary cirrhosis, systemic lupus erythematosus, hepatitis, HIV, infectious mononucleosis, rickettsial disease, scarlet fever and in pregnancy.16,37
Serological testing of both non-treponemal and treponemal tests need to be performed to increase the sensitivity and specificity for the diagnosis of syphilis. The CDC recommends using either one or both of the following algorithms when testing for syphilis depending on the test volume, laboratory resources and patient populations:36
- Traditional screening:36 VDRL/RPR as the initial screening test, followed by treponemal testing, such as the FTA-ABS if the screening test is found positive (Chart 1). The advantage of using this algorithm is that it may be more widely available. Disadvantages in using the traditional screening is it may be less sensitive in finding earlier or late latent syphilis.38
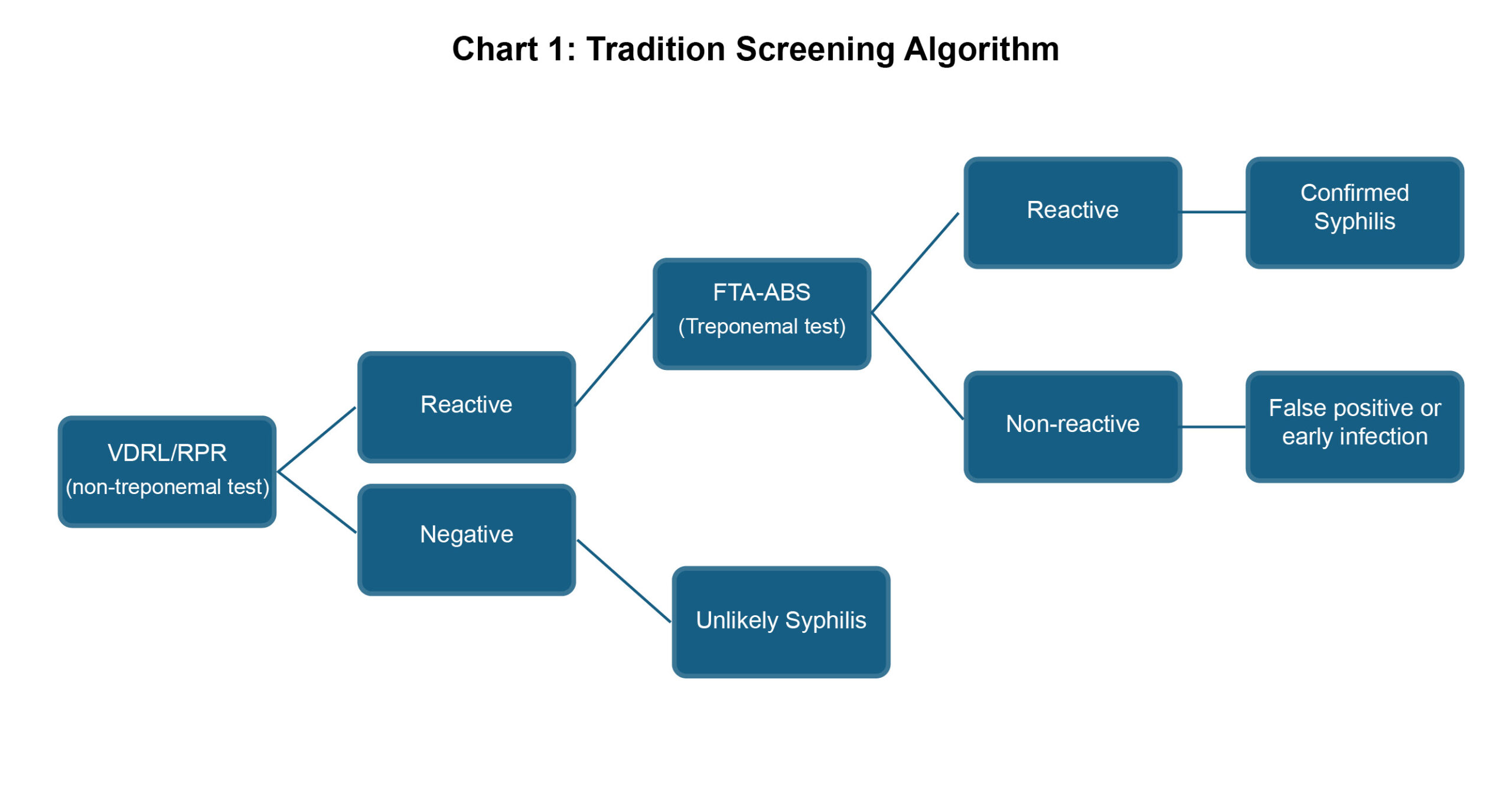
Chart 1. Flow chart of traditional screening algorithm for confirming the diagnosis of syphilis. Click to enlarge
- Reverse-Sequence screening(36): A treponemal specific immunoassay, such as the EIA or CIA as initial screening test, followed by a non-treponemal titer VDRL/RPR test if the EIA or CIA is positive. If the VDRL/RPR are non-reactive, then a treponemal test, such as the FTA-ABS is performed for confirmation (Chart 2). The advantage of this algorithm has a quicker turnaround for test results and is more sensitive in detecting early and latent syphilis. The disadvantage is that it could produce more false positives in populations with lower prevalence of syphilis(38).
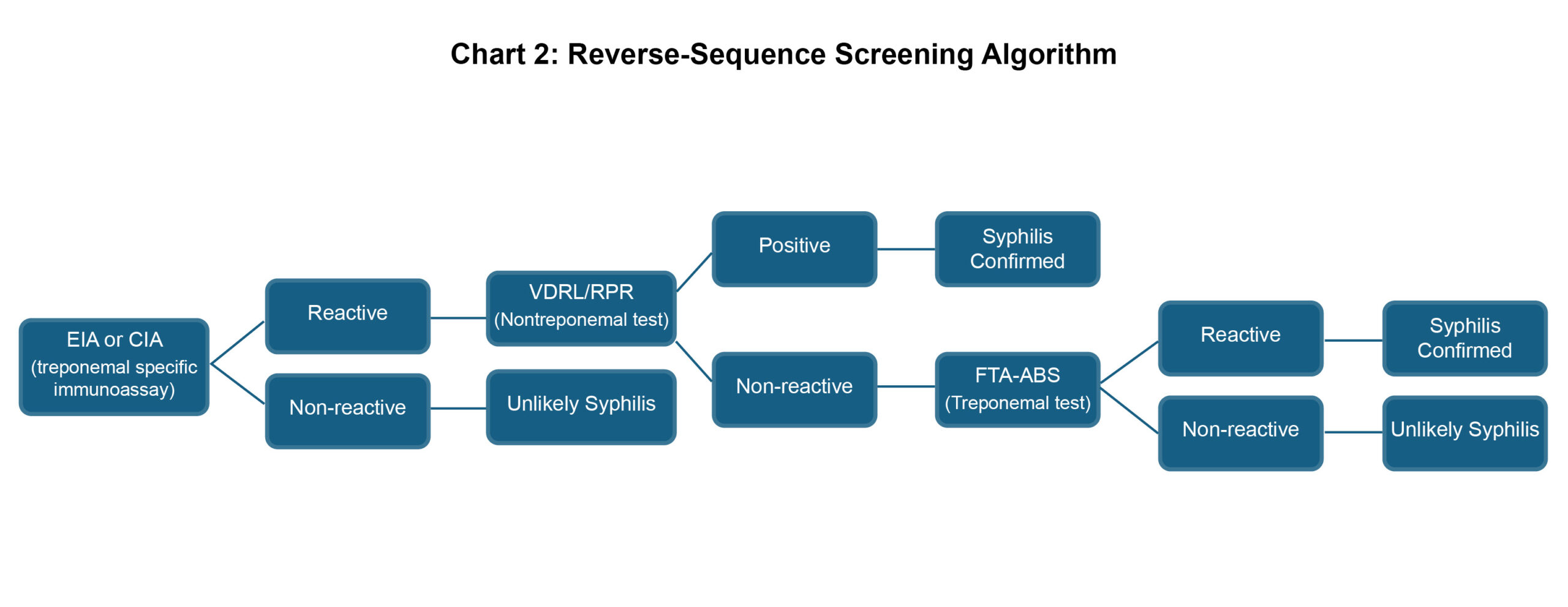
Chart 2. Flow chart of reverse-sequence screening algorithm for confirming the diagnosis of syphilis. Click to enlarge
If a patient is found to be positive for syphilis and has ocular manifestations, cerebral spinal fluid should be analyzed, with VDRL and FTA-ABS testing, for a true diagnosis of neurosyphilis. In the presented case, a lumbar puncture was ordered, but the patient refused to undergo the testing. When this diagnosis is confirmed, it is important for an infectious disease doctor to be incorporated into the patient’s care to initiate a proper treatment protocol. At the time of a syphilis diagnosis, all patients should undergo HIV testing due to the strong association between the two infections. In this case, the patient was appropriately tested for HIV, and the result was negative. Co-infection can also lead to an increased risk of developing neurosyphilis due to its increased association with posterior uveitis due to syphilis.39 There is a higher correlation for co-infection in HIV patients that had CD4 counts greater than 200 cells/mm3 and higher titers RPR/VDRL.39 This is believed to result from syphilis remaining undetected due to the false-negative prozone phenomenon, in which non-treponemal tests yield negative results despite active infection. Consequently, without timely initiation of systemic penicillin therapy, the disease may progress to later or latent stages.39 That is why in cases with co-infection, the reverse screening algorithm can be better at catching false negatives. Although it is unclear why this association exists, it is believed that HIV causes the natural history of treponemal infection to change and therefore is not detectable.39
Treatment
Once the diagnosis of ocular syphilis has been established, the patient is subsequently treated as having neurosyphilis, a subset of syphilis involving neuronal tissue that can present in any stage of syphilis. There are treatment protocols for each stage of the disease per the CDC to decrease the risk of the infection progressing to a higher staging level:
-
- Primary and secondary syphilis: Treatment with a single dose of intramuscular (IM) penicillin G benzathine or procaine penicillin (non-generic) and probenecid (a treatment to inhibit renal drug excretion), as well as 1 g of either penicillin orally 4 times/day for 14 days. For those allergic to penicillin, doxycycline 100 mg orally twice a day for 14 days or ceftriaxone 1 to 2 g IM or intravenously (IV) daily for 10-14 days or tetracycline 100 mg orally 4 times/day for 14 days.16,40
- Latent and tertiary syphilis (including neurosyphilis and ocular syphilis): Treatment includes aqueous crystalline penicillin G 3 to 4 million units IV every 4 hours for 10-14 days or benzathine penicillin G 2.4 million units IM weekly for 3 weeks. Ceftriaxone and azithromycin have been used as well.16,26
- For pregnant people, penicillin is the only documented treatment that has established efficacy for treating syphilis. For those that are allergic, they are desensitized first and then treated.16
- Adjunct Treatment with Corticosteroids
- Jarisch-Herxheimer reaction can occur in the first 24 hours of initial treatment with IV penicillin due to a hypersensitivity reaction to treponemal antigens released as the spirochetes are attacked.3,23 This reaction may also lead to an increase in severity of ocular manifestations of syphilis.41 Therefore, it is recommended that IV methylprednisolone be used before initiation of IV penicillin and continued for the next 48 hours.41
- Oral corticosteroids would be introduced after antibiotic treatment to reduce intraocular inflammation for the treatment of posterior uveitis, vitritis, scleritis and optic neuritis.41
- The use of periocular and intraocular steroid injections has been correlated to treatment failure due to the risk of bacterial or virus growth, activating dormant infections that could lead to CMV retinitis.3,42-44
Prognosis
The prognosis of ocular syphilis can be good when the disease is diagnosed early and treated promptly. Some studies have shown an over 90% improvement in visual acuity to 20/40 or better, while others have shown a 30-40% visual acuity loss of 20/50 or worse despite treatment.3,13,39,41,45-47 Prompt systemic treatment with penicillin within 1 month after the onset of ocular manifestations implies the best chance for favorable visual outcomes, especially in those with concurrent HIV.3,48,49 Permanent vision loss occurs due to structural damage to the retina, especially the macula and the optic nerve. Quality of life may be decreased based on a diagnosis of ocular syphilis, not only due to the possibility of irreversible vision loss, but other issues, such as time away from a job and family, obligations to receive care and the mental health and social stigma of having a known STI.
Due to the complexity of diagnosing, treating and managing ocular syphilis, it is important to have multiple healthcare providers involved in the patient’s care. Inter-professional communication between them is vital to ensure a proper diagnosis in addition to appropriate and timely treatment and management. The healthcare providers involved in this care often include an optometrist, ophthalmologist, primary care physician, neurologist/neuro-ophthalmologist and an infectious disease specialist. Each provider has an important role in continuing care with the patient during and after treatment to ensure the best systemic and ocular outcome. The ophthalmologist, often a retinal specialist, will monitor the posterior findings, ensuring that inflammation is improving and necrosis doesn’t develop. They would also treat any residual ocular complications not resolved after IV penicillin G treatment. For example, an unresolving vitreous hemorrhage would be treated with an Anti-VEGF injection, or if posterior inflammation was persistent, oral steroids would be started. As mentioned above, intra-ocular injections of steroids for the treatment of persistent macular edema should be cautioned until effective systemic penicillin treatment has been initiated and a response in decreased titers is established. A neuro-ophthalmologist or neurologist will continue to monitor the optic nerve and to ensure no other neurological conditions and symptoms arise, such as, meningeal/meningovascular involvement, paresis or mood/personality/memory changes.50 The infectious disease specialist will provide treatment and monitor titers to ensure that the treatment is working, as well as managing co-existing infections like herpes and HIV that are common with a syphilis diagnosis. Once the infection resolves, it’s important for the PCP to continue appropriate long-term follow-ups to ensure no new symptoms of infection arise by testing regularly and evaluating the skin in high prevalence areas where the infection can arise.
Optometrists can play an important role in identifying patients at risk for syphilis, by identifying rashes on hands, observing or asking about chancres and administering the MERSI questionnaire for patients. Optometrists also are necessary during and after treatment of syphilis, continuing to provide regular comprehensive eye exams and communicating with other co-managing providers about any new ocular changes or increased lifestyle activity (i.e. New sexual partners, IV drug use or exposure to syphilis, or other STI, especially HIV) that could pose an increase in another infection. Also, if visual outcomes are not ideal, they can provide patients with glasses, low vision devices and services in hopes of optimizing the patient’s vision and quality of life.
Conclusion
In conclusion, ocular syphilis, especially with posterior segment involvement, can lead to significant visual impairment if not diagnosed and treated promptly. Optometrists play an important role in diagnosing the risks for syphilis when it presents with posterior uveitis, vitritis, vitreous hemorrhage and/or optic neuritis, which are also seen with many other ocular conditions. This teaching case represents the importance an optometrist can have in identifying the risks for syphilis when patients present with similar ocular findings. In this case, although the optometrist considered appropriate differential diagnoses and made a suitable referral, a more comprehensive case history, specifically related to sexual activity and orientation, as well as the application of the MERSI questionnaire might have facilitated a more accurate and quicker diagnosis. Ultimately, serological testing is paramount to confirm syphilis, this case demonstrated the importance of other appropriate testing to rule out other mimicking conditions. Once syphilis is confirmed, interdisciplinary collaboration is vital to ensure timely treatment is initiated in hopes of achieving ideal patient outcomes.
References
- Centers for Disease Control and Prevention. Sexually transmitted disease surveillance, 2022 overview [Internet]. Atlanta, GA: Centers for Disease Control and Prevention; c2024 [cited 2024 Jan 31]. Available from: https://stacks.cdc.gov/view/cdc/
- World Health Organization. Prevalence and incidence of selected sexually transmitted infections, Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis: methods and results used by WHO to generate 2005 estimates. Geneva: World Health Organization; 2011.
- Furtado JM, Simões M, Vasconcelos-Santos D, et al. Ocular syphilis. Surv Ophthalmol. 2022 Mar-Apr;67(2):440–62. DOI: 10.1016/j.survophthal.2021.06.003
- Hayreh SS. Ischemic optic neuropathy. Int Ophthalmol. 1978 Sep;1(1):9–18. DOI: 10.1007/BF00133273
- Bennett JL. Optic neuritis. Continuum (Minneap Minn). 2019 Oct;25(5):1236–64. DOI: 10.1212/CON.0000000000000768
- Jena S, Tripathy K. Vitreous hemorrhage [Internet]. Treasure Island (FL): StatPearls Publishing; c2025 [cited 2025 May 10]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559131/
- Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005 Sep;140(3):509–16. DOI: 10.1016/j.ajo.2005.03.057
- Standardization of Uveitis Nomenclature Working Group. Development of classification criteria for the uveitides. Am J Ophthalmol. 2021 Aug;228:96–105. DOI: 10.1016/j.ajo.2021.03.061
- Geetha R, Tripathy K. Chorioretinitis [Internet]. Treasure Island (FL): StatPearls Publishing; c2025 [cited 2025 May 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551705/
- Touhami S, Leclercq M, Stanescu-Segall D, Touitou V, Bodaghi B. Differential diagnosis of vitritis in adult patients. Ocul Immunol Inflamm. 2021 May 19;29(4):786–95. DOI: 10.1080/09273948.2021.1898001
- Smith JR. Uveitis. In: Ehlers JP, Shah CP, editors. The Wills Eye Manual: Office and Emergency Room Diagnosis and Treatment of Eye Disease. 5th ed. Baltimore (MD): Lippincott Williams & Wilkins; 2008. pp. 308–309.
- Neurosyphilis, ocular syphilis, and otosyphilis [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; c2021 [cited 2024 Jan 31]. Available from: https://www.cdc.gov/std/treatment-guidelines/neurosyphilis.htm [updated URL].
- Furtado JM, Arantes TE, Nascimento H, et al. Clinical manifestations and ophthalmic outcomes of ocular syphilis at a time of re-emergence of the systemic infection. Sci Rep. 2018 Aug 13;8(1):12071. DOI: 10.1038/s41598-018-30559-7
- Berkenstock M, Mopuru R, Thorne J, Scott AW. Analysis of new cases of uveitis at academic and community settings. Br J Ophthalmol. 2021 Jun;105(6):779–82. DOI: 10.1136/bjophthalmol-2020-316651
- Nham A, Holly T, Flores J, Kern D, Tabidze I. Notes from the field: neurosyphilis, ocular syphilis, and otic syphilis — Chicago, January–October 2023. MMWR Morb Mortal Wkly Rep. 2025 Mar 13;74(8):140–3. DOI: 10.15585/mmwr.mm7408a3
- Koundanya VV, Tripathy K. Syphilis ocular manifestations [Internet]. Treasure Island (FL): StatPearls Publishing; c2024 [cited 2025 Feb 11]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558957/
- Lafond RE, Lukehart SA. Biological basis for syphilis. Clin Microbiol Rev. 2006 Jan;19(1):29–49. DOI: 10.1128/CMR.19.1.29-49.2006
- Hook EW 3rd, Marra CM. Acquired syphilis in adults. N Engl J Med. 1992 Apr 16;326(16):1060–9. DOI: 10.1056/NEJM199204163261606
- Garnett GP, Aral SO, Hoyle DV, Cates W Jr, Anderson RM. The natural history of syphilis: implications for the transmission dynamics and control of infection. Sex Transm Dis. 1997 Apr;24(4):185–200. DOI: 10.1097/00007435-199704000-00002
- Tsan GL, Claiborne RT. Ocular syphilis. Clin Exp Optom. 2021 Sep;104(7):756–9. DOI: 10.1080/08164622.2021.1906848
- Anderson J, Mindel A, Tovey SJ, Williams P. Primary and secondary syphilis, 20 years’ experience. 3: diagnosis, treatment, and follow up. Genitourin Med. 1989 Aug;65(4):239–43. DOI: 10.1136/sti.65.4.239
- Workowski KA. Centers for Disease Control and Prevention sexually transmitted diseases treatment guidelines. Clin Infect Dis. 2015 Dec 15;61 Suppl 8:S759–62. DOI: 10.1093/cid/civ771
- Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015 Jun 5;64(RR-03):1–137.
- Ghanem KG, Ram S, Rice PA. The modern epidemic of syphilis. N Engl J Med. 2020 Feb 27;382(9):845–54. DOI: 10.1056/NEJMra1901593
- Kiss S, Damico FM, Young LH. Ocular manifestations and treatment of syphilis. Semin Ophthalmol. 2005 Jul-Sep;20(3):161–7. DOI: 10.1080/08820530500232092
- Clement ME, Okeke NL, Hicks CB. Treatment of syphilis: a systematic review. JAMA. 2014 Nov 12;312(18):1905–17. DOI: 10.1001/jama.2014.13259
- Gass JD, Braunstein RA, Chenoweth RG. Acute syphilitic posterior placoid chorioretinitis. Ophthalmology. 1990 Oct;97(10):1288–97. DOI: 10.1016/S0161-6420(90)32418-1
- Fu EX, Geraets RL, Dodds EM, et al. Superficial retinal precipitates in patients with syphilitic retinitis. Retina. 2010 Jul-Aug;30(7):1135–43. DOI: 10.1097/IAE.0b013e3181cdf3ae
- Agarwal A, Rubsam A, Zur Bonsen L, Pichi F, Neri P, Pleyer U. A comprehensive update on retinal vasculitis: etiologies, manifestations and treatments. J Clin Med. 2022 Apr 30;11(9):2525. DOI: 10.3390/jcm11092525
- Marmor MF. Control of subretinal fluid: experimental and clinical studies. Eye (Lond). 1990;4(Pt 2):340–4. DOI: 10.1038/eye.1990.46
- Kuo A, Ziaee SM, Hosseini H, et al. The great imitator: ocular syphilis presenting as posterior uveitis. Am J Case Rep. 2015 Jul 7;16:434–7. DOI: 10.12659/AJCR.893907
- Neri P, Pichi F. Acute syphilitic posterior placoid chorioretinitis: when the great mimicker cannot pretend any more. J Ophthalmic Inflamm Infect. 2022 Feb 22;12(1):9. DOI: 10.1186/s12348-022-00286-2
- Geetha R, Tripathy K. Chorioretinitis [Internet]. Treasure Island (FL): StatPearls Publishing; c2024 [cited 2025 Mar 2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551705/
- Pierce EF, Katz KA. Darkfield microscopy for point-of-care syphilis diagnosis. MLO Med Lab Obs. 2011;43(1):30–1.
- Davis JL. Ocular syphilis. Curr Opin Ophthalmol. 2014 Nov;25(6):513–8. DOI: 10.1097/ICU.0000000000000099
- Papp JR, Park IU, Fakile Y, Pereira L, Pillay A, Bolan GA. CDC laboratory recommendations for syphilis testing, United States, 2024. MMWR Recomm Rep. 2024 Feb 8;73(1):1–32. DOI: 10.15585/mmwr.rr7301a1
- Henao-Martinez AF, Johnson SC. Diagnostic tests for syphilis: new tests and new algorithms. Neurol Clin Pract. 2014 Apr;4(2):114–22. DOI: 10.1212/01.CPJ.0000435752.17621.48
- Binnicker MJ, Jespersen DJ, Rollins LO. Direct comparison of the traditional and reverse syphilis screening algorithms in a population with a low prevalence of syphilis. J Clin Microbiol. 2012 Jan;50(1):148–50. DOI: 10.1128/JCM.05636-11
- Tucker JD, Li JZ, Robbins GK, et al. Ocular syphilis among HIV-infected patients: a systematic analysis of the literature. Sex Transm Infect. 2011 Feb;87(1):4–8. DOI: 10.1136/sti.2010.043042
- Hook EW 3rd, Roddy RE, Handsfield HH. Ceftriaxone therapy for incubating and early syphilis. J Infect Dis. 1988 Oct;158(4):881–4. DOI: 10.1093/infdis/158.4.881
- Bollemeijer JG, Wieringa WG, Missotten TO, et al. Clinical manifestations and outcome of syphilitic uveitis. Invest Ophthalmol Vis Sci. 2016 Feb;57(2):404–11. DOI: 10.1167/iovs.15-17906
- Hoogewoud F, Frumholtz L, Loubet P, et al. Prognostic factors in syphilitic uveitis. Ophthalmology. 2017 Dec;124(12):1808–16. DOI: 10.1016/j.ophtha.2017.06.003
- Saidel MA, Berreen J, Margolis TP. Cytomegalovirus retinitis after intravitreous triamcinolone in an immunocompetent patient. Am J Ophthalmol. 2005 Dec;140(6):1141–3. DOI: 10.1016/j.ajo.2005.06.058
- van Kooij B, Rothova A, de Vries P. The pros and cons of intravitreal triamcinolone injections for uveitis and inflammatory cystoid macular edema. Ocul Immunol Inflamm. 2006 Apr;14(2):73–85. DOI: 10.1080/09273940500545684
- Mathew RG, Goh BT, Westcott MC. British Ocular Syphilis Study (BOSS): 2-year national surveillance study of intraocular inflammation secondary to ocular syphilis. Invest Ophthalmol Vis Sci. 2014 Jun 12;55(8):5394–400. DOI: 10.1167/iovs.14-14559
- Moradi A, Salek S, Daniel E, et al. Clinical features and incidence rates of ocular complications in patients with ocular syphilis. Am J Ophthalmol. 2015 Feb;159(2):334–43.e1. DOI: 10.1016/j.ajo.2014.10.030
- Fonollosa A, Martinez-Indart L, Artaraz J, et al. Clinical manifestations and outcomes of syphilis-associated uveitis in Northern Spain. Ocul Immunol Inflamm. 2016;24(2):147–52. DOI: 10.3109/09273948.2014.943349
- Tsuboi M, Nishijima T, Yashiro S, et al. Prognosis of ocular syphilis in patients infected with HIV in the antiretroviral therapy era. Sex Transm Infect. 2016 Dec;92(8):605–10. DOI: 10.1136/sextrans-2016-052568
- Zhu J, Jiang Y, Shi Y, Zheng B, Xu Z, Jia W. Clinical manifestations and treatment outcomes of syphilitic uveitis in HIV-negative patients in China. Medicine (Baltimore). 2017 Oct;96(43):e8376. DOI: 10.1097/MD.0000000000008376
- Ha T, Tadi P, Leslie SW, Dubensky L. Neurosyphilis [Internet]. Treasure Island (FL): StatPearls Publishing; c2025 [cited 2025 May 20]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK540979/
- Sudharshan S, Ganesh SK, Biswas J. Current approach in the diagnosis and management of posterior uveitis. Indian J Ophthalmol. 2010 Jan-Feb;58(1):29–43. DOI: 10.4103/0301-4738.58470
- Voss E, Raab P, Trebst C, Stangel M. Clinical approach to optic neuritis: pitfalls, red flags and differential diagnosis. Ther Adv Neurol Disord. 2011 Mar;4(2):123–34. DOI: 10.1177/1756285611398702

