
PEER REVIEWED
Scleritis
Jennifer Reilly OD, MS, FAAO
Abstract
Scleritis is a rare ocular condition involving inflammation of the sclera and a significant degree of associated pain. Underlying inflammatory systemic disease is a common cause of scleritis, although it may be idiopathic or due to infectious etiologies as well. Proper disease management is paramount as the condition can be vision threatening. In addition, management can be complex and often requires a team of healthcare providers working together to manage the patient. This case report explores an instance of scleritis while highlighting important teaching elements throughout the diagnosis and management of the condition.
Keywords
Background
Scleritis is a rare but critical ocular condition that consists of painful inflammation of the sclera.1 The condition often presents as a painful red eye that may be unilateral or bilateral in nature.2 Scleritis is a significant condition because it can be vision threatening;1,3,4 therefore, proper diagnosis and management are crucial. Scleritis may be caused by underlying inflammatory systemic disease or an infectious etiology and thus a proper workup to determine the underlying cause of the condition is critical for successful disease management. Scleritis management is often complex and involves a team of healthcare providers. Optometrists can play a key role in the healthcare team managing a case of scleritis, particularly as they may be the first providers to see and identify the condition. The following clinical case discussion is directed toward third- and fourth-year optometry students, optometry residents and practicing doctors.
Case Description
Optometry, Initial Presentation, Visit 1
A 43-year-old White male presented to the optometry department for a problem specific eye exam. His chief concern was a bilateral red eye with a deep pain in and around both eyes for 4-6 weeks. Signs and symptoms were greater in the left eye than the right eye. He rated the pain a 10 out of 10 with 10 being the worst pain imaginable in both eyes. He was mildly light sensitive but denied double vision, discharge or other associated symptoms. The patient reported that he was previously seen at another eye clinic about 4 weeks prior and again 2 weeks ago but had not experienced any relief of his symptoms despite those visits and compliance with recommended treatment. The medical records from the external eye clinic were requested, received and reviewed during the exam.
The patient’s ocular history was significant for myopia, corrected with spectacles and soft contact lenses. The external records indicated that he had a “significant history of soft contact lens overwear and contact lens associated red eye (CLARE),” for which he had been treated with antibiotic-steroid combination eye drops on multiple occasions in the past and was a known steroid responder when using such drops. He also had a history of chronic mild dry eye for which he used artificial tears twice a day in both eyes and stable lattice retinal degeneration in both eyes. The notes indicated that the patient was last seen 2 weeks ago at the external clinic for a follow up visit as he had been diagnosed with CLARE in both eyes and was to discontinue soft contact lens wear until the condition resolved. When the discontinued use of soft contact lenses did not provide relief, he presented to our eye clinic.
The patient’s medical history was significant for hypertension, lower back pain and joint pain which he attributed to a prior work injury. He had no history of concussion or traumatic brain injury (TBI). The patient’s hypertension was managed with lisinopril, and he took 200 mg of ibuprofen as needed for the lower back and joint pain. The patient’s father also had hypertension, but the family medical and ocular history were otherwise unremarkable. The patient was a former smoker and reported drinking alcohol socially with no recreational drug use.
At presentation, his visual acuities with habitual spectacle correction were 20/20 right, left, and both eyes at distance and near. Pupils and confrontation fields were unremarkable in both eyes. Extraocular muscle movements were smooth, accurate, full and extensive. However, the patient reported a “deep pain” in downgaze of both eyes, which was caused by the congestion and inflammation of the scleral shell where the extraocular muscles insert.
Anterior segment evaluation revealed mild capped Meibomian glands of both eyes. The conjunctiva, episclera and sclera presented a diffuse deep red injection worse in the left eye than the right eye. The left eye also had a mild conjunctival chemosis (Figures 1A and 1B). There were no visible nodules, areas of scleral whitening or capillary non-perfusion in either eye. The cornea had a few small scattered round scars in the periphery of both eyes, presumed to be old scarred subepithelial infiltrates (SEI) from past episodes of CLARE. There was mild pannus around the limbus in both eyes. There was no active dendrite or corneal ulcer in either eye. The anterior chamber was deep and quiet in the right eye, but had a mild cell and flare reaction in the left eye. The iris was flat and clear and the Van Herick angle estimation was 1:1 in both eyes. Intraocular pressures (IOP) by Goldmann Applanation Tonometry (GAT) were 15 mmHg in the right eye and 17 mmHg in left eye. The patient was dilated with 2 drops of tropicamide 1% in each eye. Of note, phenylephrine 2.5% was not available in the clinic on the day of presentation.

Figure 1A. Anterior segment photography of the right eye displaying conjunctival, episcleral and scleral injection. Click to enlarge
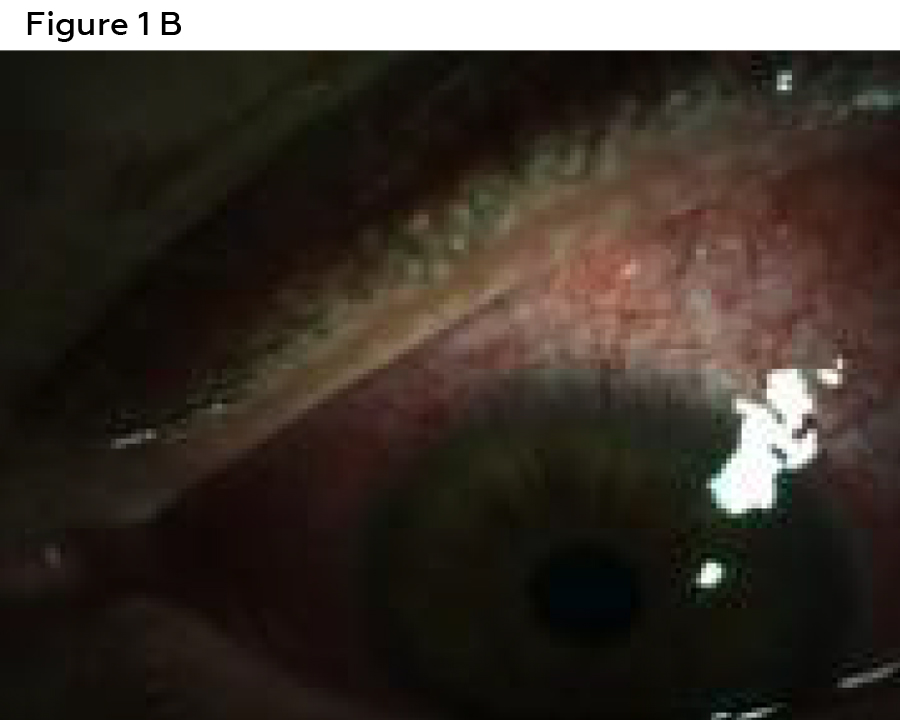
Figure 1B. Anterior segment photography of the eft eye (B) displaying conjunctival, episcleral and scleral injection. Click to enlarge
The dilated ocular health exam revealed a clear media without vitritis, vasculitis or retinitis. The macula was flat and clear in both eyes. The optic nerve head appeared healthy, well perfused and had a cup to disc ratio of 0.35/0.35 H/V in both eyes. There was lattice retinal degeneration inferiorly in both eyes, with no other significant peripheral retinal findings in either eye.
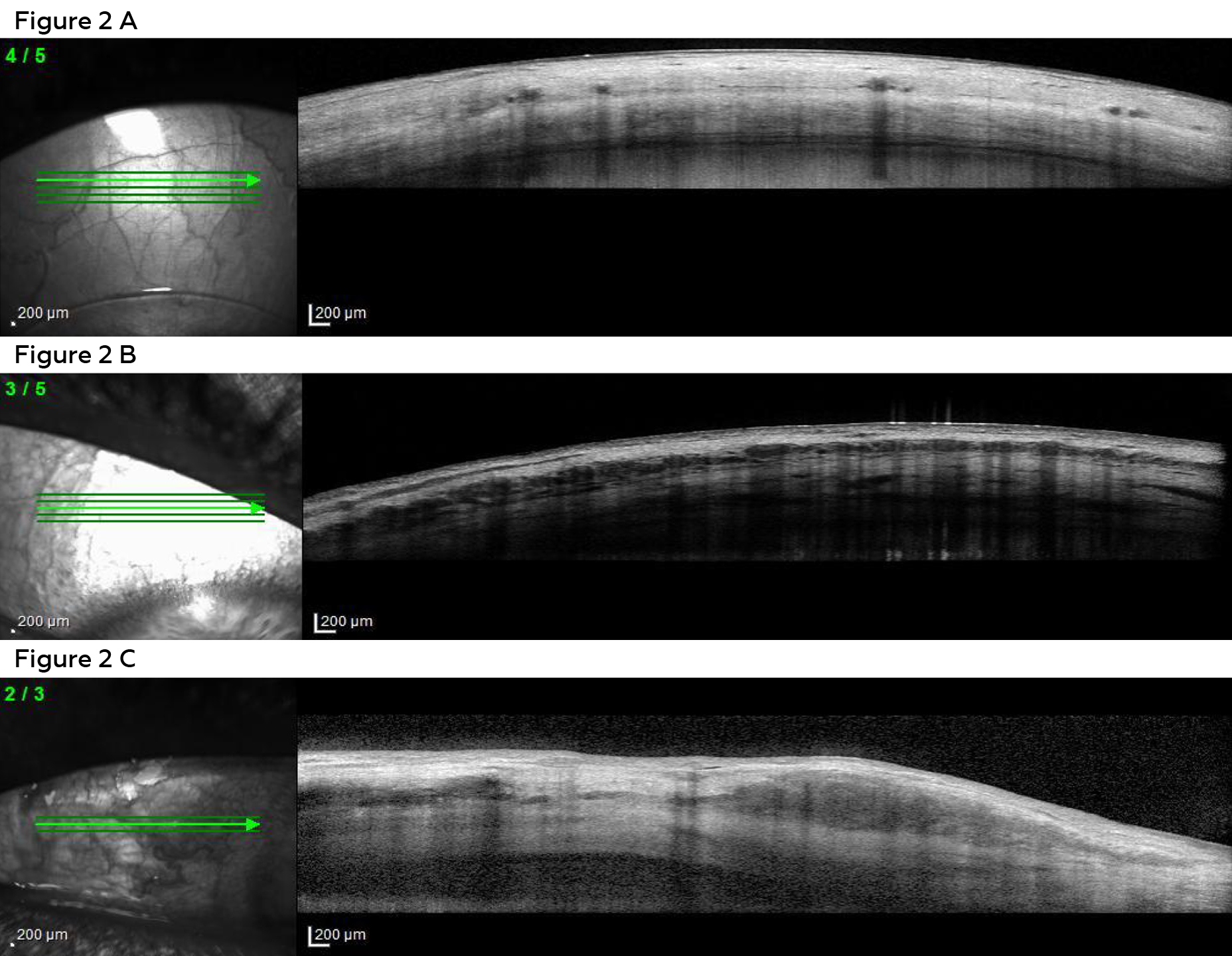
Figure 2. ASOCT images of (A) a normal conjunctiva, episclera and sclera and of our patient’s scleritis in the right eye (B) and left eye (C). The circular hypopigmented spaces with an underlying shadow are blood vessels. The horizontal lines of hypopigmented spaces between or within layers are edema. The deep delamination and edema is highly suggestive of scleritis in both eyes. Click to enlarge
Ancillary testing was performed the same day including anterior segment photography (Canon USA Inc.)a and anterior segment optical coherence tomography (ASOCT) (Heidelberg Engineering)b. The anterior segment photos showed diffuse moderate injection of both eyes (Figures 1A and 1B). The ASOCT line scans through the conjunctiva, episclera and sclera showed blood vessel dilation and edema of all layers (Figure 2).
The patient was diagnosed with presumed diffuse anterior non-necrotizing scleritis of both eyes and mild anterior uveitis of the left eye believed to be associated with the scleritis. The patient was extensively educated on the condition and was started on 400 mg of ibuprofen orally 4 times per day. A table with all prescribed medications over the course of the patient’s treatment can be found in Table 1. Ophthalmology was consulted to assist in management and determining the causative etiology of the suspected scleritis and the patient was scheduled with the uveitis clinic 2 days later. Assessments were also made to acknowledge the patient’s history of dry eye, CLARE with associated corneal remnant findings, prior steroid response, lattice retinal degeneration and refractive error. The patient was instructed to maintain discontinuation of soft contact lenses until the suspected scleritis was under control.
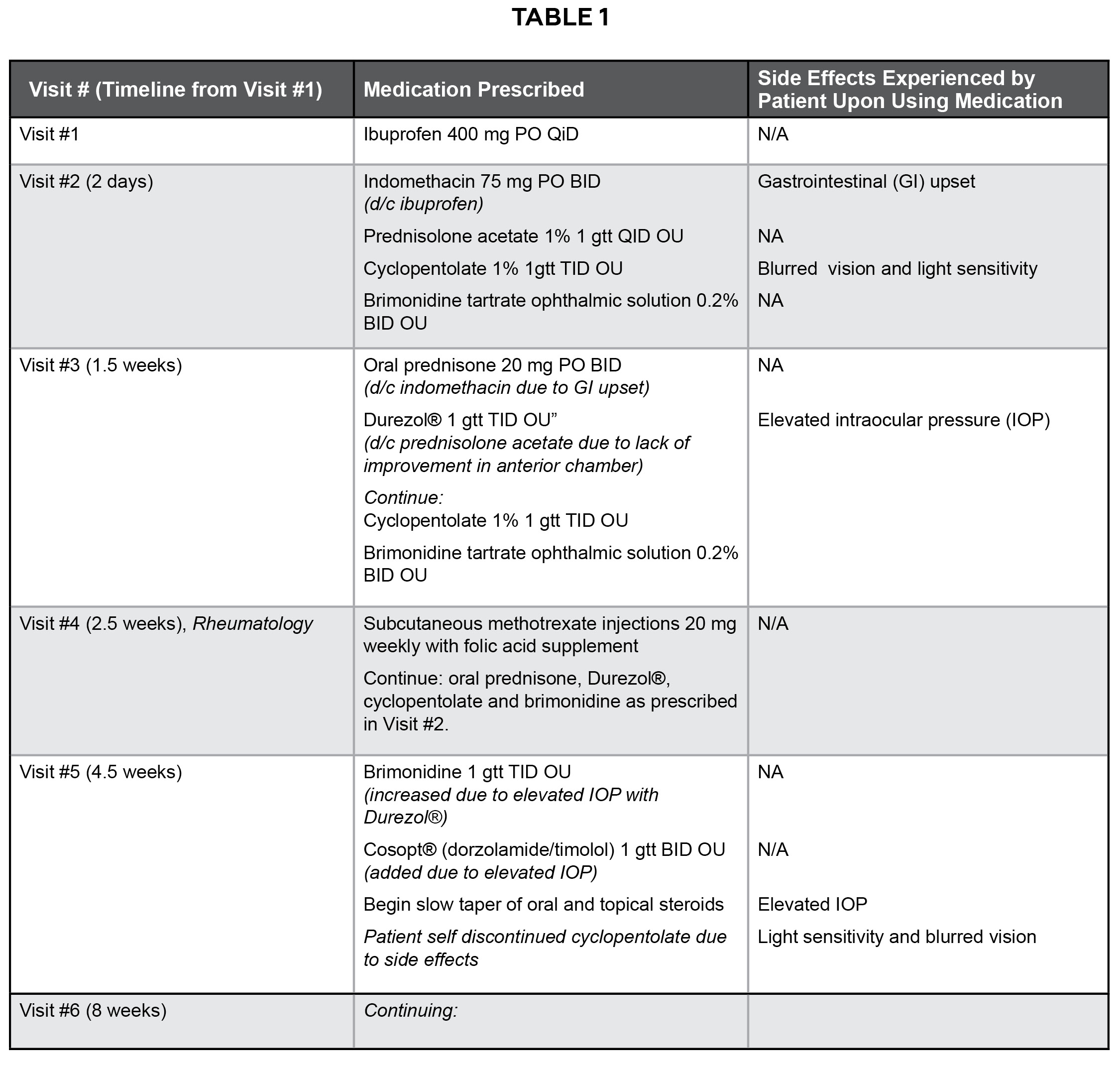
Table 1. Medications prescribed for the patient during the course of his treatment. Click to enlarge
Ophthalmology, Uveitis Clinic, Visit 2
At the ophthalmology consultation 2 days later, the patient’s presenting symptoms, visual acuity and entrance test findings remained unchanged from the prior visit. The anterior segment assessment was also unchanged with the exception of a mild anterior chamber reaction now noted in the right eye in addition to the left eye. IOP by GAT was 17 mmHg in each eye. The patient was dilated with 2 drops of tropicamide 1% in each eye. The dilated posterior segment exam was also unchanged from the previous visit.
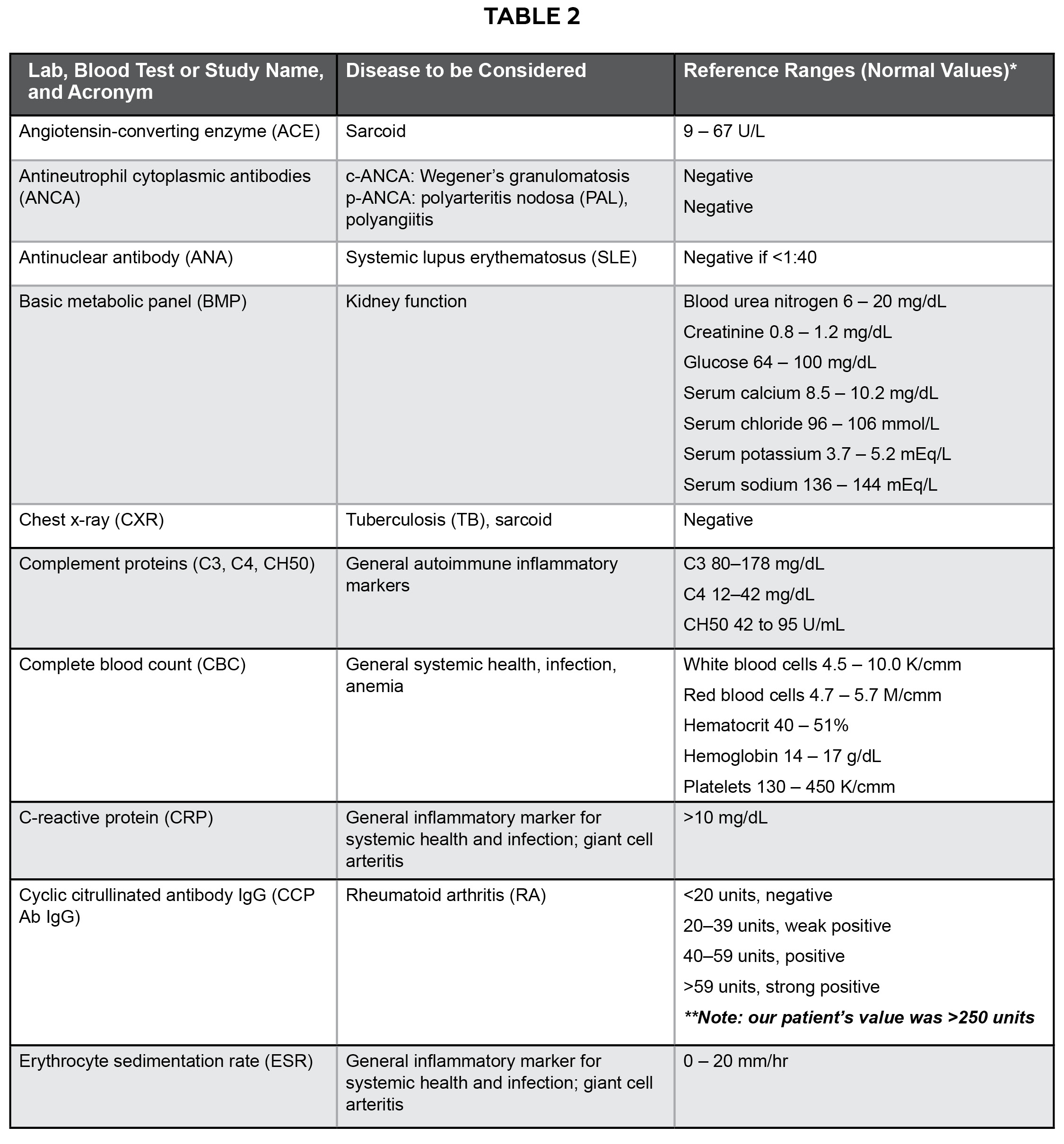
Table 2. Blood work, labs and imaging that are often or may be ordered in the presence of scleritis to rule out systemic etiology.12 *Reference ranges were provided by the laboratory with the blood work results. Reference ranges may vary slightly between laboratories. **The only positive findings that our patient had from ordered labs was CCP Ab IgG, which was >250 units compared to the reference ranges listed above. Click to enlarge
The ophthalmology clinic supported the presumed diagnosis of scleritis in both eyes and changed the oral nonsteroidal anti-inflammatory (NSAID) from ibuprofen 400 mg 4 times per day to indomethacin 75 mg orally 2 times per day. The patient was also started on Pred Forte® (prednisolone acetate 1% ophthalmic suspension) 4 times per day in both eyes in addition to cyclopentolate 3 times per day in both eyes for the anterior chamber reaction. Prophylactically, brimonidine tartrate ophthalmic solution 0.2% 2 times per day in both eyes was prescribed due to the patient’s history of being a steroid responder.
Blood work was ordered including rapid plasma reagin (RPR), fluorescent treponemal antibody-absorption (FTA-ABS), Lyme titers, rheumatoid factor (RF), cyclic citrullinated antibody (CCP Ab IgG), human leukocyte antigen B27 (HLA-B27), antinuclear antibody (ANA), erythrocyte sedimentation rate (ESR), c-reactive protein (CRP), basic metabolic panel (BMP), thyroid-stimulating hormone (TSH), complete blood count (CBC), angiotensin converting enzyme (ACE) and a chest x-ray (CXR). See Table 2 and discussion below for additional information on recommended blood work. The patient was referred to both rheumatology and dermatology for comprehensive evaluation and was directed to follow up with the ophthalmology clinic in 1 week.
Ophthalmology, Uveitis Clinic, Visit 3
At the 1 week follow-up visit to ophthalmology, the patient’s condition was essentially unchanged from the previous assessment. The patient experienced gastrointestinal (GI) upset due to the high dose oral NSAIDs prescribed, and thus was switched to oral steroids in order to treat the scleritis but avoid the GI symptoms. The labs and blood work were completed and all were negative or within normal ranges with the exception of CCP Ab IgG which came back at >250 units. The reference ranges for CCP Ab IgG were: <20-50 units is normal, and >59 units is considered a strong positive for rheumatoid arthritis (RA). Interestingly, the RF blood work came back negative.
Given the lack of improvement in the condition and GI symptoms, indomethacin was discontinued and oral prednisone 20 mg 2 times per day was initiated. In addition, the patient was switched from Pred Forte® 4 times per day, both eyes to Durezol® three times per day, both eyes. The patient was to continue cyclopentolate 3 times per day both eyes and brimonidine 2 times per day both eyes. The patient was directed to return to the ophthalmology clinic in 1-2 weeks for follow-up.
Rheumatology Consultation, Visit 4
About 2 weeks after the initial ophthalmology consultation the patient had their comprehensive rheumatology examination and was diagnosed with RA given their history of back and joint pain and the strong positive CCP Ab IgG lab results. The patient was instructed to begin subcutaneous methotrexate injections 20 mg weekly with folic acid supplement. The patient was instructed to return to rheumatology in 4 weeks for follow-up and continue with ophthalmology as directed. The dermatology consultation was canceled.
Ophthalmology, Uveitis Clinic, Visit 5
Two weeks after the rheumatology consultation, the patient returned to the ophthalmology clinic for follow-up. The patient’s signs and symptoms were improved, and he reported decreased eye pain, headaches and redness. At this visit, the patient was taking oral prednisone 20 mg orally 2 times per day, Durezol 3 times per day both eyes, brimonidine 2 times per day both eyes and subcutaneous methotrexate injections 20 mg weekly. He had self-discontinued the cyclopentolate eye drops at some point in the week prior as he did not like the blurred vision and light sensitivity.
The patient’s examination findings were consistent with moderate improvement in the left eye greater than the right eye; however, his IOP had increased to 26 mmHg in each eye, about 10 mmHg higher than his usual IOP. Because of the increased IOP, the brimonidine dosing was increased to 3 times per day in both eyes, and Cosopt® (dorzolamide/timolol) 2 times per day in both eyes was initiated. A slow taper of the oral and topical steroids was started due to the improvement seen in the scleritis and anterior uveitis at this visit. The patient was instructed to return to ophthalmology in about 2 weeks for a pressure check and follow-up.
Optometry, Visit 6
About 2 months after the initial optometry presentation, and 4 weeks after his last ophthalmology examination, the patient returned to our optometry clinic. The patient had missed his most recently scheduled ophthalmology follow-up appointment 2 weeks prior. He reported that his symptoms had significantly improved and that he no longer experienced headaches or eye pain in either eye. He was using Durezol® which was currently being tapered at 2 times per day in the right eye and 1 time per day in the left eye for 1 more week, oral prednisone which was being tapered as well and was down to 20 mg daily for 2 more weeks, brimonidine 3 times per day both eyes and Cosopt® 2 times per day, both eyes. In addition, the patient was using subcutaneous injections of methotrexate with a folic acid supplement to manage the RA. He was due to repeat all blood work in 2 weeks.
Upon examination, his visual acuities were 20/20 in each eye with correction, and extraocular muscle movements, pupils and confrontation field were unremarkable; there was no pain on eye movement. Anterior ocular health evaluation revealed mild injection of the temporal conjunctiva of the right eye, otherwise both eyes were white and quiet. The scarred corneal SEI’s and pannus were stable in both eyes. There was no anterior chamber reaction of either eye. IOP measurements were 17 mmHg in each eye. Dilated posterior ocular health assessment was stable to prior assessments.
Examination findings were communicated with ophthalmology and rheumatology and the patient was scheduled to return to ophthalmology in just over 2 weeks so that the results of his next blood work would be available for that evaluation. The patient was directed to continue the tapering plan as outlined by ophthalmology for both the oral and topical steroids, and to continue the other medications as prescribed. He planned to continue care with ophthalmology and rheumatology and follow up with the optometry clinic for comprehensive care or sooner as directed by the tertiary providers. The patient was educated that he may resume soft contact lens wear, but not to instill ophthalmic eye drops while wearing the lenses. Contact lens infection precautions were reviewed. A timeline of the visits outlined above is available in Figure 3.
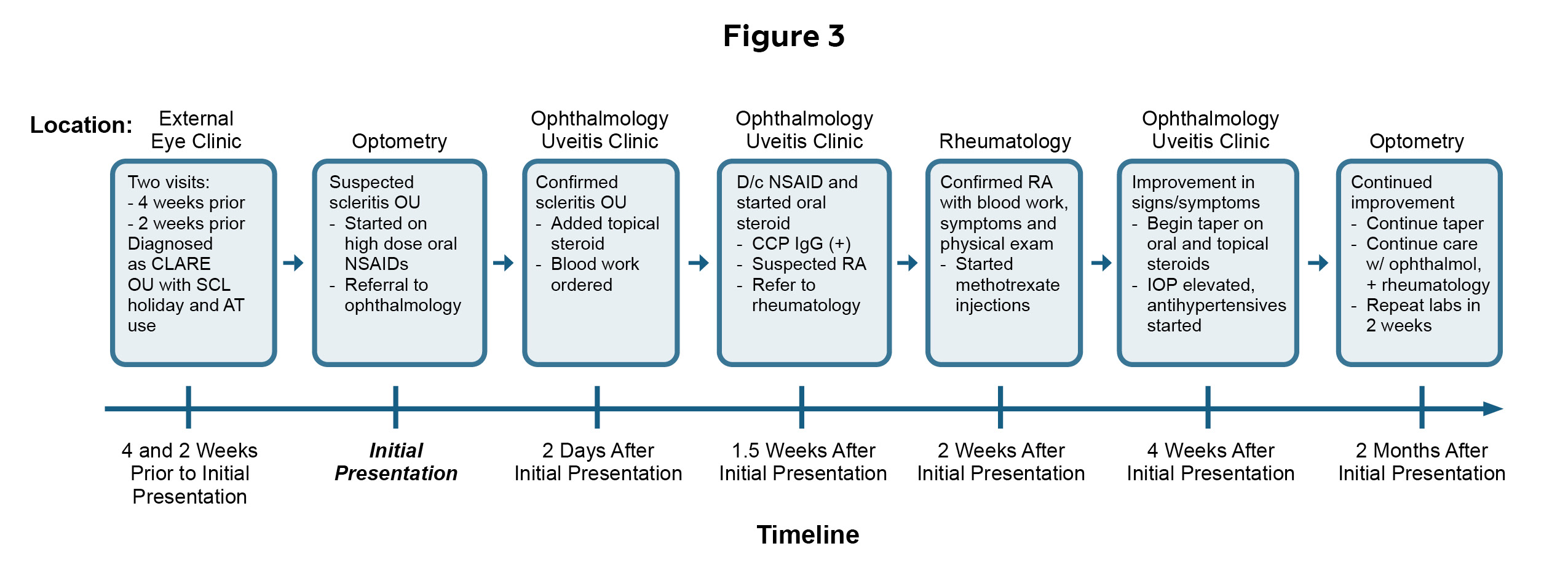
Figure 3. Timeline of visits with the healthcare team who worked together to manage the patient’s condition. *Acronyms: AT = artificial tears, CLARE = contact lens associated red eye, CCP IgG = cyclic citrullinated peptide immunoglobulin G, D/c = discontinue, IOP = intraocular pressure, NSAID = nonsteroidal anti-inflammatory, OD = oculus dexter (right eye), OS = oculus sinister (left eye), OU = oculus uterque (both eyes), RA = rheumatoid arthritis, SCL = soft contact lens. Click to enlarge
Educator’s Guide
Key Concepts
- Ocular manifestations of systemic vasculitides
- Ocular and systemic ancillary testing, imaging and lab work
- Management of ocular disease with high criticality
- Interprofessional care
Learning Objectives
- Describe the characteristic signs and symptoms of scleritis
- Differentiate scleritis from episcleritis or other similar conditions
- Describe the classifications of scleritis and key features of each classification
- Identify systemic conditions associated with scleritis and other potential causes of the condition
- Identify which tests should be performed to confirm or rule out scleritis
- Outline a (co-)management plan for a patient with scleritis and develop a referral letter for interprofessional care
Discussion Questions
Knowledge, understanding and facts about the clinical case and condition presentation
- What is the pathophysiology of scleritis?
- Describe the typical signs and symptoms of scleritis.
- What differentiates non-necrotizing scleritis and necrotizing scleritis?
- Name systemic conditions associated with scleritis.
Differential diagnosis
- What other conditions are on your list of differential diagnoses?
- How can scleritis be differentiated from episcleritis?
- What examination techniques or tests can you utilize to help confirm or rule out a diagnosis of scleritis?
Patient management and role of the optometrist
- What is the typical prognosis of scleritis?
- How would you treat anterior non-necrotizing diffuse scleritis? How would your treatment plan change if the condition was necrotizing?
- How would you communicate your case to other healthcare professionals who may become involved in case management?
Critical-thinking concepts
- If the scleritis is not responding well to the initial treatment, what other tests should be considered? What other therapies should be considered or changed to manage the condition?
Assessment of Learning Objectives
This case may be used in both the didactic classroom or clinical education setting. In the classroom, this case can be presented as part of a lecture on scleritis in an ocular disease course for third- or fourth-year optometry students. Live quiz features during the presentation such as PowerPoint® Polling (PointSolutions, Turning Tech Intermediary, Inc.c) or Zoom Polling (Zoom Video Communications, Inc.d) may assess understanding of key concepts in real time. Knowledge can also be assessed through traditional examination techniques such as multiple choice, “one best answer” or fill in the blank questions based on general knowledge of the condition or through short case-based questions.
In the clinical education setting, this case may be used as part of a journal club presentation or grand rounds discussion. The questions outlined above can be used to facilitate small group discussions about the case and condition.
The recommended approach for this case would be to first review the key concepts, learning objectives and read the discussion questions. Then, read the case presentation and discussion. Finally, answer the discussion questions to satisfy the learning objectives.
Discussion
Epidemiology and Pathophysiology
Scleritis is a rare condition that consists of a painful inflammation of the sclera and potentially other surrounding tissues.1 The sclera itself is the protective shell of the eye comprised of an extracellular matrix. It is innervated by the ciliary nerves, and the extraocular muscles have points of insertion along the scleral shell.5 Anteriorly, the sclera meets with the cornea at the limbus and posteriorly it is continuous with the exception of where it is pierced by the optic nerve. The sclera itself is avascular, but the deep episcleral vascular plexus sits just atop the scleral shell anteriorly while the vortex veins drain posteriorly to the ophthalmic vein. Vasculitis of this deep vascular plexus causes the inflammation and classic deep red appearance associated with scleritis.1 It is thought that the cause of this vasculitis is often due to autoimmune mechanisms including immune complex mediated inflammation.6 Pain on eye movements associated with scleritis is due to the extraocular muscle insertion into the scleral shell which, if inflamed, will cause pain with contraction of the muscles.
Scleritis can be classified by location, diffuse or nodule nature and presence or absence of necrotization. Scleritis can occur anterior to the insertion of the recti muscles (anterior scleritis), posterior to their insertion (posterior scleritis) or both simultaneously. In addition, scleritis can be identified as occurring in a diffuse or nodular form, determined by the presence or absence of an associated nodule. Arguably most important is the ability to classify the scleritis as necrotizing or non-necrotizing as necrotizing scleritis poses an immediate threat to vision and is a true ocular emergency.7 Necrotizing scleritis can occur with inflammation or without inflammation; the form without inflammation is also referred to as scleromalacia perforans. Necrosis in scleritis will appear as a whitening of the conjunctival and scleral tissues associated with capillary non-perfusion and absence or death of the vasculature. Necrotizing scleritis without inflammation is an exception to the typical painful presentation of scleritis because it is a chronic wasting of tissue heavily associated with chronic RA and is often asymptomatic.8 The scleral tissue slowly wastes away over time and the purple uveal tissue will show through. It is often seen coincidentally on an eye examination due to the asymptomatic nature and gradual chronic progression. Scleritis can occur in one eye or both eyes simultaneously. Bilateral scleritis is thought to be more often associated with systemic disease than unilateral presentations.2,9,10
While the cause of scleritis can be due to idiopathic inflammation, up to 40 to 50% of cases are associated with systemic conditions or infection.10-12 As mentioned, it is thought that the vasculitis is immune mediated and possibly caused by immune complex deposition or the upregulation of proinflammatory cytokines. Given this autoimmune pathophysiology, common conditions associated with scleritis include RA, systemic lupus erythematosus (SLE), inflammatory bowel disease (IBD), reactive arthritis, polychondritis, juvenile chronic arthritis and seronegative polyarthritis to name a few.12,13 Granulomatous conditions have also been associated with scleritis including Wegener’s granulomatosis and sarcoidosis. Infections are a less common cause of scleritis than systemic disease, but still must be considered, especially postoperatively. The herpes virus is the most common cause of infectious scleritis.14 Scleritis can occur due to a spillover of an infectious keratitis or can occur due to infection from a retained foreign body or postoperative complications.
Historically, studies have shown that scleritis tends to occur in women more than men and it is thought that this may be due to the higher prevalence of autoimmune conditions in women.15 However, some recent studies in Asia have shown a slight male preponderance.2 Scleritis most often presents in the fourth to sixth decade of life.15
Clinical Presentation and Prognosis
The classic presentation of scleritis is a very painful, red eye with scleral edema. Due to the depth of the vessels involved and the significant vascular dilation, the red appearance is often a deep red to purple color, sometimes called a violaceous hue.5,16 The scleral edema associated with anterior scleritis can be observed in natural light, on careful slit lamp examination and with ASOCT.17-19 If ischemia or necrosis are present, areas of the sclera may appear as a stark white due to the loss of the vasculature in that area. While the deep red appearance is classic with anterior scleritis, posterior scleritis alone (not in conjunction with anterior scleritis) can be harder to discern since the anterior scleral vasculature may not be as obviously inflamed. A careful dilated examination and additional ocular imaging are warranted in cases of suspected posterior scleritis as discussed below.12
Patients with scleritis are often in a significant amount of acute or subacute pain due to the degree of vascular dilation and scleral edema. The pain is often described as a deep boring pain that can be felt in the orbit and surrounding tissues.1 The pain is often worse on eye movements because of the recti muscle insertions into the sclera.
Due to the inflammatory nature of the condition, scleritis may present with associated inflamed ocular tissues including the cornea, ciliary body and trabecular meshwork resulting in keratitis, anterior uveitis and increased intraocular pressure, respectively.1 Anterior uveitis may present in up to 42% of cases of scleritis.10 Posterior scleritis may present with other posterior segment findings including exudative retinal detachment, serous retinal detachment, cystoid macular edema, choroidal effusion syndrome, swollen optic discs, choroidal folds, and retinal vascular occlusion, and therefore a careful dilated fundus examination is warranted.20-22 The vision may be reduced due to these potential findings accompanying the scleritis.
Scleritis is potentially sight threatening and thus must be managed accordingly.1,3,4,23 The type and severity of the condition determines the likelihood of vision loss with moderate to severe and necrotizing disease being more at risk. Scleritis with necrosis has a high risk for globe perforation highlighting the importance of determining the presence or absence of necrosis on ocular examination. It is imperative to determine the underlying cause to accurately treat the condition and reduce the risk of complications and poor visual outcome.
Ancillary Testing and Differential Diagnosis
When scleritis is suspected, certain ocular testing should be performed including: a thorough case history, a review of systems (ROS) to identify potential systemic disease associations, visual acuity, extraocular muscle movements, a thorough slit lamp examination, intraocular pressure measurement and dilated fundus exam.12 Anterior segment photography and ASOCT may be helpful to follow and confirm or rule out a diagnosis of scleritis. ASOCT allows the examiner to observe all layers of the conjunctiva, episclera and sclera and determine the depth and extent of the inflammation.17 If posterior scleritis is suspected, then a B-scan ultrasound should be performed looking for posterior scleral thickening which creates a “T” shape between the sclera and optic nerve known as the “T-sign”.24 OCT with enhanced depth imaging (EDI-OCT) may also be considered for posterior scleritis imaging as posterior segment and choroidal thickness can be assessed.25
In addition to the ocular examination, a complete physical examination should be performed including blood work. Blood work is used to confirm or rule out the presence of causative systemic conditions such as RF and CCP Ab IgG for RA, ANA for SLE, ANCA for Wegener’s granulomatosis and polyarteritis nodosa (PAN), ESR and CRP for giant cell arteritis (GCA), uric acid for gout, CBC for general systemic health and infectious etiology, RPR and FTA-ABS for syphilis, and ACE for sarcoid.12,14 See Table 2 for a more thorough outline of recommended blood work in a scleritis workup and reference ranges. Additional tests may be considered if suspicion for other etiologies exists including purified protein derivative (PPD) for tuberculosis (TB), CXR for TB and sarcoid, Lyme titers for Lyme disease, magnetic resonance imaging (MRI) and computed tomography (CT) to rule out a neoplasm.12 As noted above, systemic disease is a common cause of scleritis and thus blood work is paramount for determining the underlying cause of the condition at presentation.
The differential diagnosis for scleritis should include severe cases of conjunctivitis or episcleritis, and keratitis with spillover to the sclera. One exam technique that allows the examiner to differentiate scleritis from severe cases of conjunctivitis or episcleritis is the use of phenylephrine 2.5% ophthalmic eye drops to induce blanching or whitening of the conjunctival and episcleral vessels. Deeper vessels will not blanch as seen in cases of scleritis and thus the presence of blanching after phenylephrine instillation is consistent with conjunctivitis or episcleritis.26
A careful slit lamp examination can determine the presence of keratitis and associated corneal findings such as ulceration. Scleritis can occur as a result of an infectious keratitis, and infection must be considered if there are corneal findings when a scleritis is present.27 Culturing the ocular tissue would be helpful for this determination. Additionally, corneal findings such as peripheral ulcerative keratitis (PUK) may accompany scleritis more commonly in causative systemic conditions such as Wegener’s granulomatosis; Wegener’s should be considered any time corneal findings present simultaneously with scleritis.28
Less common differentials for scleritis may include infectious orbital disease such as orbital cellulitis and endophthalmitis.29,30 Thorough case history and careful ocular examination can assist in this differentiation, as well as close monitoring of response to treatment. There are also case reports of ocular tumors masquerading as scleritis, highlighting the importance of considering additional imaging.31,32 Ocular tumors must be considered if scleritis is not responding to initial treatment.
Treatment and Management
Treatment for scleritis depends on the causative agent. For diffuse and nodular anterior non-necrotizing and non-infectious disease, high dose oral NSAIDs and oral steroids are considered in first line treatment.32-34 Oral NSAIDs are often tried in sequential order including ibuprofen 400 to 600 mg by mouth 4 times per day, naproxen 250 to 500 mg by mouth twice a day, and indomethacin 25 mg by mouth three times a day, respectively.12 Of note, if prescribing high dose oral NSAIDs, a histamine type 2 receptor blocker or proton pump inhibitor is advised to reduce the likelihood of GI upset. Oral steroid prescribing may include prednisone 60 to 100 mg by mouth daily for 1 week, tapering to 20 mg daily, very slowly over a 2-6 week period, followed by an even slower taper after that. If both oral NSAID and oral steroid therapy are unsuccessful, immunosuppressive agents such as methotrexate, cyclophosphamide, azathioprine and anti-tumor necrosis factor alpha are considered.12 Failure of NSAID and steroid therapy is also indicative of an undetermined underlying cause and additional testing and imaging should be considered if not already performed.
If the scleritis is necrotizing in nature or non-necrotizing but severe, oral NSAIDs are often skipped and oral steroids alone or in combination with immunosuppressive agents are used in the same prescribing dosages as outlined above.12 Necrotizing disease has an increased risk of perforation and thus perforation precautions should be considered including polycarbonate lens protection, a fox shield during sleeping hours and scleral patch grafting depending upon the extent of the scleral thinning.12 Necrotizing disease warrants an urgent/immediate assessment with ophthalmology due to its vision threatening nature.
Due to the high likelihood of associated systemic disease and complex nature of scleritis, the condition is often co-managed by a team of healthcare providers.35 The team may include but is not limited to optometrists, ophthalmologists, primary care providers, rheumatologists, dermatologists and infectious disease experts. Excellent communication and interprofessional care is often required to successfully manage cases of scleritis caused by systemic or infectious disease. The follow-up plan for scleritis depends on the cause and severity of the disease. Close follow-up is recommended until positive clinical response to therapy is seen including reduction of pain and inflammation.12
Because other ocular tissues may be involved in cases of scleritis, the associated findings should be treated accordingly. For example, an associated anterior uveitis may be managed with topical ophthalmic steroids and cycloplegic agents as seen in the clinical case outlined above.12 Of course caution should be exercised if the scleritis is necrotizing in nature and then oral steroids with cycloplegia may be considered instead of topical steroids which have been thought to promote further necrotization. Adverse events from treatment should also be addressed including GI upset from high dose oral NSAIDs, or an increase in IOP from steroid therapy also known as a steroid response. GI upset can be managed with oral histamine type 2 receptor blocker or proton pump inhibitors, while increase in IOP can be managed with IOP lowering agents which are chosen and tailored to the patient at hand.36,37 Considering all aspects of therapeutic treatment including side effects of the drugs prescribed will lead to better overall case management.
Conclusions
Scleritis is a rare ocular condition that is potentially sight threatening and therefore must be identified and managed accordingly. Patients with anterior scleritis typically present with a red eye and high degree of pain. A thorough history, review of systems and ocular and physical examination are required to assess the condition. Examination techniques such as blanching the ocular blood vessels with topical ophthalmic phenylephrine or image acquisition with ASOCT can help differentiate scleritis from other conditions such as severe episcleritis. Differentiating necrotizing and non-necrotizing scleritis is critical because of the fast acting and devastating nature of necrotizing disease. Due to the common association of scleritis with systemic disease, determining the underlying cause for the condition is paramount as it will direct proper treatment. Blood work and additional imaging are often ordered and needed to determine the underlying cause.
Scleritis cases are managed with therapeutics including oral NSAIDs, oral steroids and immunosuppressive agents that are selected based upon the presentation and nature of the case at hand. Close follow-up is warranted until a positive clinical response to therapy is observed. Management of scleritis is often complex with disease co-management and excellent interprofessional communication being key to proper case management.
This case outlined a bilateral anterior non-necrotizing diffuse scleritis due to an underlying systemic disease, rheumatoid arthritis. ASOCT was helpful in confirming the suspected condition, and blood work was key to determining the underlying cause. The usual course of scleritis management was exercised in this case by first using high dose oral NSAIDs, followed by oral steroids and finally, immunosuppressive therapy with methotrexate as indicated by the RA diagnosis. This case also demonstrated the importance of managing side effects of treatment including GI upset from high dose oral NSAIDs and IOP reduction due to topical steroid response. Co-management and communication with ophthalmology and rheumatology were crucial to the successful diagnosis and management of this case.
References
- Okhravi N, Odufuwa B, McCluskey P, Lightman S. Scleritis. Surv Ophthalmol. 2005 Jul-Aug;50(4):351-63. DOI: 1016/j.survophthal.2005.04.001
- Lane J, Nyugen E, Morrison J, et al. Clinical features of scleritis across the Asia-Pacific region. Ocul Immunol Inflamm. 2019;27(6):920-6. DOI: 1080/09273948.2018.1484496
- Sims J. Scleritis: presentations, disease associations and management. Postgrad Med J. 2012 Dec;88(1046):713-8. DOI: 1136/postgradmedj-2011-130282
- Majumder PD, Agrawal R, McCluskey P, Biswas J. Current approach for the diagnosis and management of noninfective scleritis. Asia Pac J Ophthalmol (Phila). 2020 Dec 7;10(2):212-23. DOI: 1097/APO.0000000000000341
- Remington L, Goodwin D. Cornea and sclera. In: Clinical anatomy and physiology of the visual system. 4th ed. Elsevier; 2021. pp 10-39.
- Fong LP, de la Maza MS, Rice BA, Kupferman AE, Foster CS. Immunopathology of scleritis. Ophthalmology. 1991 Apr;98(4):472-9. DOI: 1016/s0161-6420(91)32280-2
- Watson PG, Hayreh SS. Scleritis and episcleritis. Br J Ophthalmol.1976 Mar;60(3):163-91. DOI: 1136/bjo.60.3.163
- Kopacz D, Maciejewicz P, Kopacz M. Scleromalacia perforans–What we know and what we can do. J Clinic Experiment Ophthalmol. 2013:S2. DOI: 4172/2155-9570-S2-009
- de la Maza MS, Molina N, Gonzalez-Gonzalez LA, Doctor PP, Tauber J, Foster CS. Clinical characteristics of a large cohort of patients with scleritis and episcleritis. Ophthalmology. 2012 Jan;119(1):43-50. DOI: 1016/j.ophtha.2011.07.013
- de la Maza MS, Jabbur NS, Foster CS. Severity of scleritis and episcleritis. Ophthalmology. 1994 Feb;101(2):389-96. DOI: 1016/s0161-6420(94)31325-x
- Akpek EK, Thorne JE, Qazi FA, Do DV, Jabs DA. Evaluation of patients with scleritis for systemic disease. Ophthalmology. 2004 Mar;111(3):501-6. DOI: 1016/j.ophtha.2003.06.006
- Gerstenblith AT, Rabinowitz MP. Conjunctiva/Sclera/Iris/External Disease. In: The Wills Eye Manual. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. pp 122-124.
- Pavesio CE, Meier FM. Systemic disorders associated with episcleritis and scleritis. Curr Opin Ophthalmol. 2001 Dec;12(6):471-8. DOI: 1097/00055735-200112000-00013
- Gonzalez-Gonzalez LA, Molina-Prat N, Doctor P, Tauber J, de la Maza MT, Foster CS. Clinical features and presentation of infectious scleritis from herpes viruses: a report of 35 cases. Ophthalmology. 2012 Jul;119(7):1460-4. DOI: 1016/j.ophtha.2012.01.033
- Honik G, Wong IG, Gritz DC. Incidence and prevalence of episcleritis and scleritis in Northern California. Cornea. 2013 Dec;32(12):1562-1566. DOI: 1097/ICO.0b013e3182a407c3
- Galor A, Thorne JE. Scleritis and peripheral ulcerative keratitis. Rheum Dis Clin North Am. 2007 Nov;33(4):835-54, vii. DOI: 1016/j.rdc.2007.08.002
- Shoughy SS, Jaroudi MO, Kozak I, Tabbara KF. Optical coherence tomography in the diagnosis of scleritis and episcleritis. Am J Ophthalmol. 2015 Jun;159(6):1045-9.e1. DOI: 1016/j.ajo.2015.03.004
- Axmann S, Ebneter A, Zinkernagel MS. Imaging of the sclera in patients with scleritis and episcleritis using anterior segment optical coherence tomography. Ocul Immunol Inflamm. 2016;24(1):29-34. DOI: 3109/09273948.2015.1025983
- Levison AL, Lowder CY, Baynes KM, Kaiser PK, Srivastava SK. Anterior segment spectral domain optical coherence tomography imaging of patients with anterior scleritis. Int Ophthalmol. 2016 Aug;36(4):499-508. DOI: 1007/s10792-015-0153-8
- McCluskey PJ, Watson PG, Lightman S, Haybittle J, Restori M, Branley M. Posterior scleritis: clinical features, systemic associations, and outcome in a large series of patients. Ophthalmology. 1999 Dec;106(12):2380-6. DOI: 1016/S0161-6420(99)90543-2
- Gonzalez-Gonzalez LA, Molina-Prat N, Doctor P, Tauber J, Sainz de la Maza M, Foster CS. Clinical features and presentation of posterior scleritis: a report of 31 cases. Ocul Immunol Inflamm. 2014 Jun;22(3):203-7. DOI: 3109/09273948.2013.840385
- Lavric A, Gonzalez-Lopez JJ, Majumder PD, et al. Posterior scleritis: analysis of epidemiology, clinical factors, and risk of recurrence in a cohort of 114 patients. Ocul Immunol Inflamm. 2016;24(1):6-15. DOI: 3109/09273948.2015.1005240
- Wieringa WG, Wieringa JE, ten Dam-van Loon NH, Los LI. Visual outcome, treatment results, and prognostic factors in patients with scleritis. Ophthalmology. 2013 Feb;120(2):379-86. DOI: 1016/j.ophtha.2012.08.005
- Maleki A, Ruggeri M, Colombo A, et al. B-scan ultrasonography findings in unilateral posterior scleritis. J Curr Ophthalmol. 2022 Apr 16;34(1):93-9. DOI: 4103/joco.joco_267_21
- Hirukawa K, Keino H, Watanabe T, Okada AA. Enhanced depth imaging optical coherence tomography of the choroid in new-onset acute posterior scleritis. Graefes Arch Clin Exp Ophthalmol. 2013 Sep;251(9):2273-5. DOI: 1007/s00417-013-2265-z
- Diaz JD, Sobol EK, Gritz DC. Treatment and management of scleral disorders. Surv Ophthalmol. 2016 Nov-Dec;61(6):702-17. DOI: 1016/j.survophthal.2016.06.002
- Reynolds MG, Alfonso E. Treatment of infectious scleritis and keratoscleritis. Am J Ophthalmol. 1991 Nov 15;112(5):543-7. DOI: 1016/s0002-9394(14)76856-4
- Tarabishy AB, Schulte M, Papaliodis GN, Hoffman GS. Wegener’s granulomatosis: clinical manifestations, differential diagnosis, and management of ocular and systemic disease. Surv Ophthalmol. 2010 Sep-Oct;55(5):429-44. DOI: 1016/j.survophthal.2009.12.003
- Rossiter‐Thornton M, Rossiter‐Thornton L, Ghabrial R, Azar DA. Posterior scleritis mimicking orbital cellulitis. Med J Aus. 2010 Sep 6;193(5):305-6. DOI: 5694/j.1326-5377.2010.tb03915.x
- Murthy SI, Sati A, Sangwan V. Infectious scleritis mimicking severe ocular inflammation: atypical initial presentation. BMJ Case Rep. 2013 Feb 20:2013:bcr2013008686. DOI: 1136/bcr-2013-008686
- Kaliki S, Freitag SK, Chodosh J. Nodulo-ulcerative ocular surface squamous neoplasia in 6 patients: a rare presentation. Cornea. 2017 Mar;36(3):322-6. DOI: 1097/ICO.0000000000001031
- Kafkala C, Daoud YJ, Paredes I, Foster CS. Masquerade scleritis. Ocul Immunol Inflamm. 2005 Dec;13(6):479-82. DOI: 1080/09273940591004133
- Rachitskaya A, Mandelcorn ED, Albini TA. An update on the cause and treatment of scleritis. Curr Opin Ophthalmol. 2010 Nov;21(6):463-7. DOI: 1097/ICU.0b013e32833f1060
- de la Maza MS, Molina N, Gonzalez-Gonzalez LA, Doctor PP, Tauber J, Foster CS. Clinical characteristics of a large cohort of patients with scleritis and episcleritis. Ophthalmology. 2012 Jan;119(1):43-50. DOI: 1016/j.ophtha.2011.07.013
- Castells DD. Anterior scleritis: three case reports and a review of the literature. Optometry. 2004 Jul;75(7):430-44. DOI: 1016/s1529-1839(04)70158-x
- Tuskey A, Peura D. The use of H2 antagonists in treating and preventing NSAID-induced mucosal damage. Arthritis Res Ther. 2013;15 Suppl 3(Suppl 3):S6. DOI: 1186/ar4178
- Razeghinejad MR, Katz LJ. Steroid-induced iatrogenic glaucoma. Ophthalmic Res. 2012;47(2):66-80. DOI: 1159/000328630
Footnotes
- Canon EOS Rebel T7, Canon USA, Inc.
- Spectralis OCT, Heidelberg Engineering
- PowerPoint® Polling, PointSolutions, Turning Tech Intermediary, Inc.
- Zoom Polling, Zoom Video Communications, Inc.

